Cannabis consumption has increased substantially in recent years, driven by expanding legalization, shifting societal attitudes, and the widespread availability of high-potency formulations. According to data from the Centers for Disease Control and Prevention (CDC), cannabis remains the most commonly used federally illegal substance in the United States, with approximately 22% of individuals aged 12 years and older reporting past-year use.1 Epidemiologic studies further suggest that nearly 30% of individuals who use cannabis may meet diagnostic criteria for cannabis use disorder (CUD), with increased risk associated with earlier initiation, higher frequency of use, and greater tetrahydrocannabinol (THC) exposure.2
Although cannabis use is often perceived as relatively benign, its pharmacologic effects extend across multiple organ systems through activation of the endocannabinoid system. Of relevance to oral health, cannabinoid receptors are expressed in immune cells, bone tissue, and oral mucosa, suggesting potential effects on inflammatory response, wound healing, and bone metabolism. These biologic processes are critical determinants of successful dental implant therapy, including osseointegration and long-term peri-implant tissue stability.
Despite the growing prevalence of cannabis use among adults—particularly within age groups most likely to seek implant rehabilitation—its implications in implant dentistry remain underrecognized and insufficiently characterized. Emerging evidence indicates that cannabis use may be associated with altered immune function, impaired wound healing, and changes in bone biology, all of which may influence peri-implant health and implant success.3 However, existing data are limited, heterogeneous, and often extrapolated from non-dental models.
The purpose of this narrative review is to examine the current evidence regarding the potential effects of cannabis use on dental implant therapy. Specifically, this review aims to summarize relevant biologic mechanisms, evaluate available clinical and preclinical data, and provide practical considerations for risk assessment, patient counseling, and treatment planning in implant dentistry.
Mechanism of Action:
The principal psychoactive constituent of cannabis, Δ9 -tetrahydrocannabinol (THC), exerts its effects primarily through activation of cannabinoid receptors type 1 (CB1) and type 2 (CB2). CB1 receptors are abundantly expressed within the central nervous system and are largely responsible for the psychoactive effects of THC, whereas CB2 receptors are predominantly associated with immune modulation and are expressed in immune cells, bone tissue, and peripheral organs, including the vasculature.
THC produces rapid and predictable psychoactive effects, which contribute to its widespread use for perceived benefits such as relaxation, stress reduction, euphoria, and analgesia. However, activation of the endocannabinoid system also influences inflammatory pathways, immune cell function, vascular tone, and bone metabolism—biologic processes directly relevant to wound healing and osseointegration in dental implant therapy.
Although cannabis use is frequently perceived as “natural” or safer than alcohol or prescription medications, contemporary cannabis products contain substantially higher concentrations of THC than historically encountered. As a result, physiologic and clinical effects may vary considerably and are influenced by dose, frequency of use, route of administration, and individual susceptibility. These factors complicate risk assessment and underscore the need for careful consideration of cannabis use in patients undergoing implant-related surgical procedures.4,5
Mode of Administration:
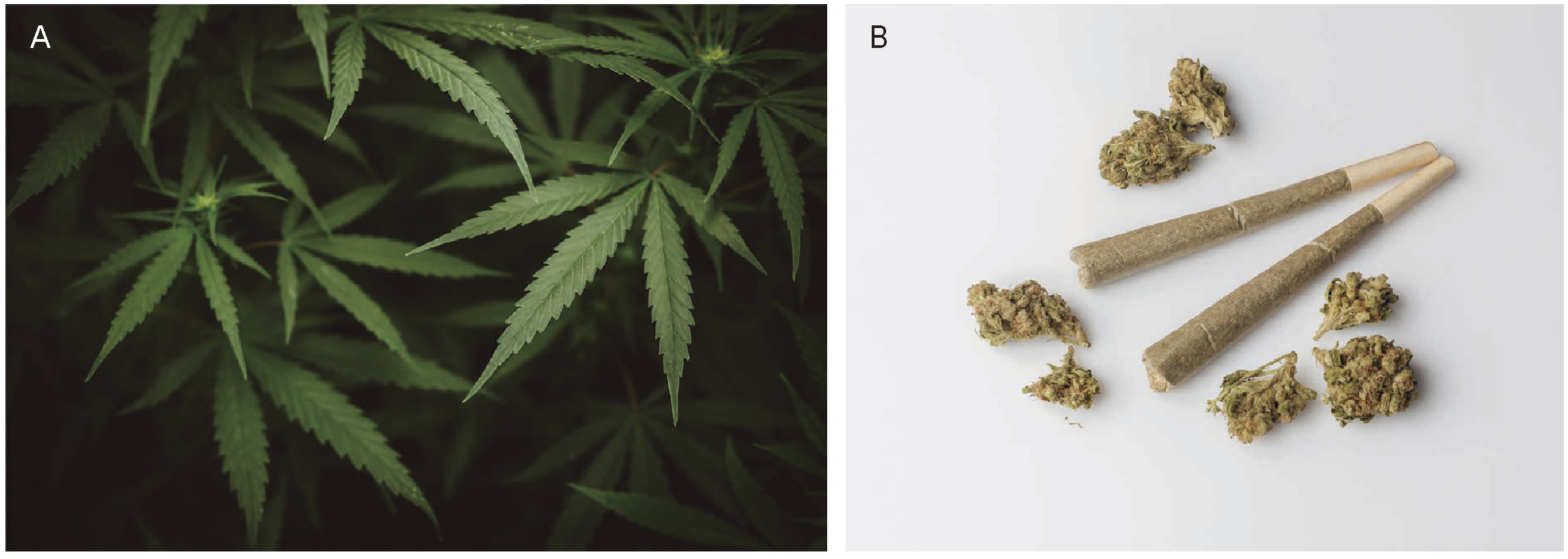
Cannabis may be administered through multiple routes, each associated with distinct pharmacokinetic characteristics, patterns of systemic exposure, and local tissue interactions that may influence peri-implant wound healing and osseointegration. Variations in route of administration affect the rate and extent of cannabinoid absorption, peak plasma concentrations, duration of biologic activity, and metabolic pathways, all of which may alter immune response, vascular dynamics, and bone remodeling. In addition, certain delivery methods involve direct exposure of the oral and peri-oral tissues to physical, thermal, or chemical insults, whereas others primarily exert systemic effects. As a result, the route of cannabis administration represents an important, yet often underappreciated, variable when evaluating potential risks associated with implant surgery and peri-implant tissue stability.6 (Figure 1) The following are the most common routes of administration.
Inhalation methods—including smoking, vaping, and dabbing—result in rapid systemic absorption and higher peak plasma concentrations of Δ9-tetrahydrocannabinol (THC). However, these routes also expose oral and peri-oral tissues to thermal injury, combustion byproducts, particulate matter, and, in some cases, residual solvents, which may contribute to mucosal irritation, local vasoconstriction, and impaired soft-tissue healing.
Oral routes of administration, such as edibles, capsules, and oils, are characterized by delayed onset and prolonged systemic effects due to gastrointestinal absorption and hepatic first-pass metabolism. These methods are generally associated with minimal direct exposure of oral tissues but may still exert systemic effects on immune response, inflammation, and bone metabolism that are relevant to implant healing.
Oromucosal and sublingual delivery systems, including sprays and tinctures, provide more rapid absorption than oral ingestion without the thermal and combustion-related insults associated with inhalation. While local mucosal exposure occurs, these methods may result in less tissue irritation compared with smoking or vaping.
Recognition of the route of cannabis administration is clinically important, as differences in delivery method, frequency of use, and cannabinoid composition (THC-dominant versus cannabidiol-predominant formulations) may differentially affect systemic physiology and the local peri-implant environment essential for predictable osseointegration and long-term soft-tissue stability.7
(Fig.1) Cannabis plant and inhaled cannabis products.
(A) Cannabis sativa leaves representing the source plant from which medical and recreational cannabis products are derived.
(B) Examples of inhaled cannabis forms, including rolled joints and dried cannabis flower, which expose the oral cavity and peri-implant tissues to heat, combustion byproducts, and concentrated cannabinoids that may influence oral inflammation and peri-implant health.
Dental Implant Implications:
The use of cannabis can directly affect the dental implant therapy via the following pathways:
1. Thermal and Chemical Injury
Inhalation of combusted cannabis exposes the oral cavity and peri-implant tissues to a complex mixture of irritants and toxic byproducts, including carbon monoxide, tar, volatile organic compounds, and polycyclic aromatic hydrocarbons—many of which mirror those found in tobacco smoke.8 These substances exert direct cytotoxic and pro-inflammatory effects on oral mucosa, impairing the function of fibroblasts and epithelial cells that are essential for soft-tissue repair and wound closure. Exposure to these compounds increases oxidative stress, disrupts collagen synthesis and deposition, and interferes with the formation of a stable soft-tissue seal surrounding dental implants. Such alterations compromise early mucosal healing and may predispose peri-implant tissues to bacterial invasion.9
Preclinical animal studies suggest that chronic cannabis smoke exposure reduces bone-to-implant contact and diminishes peri-implant bone fill, indicating impairment of the osseointegration process. These findings suggest that the thermal and chemical components of cannabis smoke may weaken implant anchorage and increase susceptibility to early biomechanical failure, underscoring the importance of addressing inhalation habits in patients undergoing implant therapy.10
2. Oral Microbiome Alterations
Cannabis use has been increasingly associated with measurable alterations in the oral microbiome, with several studies demonstrating a shift toward microbial communities associated with periodontal and peri-implant disease. Regular exposure to cannabinoids—particularly via inhalation—appears to promote the colonization and proliferation of pathogenic species such as Porphyromonas gingivalis, Tannerella forsythia, and other anaerobic Gram-negative organisms implicated in peri-implant mucosal inflammation and alveolar bone loss.11 These microbial changes may be driven in part by THC-related xerostomia, altered salivary composition, and changes in mucosal immunity, all of which create an ecological niche favorable to dysbiosis. Compounding this effect, cannabis-associated immunomodulation—characterized by reduced neutrophil function, altered macrophage activation, and suppression of key inflammatory signaling pathways—further diminishes the host’s ability to control pathogenic biofilm formation. The convergence of microbial dysbiosis and impaired immune surveillance establishes a biologic environment conducive to peri-implant mucositis and the progression to peri-implantitis, thereby posing a significant risk to long-term implant stability.12
3. Xerostomia and Altered Salivary Function
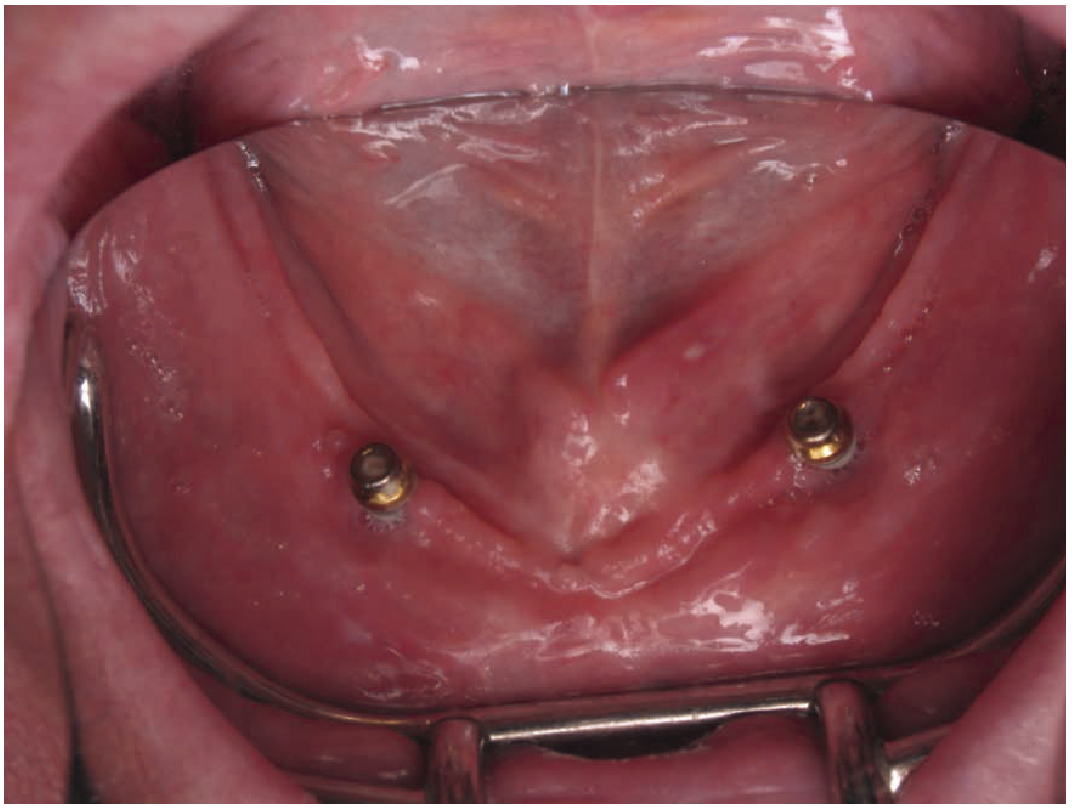
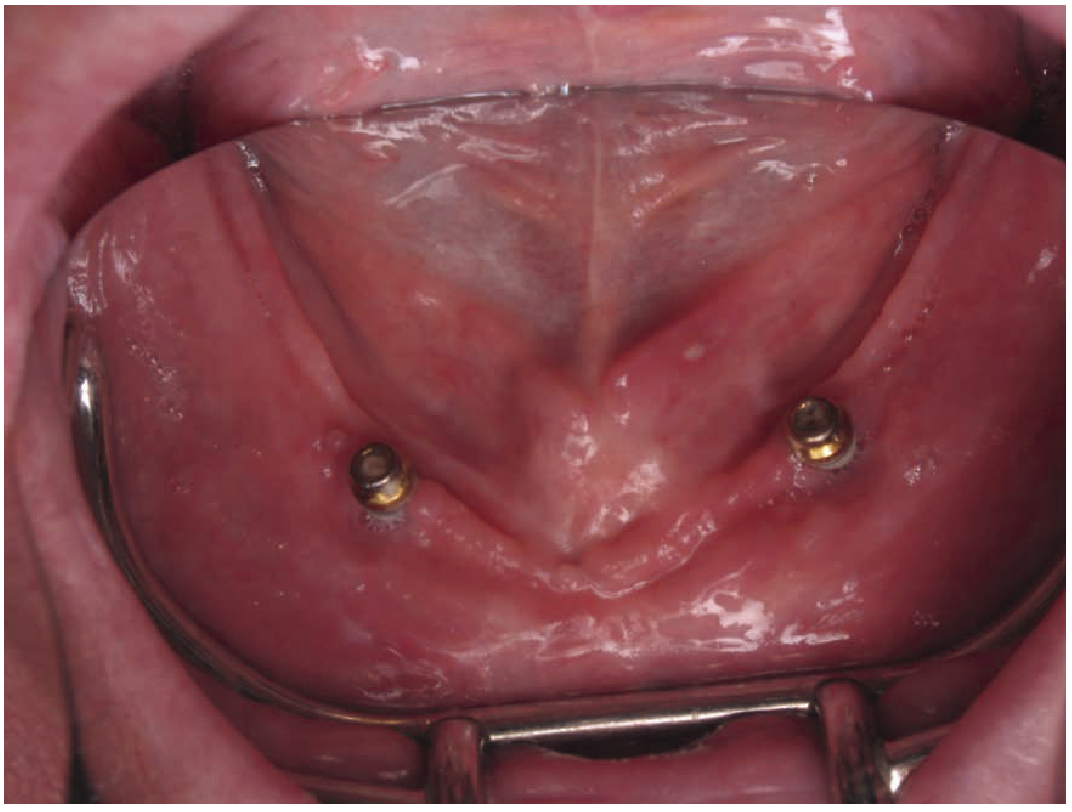
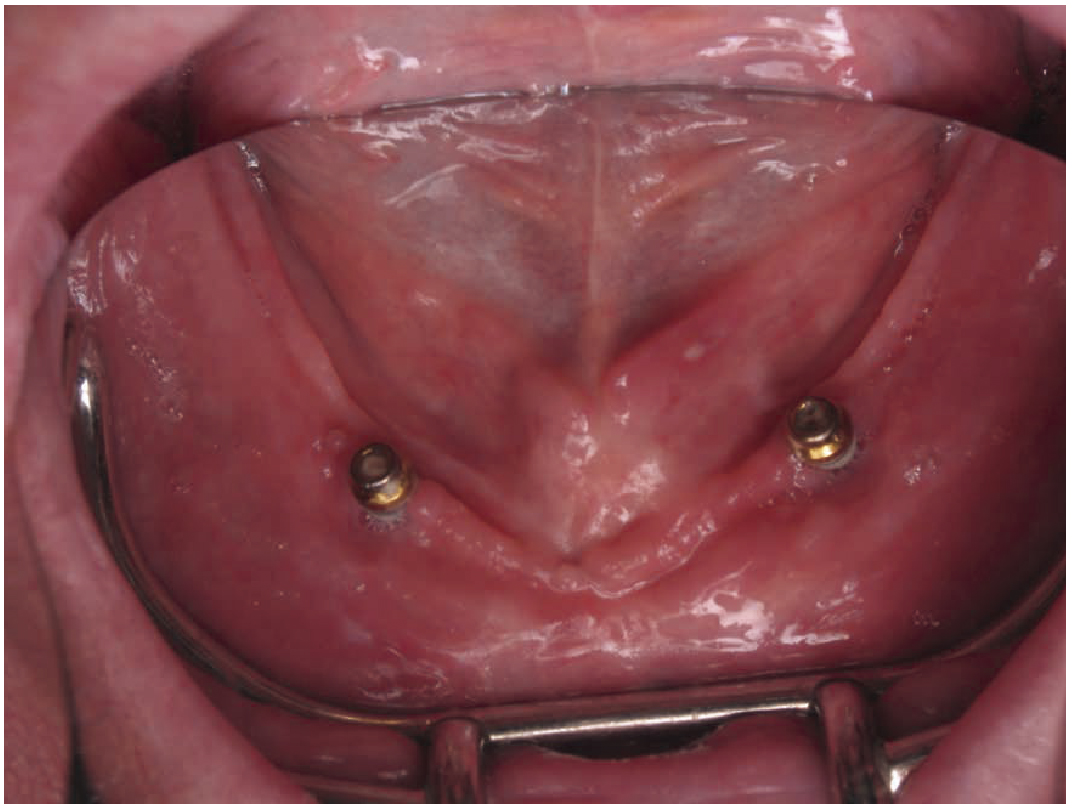
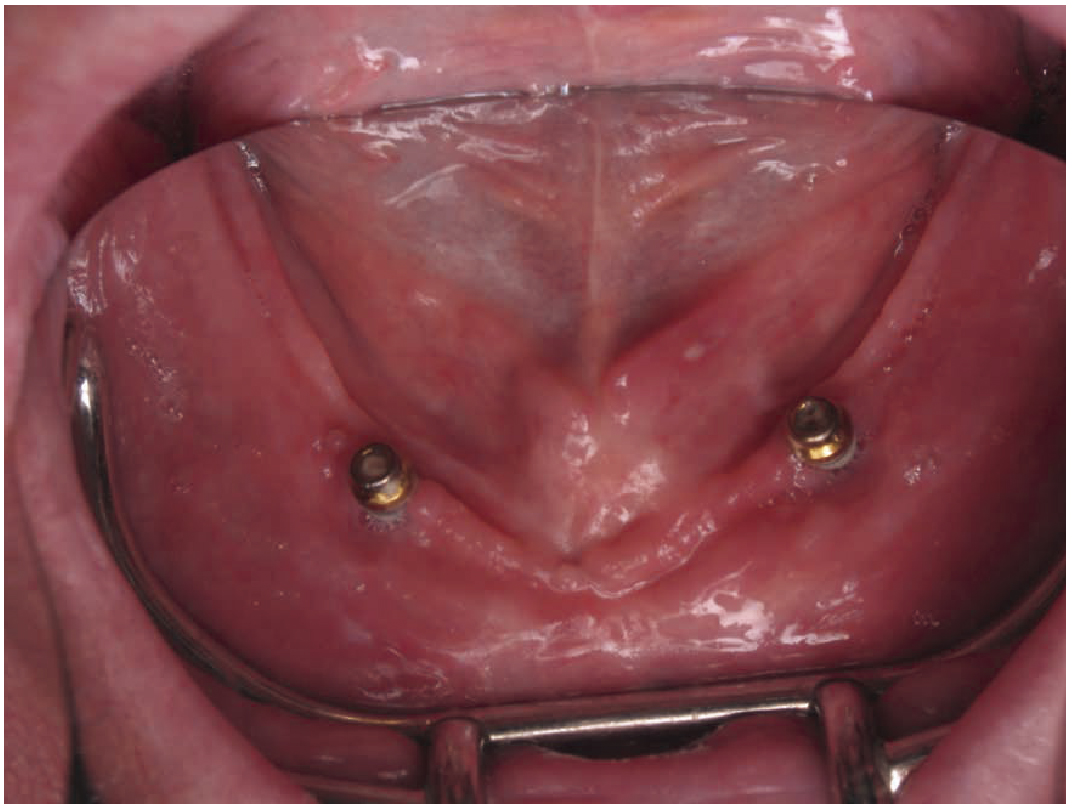
Cannabis use, particularly products high in Δ9- tetrahydrocannabinol (THC), has been shown to reduce salivary flow through inhibition of parasympathetic stimulation of the major salivary glands. This THC-induced xerostomia disrupts the protective functions of saliva, including mechanical cleansing, buffering capacity, and antimicrobial activity. Diminished salivary output results in increased oral bacterial load and facilitates the accumulation of dental plaque, creating a microenvironment that favors the proliferation and maturation of pathogenic peri-implant biofilms.13,14 These microbial shifts are clinically significant, as the biofilms associated with low-saliva conditions are more likely to harbor peri-implant pathogens capable of initiating or exacerbating mucosal inflammation. Over time, this altered microbial ecology contributes to soft-tissue inflammation, marginal bone loss, and accelerated peri-implant tissue breakdown, thereby undermining the long-term stability of dental implants. (Figure 2)
(Fig.2) Xerostomia in a patient with reported regular THC use, demonstrating diminished salivary pooling and dry oral mucosa. THC-associated salivary hypofunction may impair oral defense mechanisms and increase risk for periodontal and peri-implant disease.
4. Gingival Enlargement
Several investigators have reported an association between chronic cannabis use and gingival enlargement. Baddour et. al. first described gingival overgrowth in individuals with prolonged marijuana exposure, suggesting a potential relationship independent of plaque-induced inflammation.15 Rawal et al. reported similar findings, noting a characteristic rugged or nodular gingival appearance without evidence of clinical attachment loss in chronic cannabis users.16
In contrast, Momen-Heravi et al. described a case of chronic cannabis abuse associated with moderate to severe periodontal attachment loss accompanied by peripheral gingival enlargement, most pronounced in the anterior mandible.17 These findings suggest that gingival changes observed in cannabis users may vary in severity and clinical presentation, potentially influenced by duration of use, frequency of exposure, oral hygiene status, and concomitant risk factors.
Although the underlying mechanisms remain incompletely understood, proposed explanations include cannabinoid-mediated alterations in immune response, inflammatory regulation, and gingival fibroblast activity. Collectively, these reports highlight the need for heightened clinical awareness of gingival changes in patients with chronic cannabis use, particularly in the context of periodontal and implant therapy.
5. Periodontal and Peri-Implant Disease
A growing body of epidemiologic and experimental research provides biologically plausible and clinically relevant evidence linking cannabis use to adverse periodontal and peri-implant outcomes.18 Population-based studies consistently demonstrate that individuals who use cannabis exhibit higher prevalence and severity of periodontal disease, including increased clinical attachment loss, greater probing depths, and accelerated alveolar bone destruction, even after controlling for established confounders such as tobacco use, alcohol consumption, and socioeconomic status. Heavy or chronic cannabis use appears to further amplify these effects, with affected individuals demonstrating more pronounced gingival inflammation and deeper periodontal pockets, suggesting a potential dose-response relationship.19,20
Complementing these clinical observations, experimental and animal models have shown that exposure to cannabis smoke adversely affects critical phases of bone healing. Specifically, cannabis exposure has been associated with reduced bone fill, diminished bone volume, and decreased bone-to-implant contact during osseointegration. These findings provide biologic plausibility for compromised implant healing and raise concern for both early and late implant failure.
Beyond its association with periodontal destruction, cannabis use may also contribute to marginal bone loss around dental implants. Emerging evidence suggests that cannabinoids and cannabis smoke exposure can disrupt normal bone remodeling by altering osteoblast and osteoclast activity, impairing angiogenesis, and modulating inflammatory signaling pathways essential for peri-implant bone maintenance. Experimental studies have demonstrated decreased bone formation, reduced bone density, and compromised bone-to-implant contact in the presence of cannabis smoke exposure.21 Additionally, chronic cannabis use may indirectly exacerbate peri-implant bone loss through immune dysregulation, increased pro-inflammatory cytokine expression, and microbial shifts within the peri-implant sulcus.22
Although clinical data specifically evaluating implant marginal bone loss in cannabis-using patients remain limited, the convergence of epidemiologic findings, experimental data, and biologic mechanisms provides a compelling rationale for heightened concern. Collectively, these data suggest that cannabis use—through immune modulation, vascular effects, microbial dysbiosis, and potential cytotoxicity—may compromise both natural periodontal tissues and the biologic environment necessary for predictable osseointegration and long-term peri-implant stability, particularly in patients with heavy or long-term exposure.23 (Figure 3)
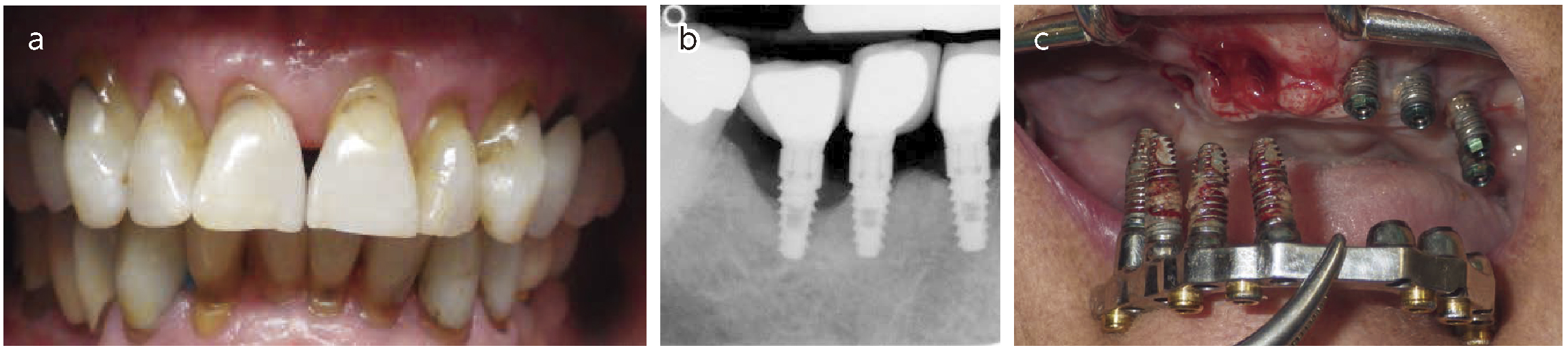
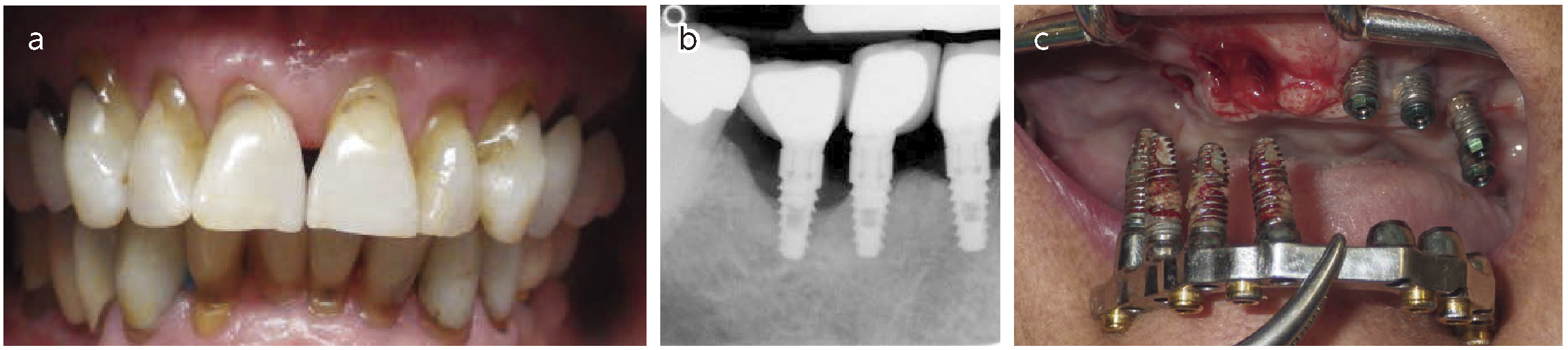
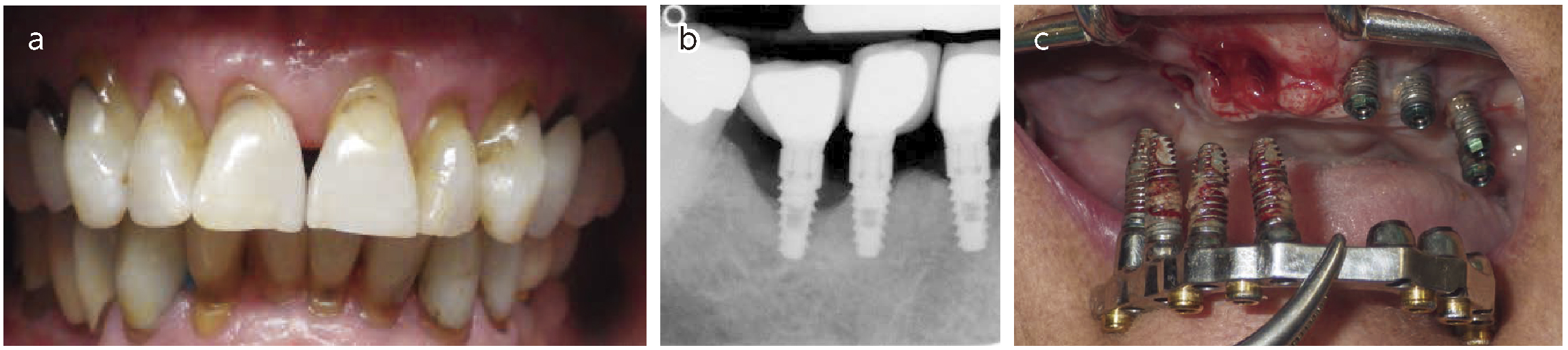
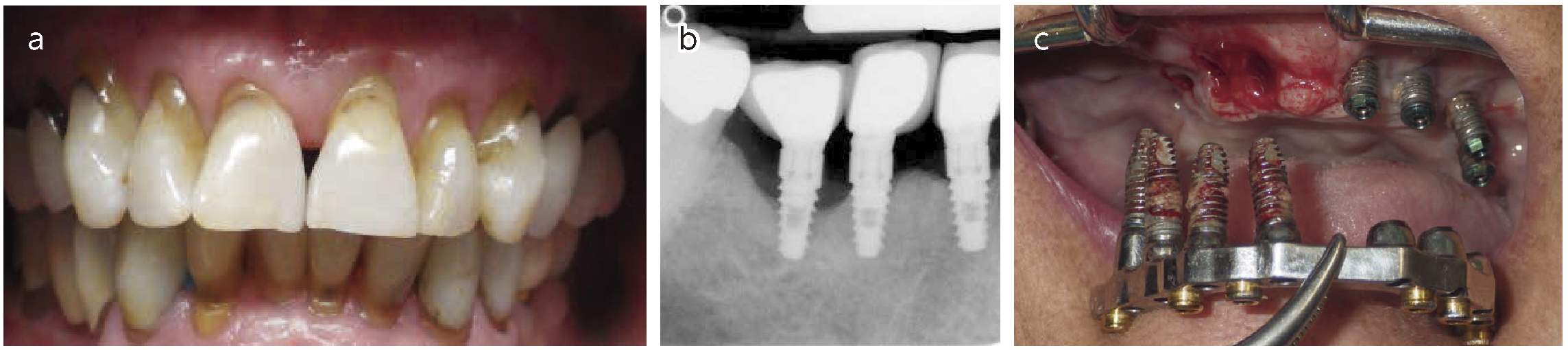
(Fig.3)
(a) Clinical photograph demonstrating advanced periodontal disease affecting the natural dentition, characterized by gingival inflammation, attachment loss, and alveolar bone destruction. Periodontal disease in cannabis users has been consistently reported in epidemiologic studies and is supported by biologic mechanisms including altered immune response, xerostomia, and microbial dysbiosis.
(b, c) Clinical images demonstrating peri-implant mucosal inflammation and peri-implant bone loss in patients with a history of chronic tetrahydrocannabinol (THC) use. While cannabis has documented adverse effects on periodontal tissues, emerging evidence suggests that its biologic impact may be particularly relevant to peri-implant tissues, where immune modulation, impaired wound healing, and altered bone remodeling may increase susceptibility to peri-implant disease
6. Effects on Anesthesia and Analgesia
Cannabis use has important implications for perioperative management in dental settings.
Sedation: Cannabis use has been associated with increased anesthetic requirements in both dental and surgical settings. A recent meta-analysis reported that individuals who use cannabis required an average of 47.33 mg more propofol than non-users, with patients undergoing general anesthesia requiring an additional 30.57 mg compared with controls. These findings suggest clinically meaningful differences in anesthetic dosing requirements among cannabis users.24
In the ambulatory oral and maxillofacial surgery setting, cannabis users have similarly been shown to require significantly higher doses of multiple anesthetic agents. Specifically, cannabis users received greater amounts of propofol (152.5mg vs 117.5mg), midazolam (5.1mg vs 4.7mg), ketamine (46.1mg vs 40.2mg), and fentanyl (88.6µg vs 75.2µg) compared with non-users.25
Cannabis may also interact with benzodiazepines, sedatives, and other centrally acting agents, resulting in unpredictable levels of sedation, delayed recovery, or enhanced respiratory depression when used concomitantly. In addition, perioperative cannabis exposure—particularly recent inhalation of high-THC products—has been associated with tachycardia, blood pressure variability, heightened anxiety, dysphoria, and altered pain perception in the postoperative period.26,27,28
The need for increased anesthetic dosing in cannabis users is thought to be multifactorial and may relate to cannabinoid-induced alterations in central nervous system receptor sensitivity, pharmacodynamic tolerance, and interactions with γ-aminobutyric acid (GABA), N-methyl-D-aspartate (NMDA), and opioid receptor pathways. From a clinical perspective, these findings underscore the importance of preoperative screening for cannabis use and heightened vigilance during sedation and anesthesia planning in dental implant and oral surgical procedures.
Analgesia: Available clinical and experimental evidence indicates that cannabis use is associated with higher postoperative pain scores and increased opioid requirements compared with non-users, suggesting diminished opioid analgesic efficacy in this population. Systematic reviews and randomized controlled trials have not consistently demonstrated consistent opioid-sparing effects of cannabinoids in the acute postoperative setting and, in some cases, have reported attenuation of opioid-mediated analgesia.29,30
In addition to concerns regarding analgesic effectiveness, concomitant use of cannabinoids and opioids has been associated with an increased risk of perioperative adverse effects, including hemodynamic instability and additive central nervous system depression. Although severe respiratory depression has not been consistently observed, the variability in patient response and the potential for pharmacodynamic interactions warrant careful clinical consideration.31,32
Given these findings, clinicians should exercise significant caution when prescribing or administering opioids to patients who use cannabis, particularly those with chronic or heavy exposure. Preoperative screening for cannabis use, individualized analgesic planning, and heightened postoperative monitoring are recommended to mitigate potential risks. At present, evidence is insufficient to support routine opioid dose escalation or reduction in this population, underscoring the need for judicious, closely monitored opioid use and consideration of multimodal analgesic strategies.33,34
Alternative Cannabis Forms: Edibles
Although edible cannabis products do not expose the oral cavity to the thermal or chemical irritants associated with smoked or vaporized cannabis, their systemic pharmacologic effects may still be relevant to peri-implant healing. Oral ingestion of cannabis results in delayed onset but prolonged elevations in circulating Δ9-tetrahydrocannabinol (THC) levels due to gastrointestinal absorption and hepatic first-pass metabolism. This extended systemic exposure may amplify or prolong cannabinoid-mediated effects on immune function, inflammatory signaling, and vascular regulation.35
While these effects have not been specifically evaluated in dental implant populations, they are biologically relevant given the essential roles of immune surveillance, angiogenesis, and microvascular integrity in early osseointegration and soft-tissue healing. Prolonged systemic cannabinoid exposure may therefore have indirect implications for peri-implant tissue stability, particularly in patients with frequent or high-dose edible use.36
In addition, many commercially available edible cannabis products contain high levels of fermentable carbohydrates, which may contribute to increased plaque accumulation and cariogenic biofilm formation. In susceptible individuals, this may indirectly increase the risk of peri-implant mucosal inflammation and compromise long-term peri-implant health.37
Although direct clinical evidence linking edible cannabis use to adverse implant outcomes is currently lacking, these mechanistic considerations support the inclusion of edible cannabis consumption in comprehensive patient histories. Clinicians should incorporate this information into individualized risk assessment, patient counseling, and postoperative maintenance protocols. (Figure 4)
(Fig.4) Cannabis edibles do not expose the oral cavity to heat or chemical irritants but produce delayed and prolonged systemic THC exposure, which may influence immune response, inflammation, and vascular regulation relevant to peri-implant healing. Additionally, the high sugar content of many edibles may increase plaque accumulation and indirectly contribute to peri-implant mucosal inflammation.
Clinical Recommendations for Implant Providers
1. Comprehensive History Taking
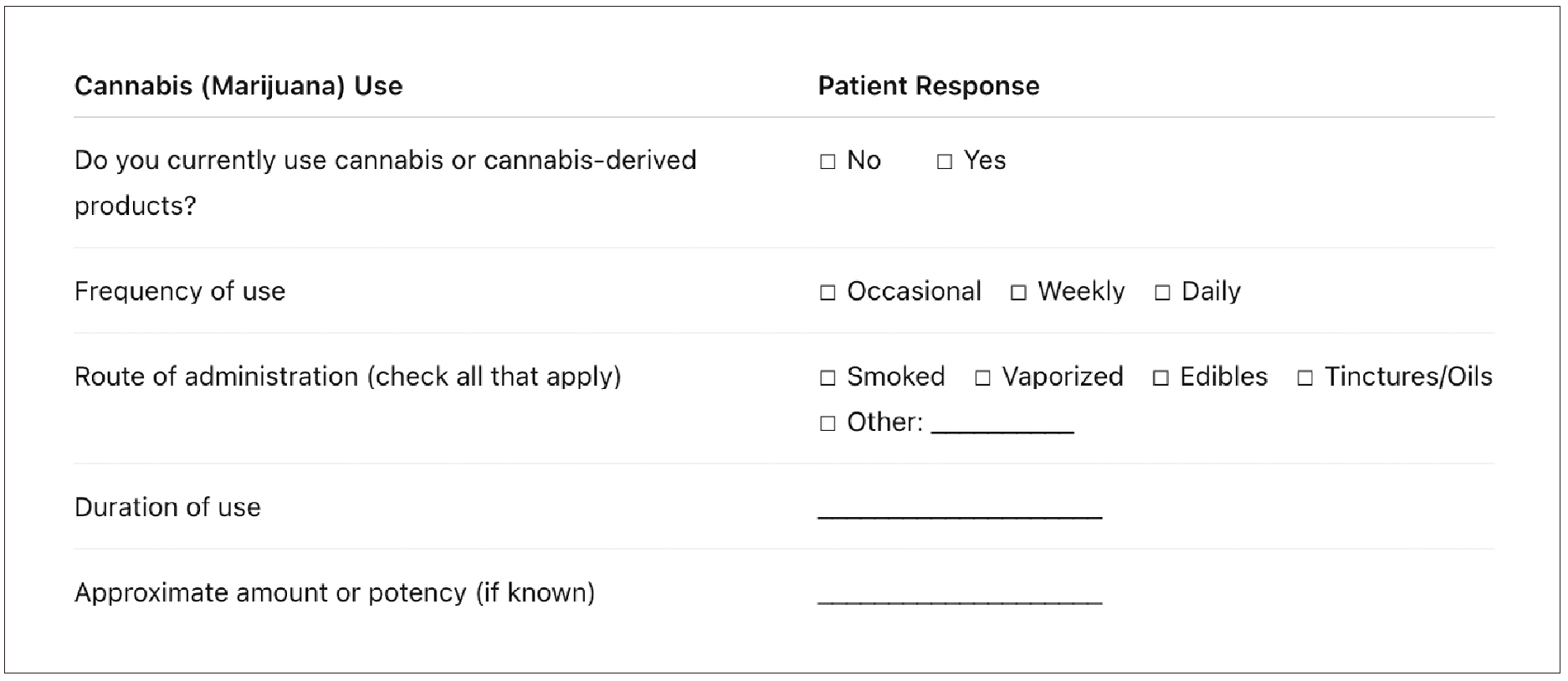
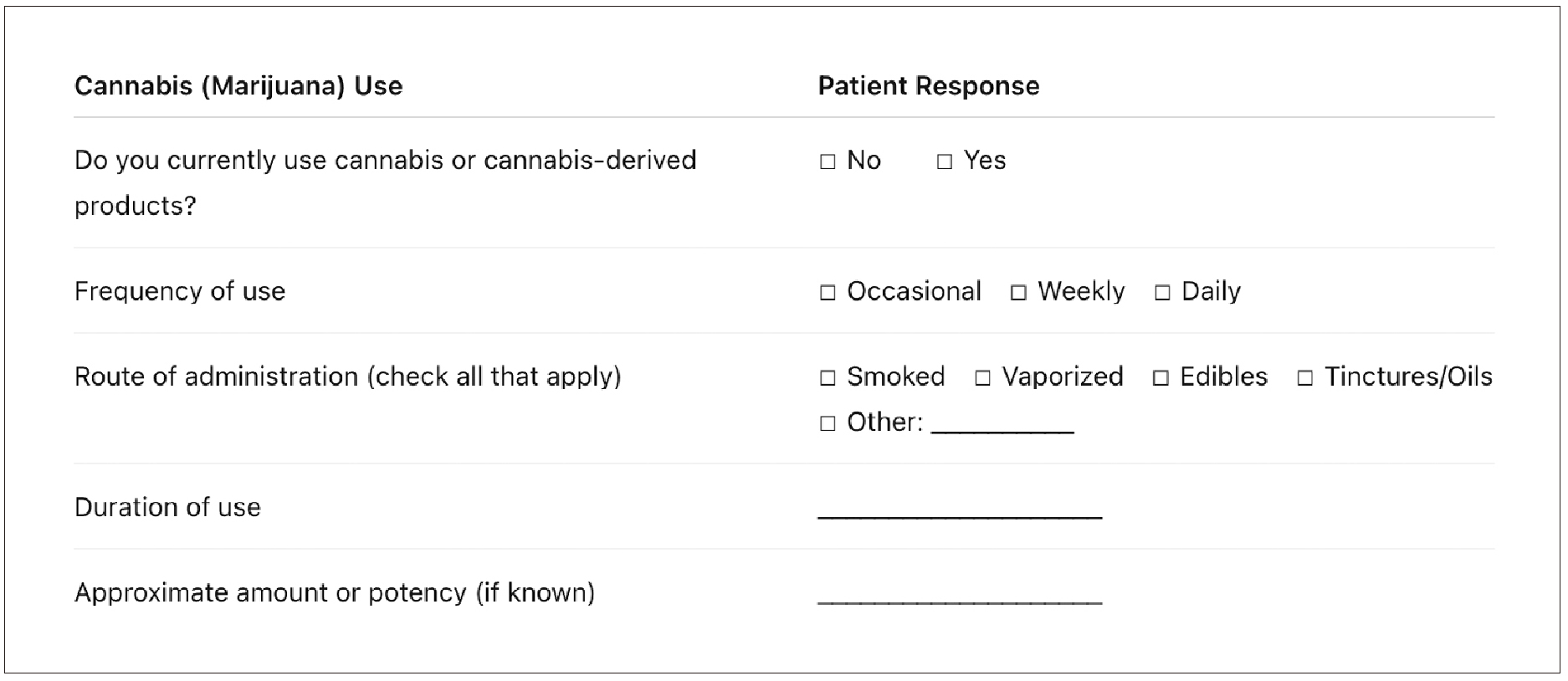
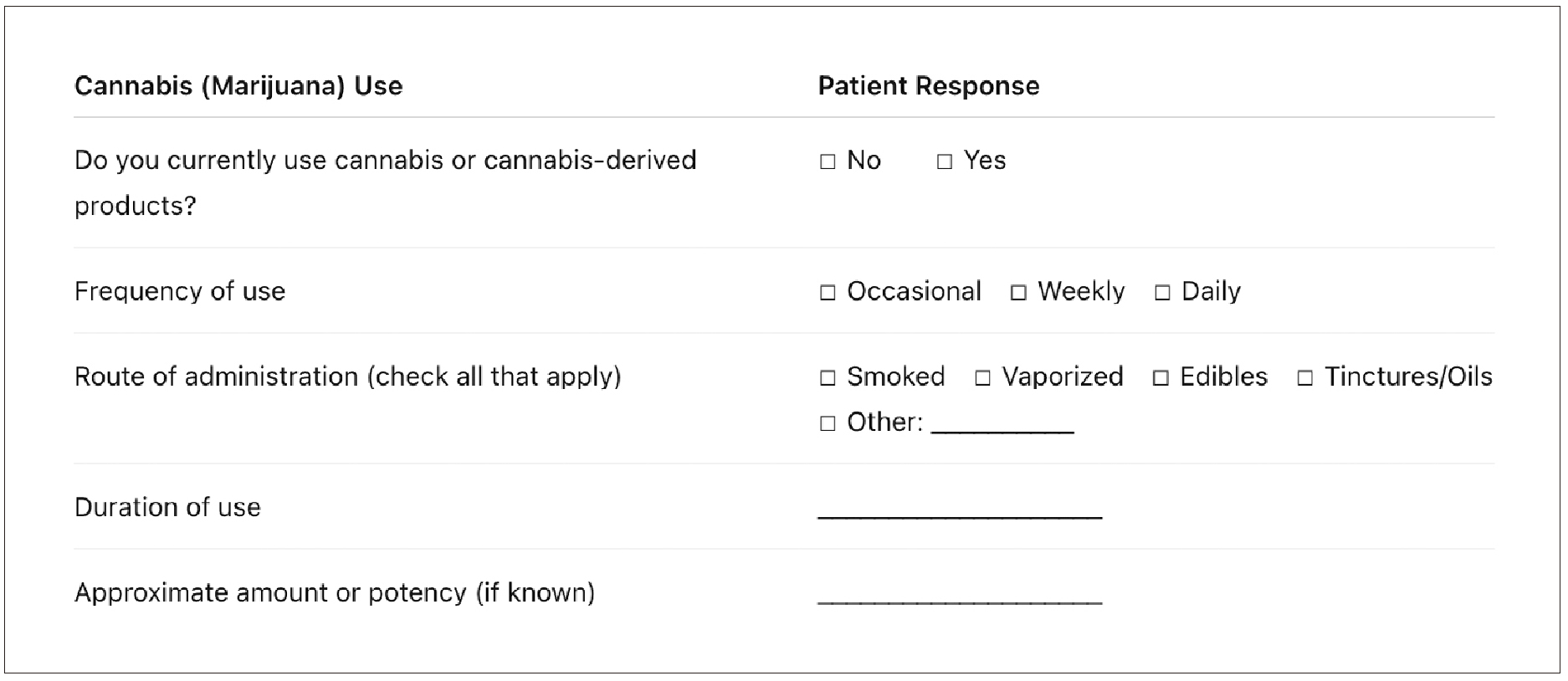
A thorough history of cannabis use should be incorporated into every implant evaluation, as this information is essential for anticipating potential intraoperative and postoperative complications. Clinicians should verify that cannabis use is explicitly included in the medical intake form, as many dental practices do not routinely capture this information, leading to unrecognized perioperative risk. Documentation should include the frequency, duration, and quantity of cannabis consumption, as well as the specific route of administration. Estimation of THC potency is important, as concentrated or aerosolized formulations may exert more pronounced physiologic and immunologic effects. The timing of the patient’s most recent cannabis exposure should also be established, given its influence on anesthetic requirements and perioperative responses. Additionally, providers should determine whether cannabis is used recreationally or for a medical indication, as coexisting systemic conditions or concomitant psychotropic medications may further influence surgical risk and treatment planning. (Figure 5)
(Fig.5) Cannabis-specific medical intake questionnaire.
Example of an intake form used to document cannabis use, including frequency, route of administration, duration, and potency, to support risk assessment and clinical decision-making in implant care.
2. Preoperative Risk Stratification
Following history acquisition, clinicians should assess individual risk factors that may predispose cannabis-using patients to peri-implant complications. Daily cannabis smokers or vapers, as well as users of high-potency concentrates, may exhibit greater impairment in immune function, vascular perfusion, and bone metabolism. Patients with existing periodontal disease constitute a particularly high-risk group, as periodontal inflammation is strongly associated with adverse peri-implant outcomes. Individuals with xerostomia or suboptimal oral hygiene practices should also be considered at elevated risk, as reduced salivary flow and inadequate plaque control promote the development of pathogenic biofilms capable of accelerating peri-implant mucosal and osseous breakdown.
3. Cannabis Cessation Recommendations
At present, no evidence-based perioperative guidelines exist that specifically address cannabis cessation in patients undergoing dental implant surgery. However, recommendations can be reasonably extrapolated from established data on wound healing, vascular reactivity, immune modulation, and the known effects of inhaled combustibles on postoperative outcomes. Based on these principles, it is advisable that patients abstain from cannabis use throughout the perioperative interval—defined as approximately one week prior to implant placement and a minimum of four weeks following surgery—to optimize tissue oxygenation, reduce inflammatory burden, stabilize cardiovascular responses, and support early osseointegration.
For individuals who use cannabis under medical supervision for a defined therapeutic indication, any perioperative modification to their regimen should be approached cautiously. In such cases, the prescribing physician should be consulted to evaluate the safety of temporary cessation or dose adjustment. Collaborative decision-making is essential to ensure that perioperative risk reduction does not compromise the management of the underlying condition for which cannabis was prescribed. This interdisciplinary approach allows for individualized treatment planning while prioritizing surgical safety and predictable implant integration.
4. Informed Consent
Informed consent (verbal and written) is a critical component of the pre-operative treatment planning process to ensure patients understand the risks of the use of THC and the intended implant procedure.
a. Verbal
Specific Risks: Given the rapid increase in high-potency THC formulations and concentrated delivery systems, clinicians should emphasize that the long-term impact of such products on implant survival remains insufficiently concluded, however current evidence suggests the potential for adverse effects. The consent process should therefore include discussion of the risk for both early failures related to impaired osseointegration and late failures associated with peri-implant inflammation or bone loss. Patients must be made aware that these complications may necessitate additional interventions, including surgical revision, grafting, or replacement of the implant.
Independent Witness Presence: Ideally, a witness (staff member) should be present and document (consent form) the confirmation the patient was fully informed.
b. Written
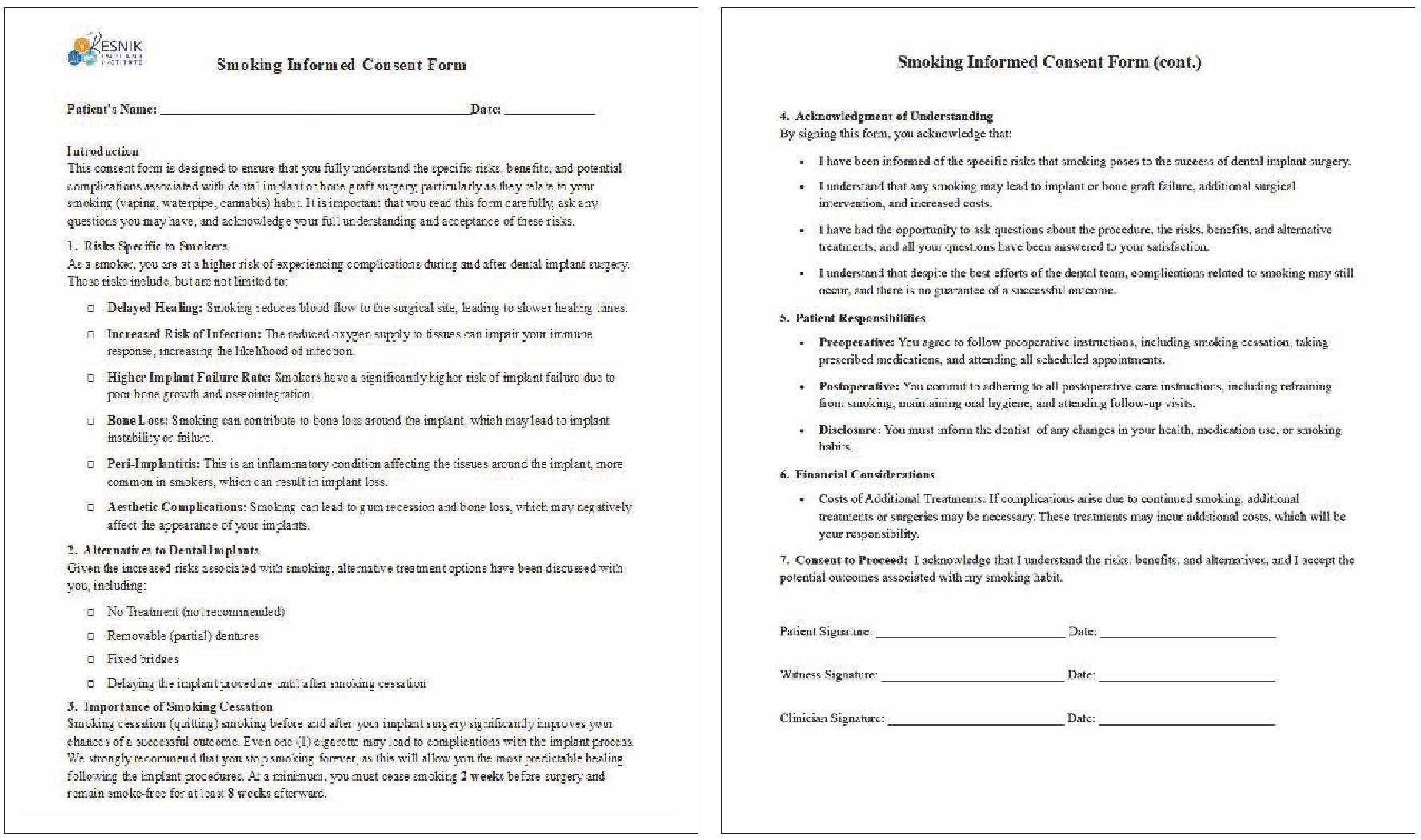
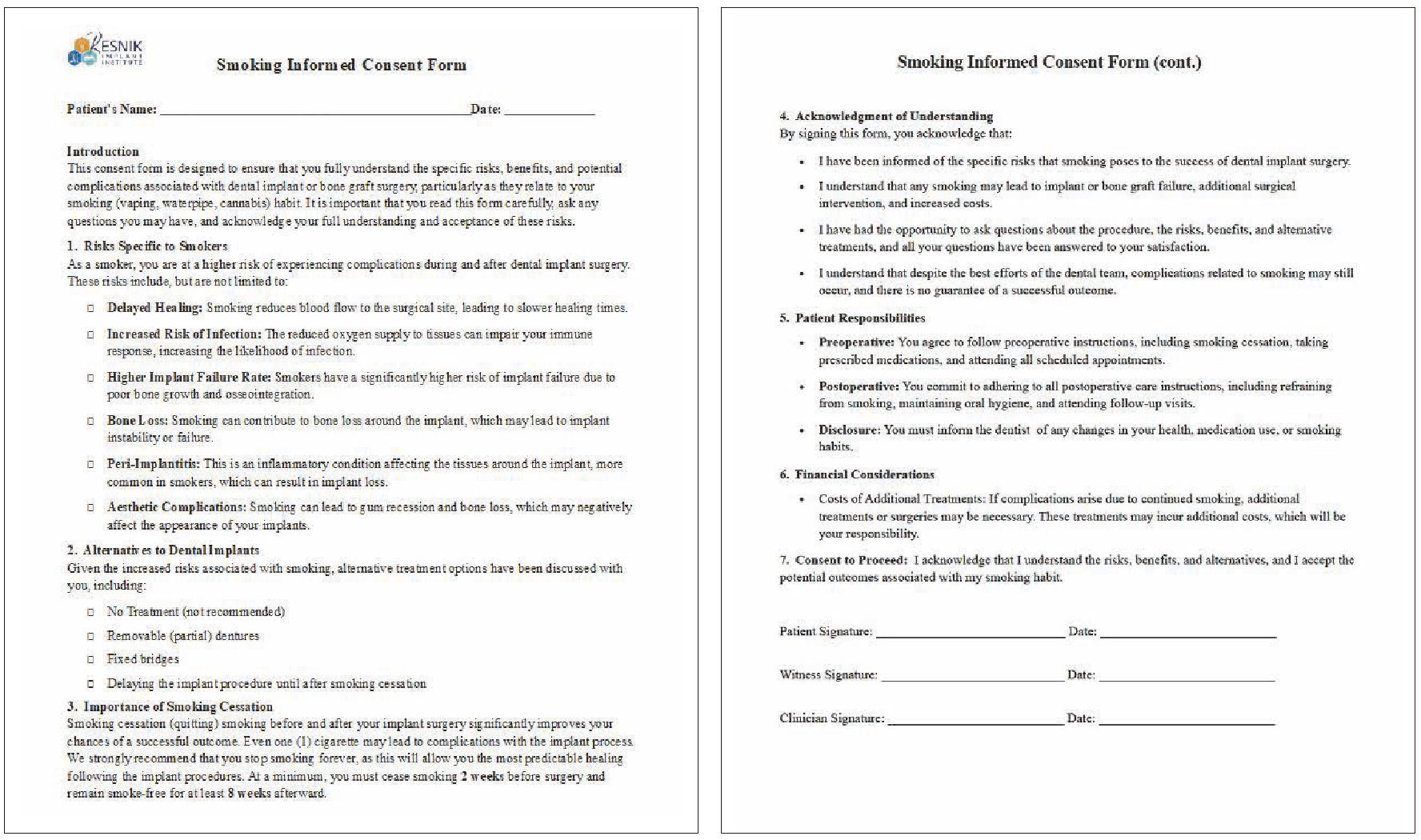
A comprehensive written consent form should be obtained, explicitly detailing the specific risks that THC poses to the dental implant process. This document must clearly outline the potential complications associated with these products, including impaired osseointegration, increased risk of implant failure, and delayed healing. To ensure informed decision-making, patients must review and sign the consent form (documenting patient acknowledgment) prior to the scheduled procedure. This process allows sufficient time for the patient to fully comprehend the associated risks and obtain clarification on any concerns. (Figure 6)
(Fig.6) Resnik Implant Institute Cannabis/ Tobacco Consent Form:
Representative example of written informed consent documents used to disclose the potential risks associated with cannabis and tobacco use in dental implant therapy, including impaired osseointegration, delayed healing, and increased risk of implant complications.
5. Enhanced Postoperative Protocols
Because cannabis users may be at heightened risk for peri-implant inflammation and healing complications, modified postoperative care protocols are advisable. More frequent recall visits and professional hygiene appointments may be necessary to manage plaque biofilm during the early healing phase. Adjunctive antimicrobial rinses, such as chlorhexidine, may be beneficial in reducing bacterial load and supporting mucosal health. Detailed education on daily plaque control methods should be provided, emphasizing the importance of mechanical disruption of biofilm around implants. For patients with cannabis-related xerostomia, management strategies—such as increased hydration, saliva stimulants, or saliva substitutes—can be implemented to improve oral clearance and support peri-implant tissue stability.
Conclusion
Cannabis exposure represents an increasingly relevant clinical variable in implant dentistry, driven by rising prevalence, escalating product potency, and the widespread use of inhalation-based delivery systems. Current evidence demonstrates that cannabis—particularly when smoked or vaporized—can adversely affect multiple physiologic pathways essential to implant success, including soft-tissue healing, salivary function, immune surveillance, vascular regulation, and bone remodeling. These biologic effects create a more permissive environment for peri-implant inflammation, accelerate biofilm maturation, and may impair early osseointegration, thereby increasing the likelihood of both early and late implant complications.
Although definitive long-term clinical data remain limited, the mechanistic and preclinical findings, combined with consistent epidemiologic associations with periodontal disease, justify a precautionary approach to treatment planning. Routine evaluation of cannabis use should therefore be incorporated into the medical history of every implant patient, with particular attention to frequency, route of administration, and timing of last exposure. Risk stratification, perioperative cessation recommendations, enhanced postoperative maintenance, and thorough informed consent are critical components of evidence-based care in this population.
As legalization continues to broaden access and novel high-potency formulations proliferate, the dental community must remain attentive to evolving scientific data and refine clinical protocols accordingly. Recognizing cannabis use as a meaningful risk modifier—and addressing it proactively through interdisciplinary communication, patient education, and tailored perioperative management—will be essential to ensuring safe, predictable, and durable dental implant outcomes.
References:
Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: Results from the 2021 National Survey on Drug Use and Health (HHS Publication No. PEP22-07-01-005, NSDUH Series H-57). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. 2022. https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report. Accessed on February 9, 2024.
Hasin DS, Saha TD, Kerridge BT, et al. Prevalence of marijuana use disorders in the United States between 2001-2002 and 2012-2013. JAMA Psychiatry. 2015 Dec;72(12):1235-1242. doi: 10.1001/jamapsychiatry.2015.1858.
Mims MM, Parikh AC, Sandhu Z, DeMoss N, Mhawej R, Queimado L. Surgery-Related Considerations in Treating People Who Use Cannabis: A Review. JAMA Otolaryngol Head Neck Surg. 2024 Oct 1;150(10):918-924. doi: 10.1001/jamaoto.2024.2545. PMID: 39172477.
Nogueira-Filho Gda R, Cadide T, Rosa BT, Neiva TG, Tunes R, Peruzzo D, Nociti FH Jr, César-Neto JB. Cannabis sativa smoke inhalation decreases bone filling around titanium implants: a histomorphometric study in rats. Implant Dent. 2008 Dec;17(4):461-70. doi: 10.1097/ID.0b013e31818c5a2a. PMID: 19077584.
Nogueira-Filho GR, Todescan S, Shah A, Rosa BT, Tunes Uda R, Cesar Neto JB. Impact of cannabis sativa (marijuana) smoke on alveolar bone loss: a histometric study in rats. J Periodontol. 2011 Nov;82(11):1602-7. doi: 10.1902/jop.2011.100362. Epub 2011 Mar 29. PMID: 21513470.
Pulvers K, Jamalian N, Suh E, Faltaoos P, Stewart SL, Aston ER. Nicotine and cannabis routes of administration and dual use among U.S. young adults who identify as Hispanic, non-Hispanic Black, and non-Hispanic White. Prev Med Rep. 2024 Oct 22;48:102912. doi: 10.1016/j.pmedr.2024.102912. PMID: 39526216; PMCID: PMC11550767.
Singh, H., J. Katz, W. Saleh, and S. Cha. "Impact of cannabis on the port of entry-oral tissues: an overview." Int J Oral Dent Health 5, no. 3 (2019): 1-5.
Graves BM, Johnson TJ, Nishida RT, Dias RP, Savareear B, Harynuk JJ, Kazemimanesh M, Olfert JS, Boies AM. Comprehensive characterization of mainstream marijuana and tobacco smoke. Sci Rep. 2020 Apr 28;10(1):7160. doi: 10.1038/s41598-020-63120-6. PMID: 32345986; PMCID: PMC7188852.
Moir D, Rickert WS, Levasseur G, Larose Y, Maertens R, White P, Desjardins S. A comparison of mainstream and sidestream marijuana and tobacco cigarette smoke produced under two machine smoking conditions. Chem Res Toxicol. 2008 Feb;21(2):494-502. doi: 10.1021/tx700275p. Epub 2007 Dec 7. PMID: 18062674.
Nogueira-Filho Gda R, Cadide T, Rosa BT, Neiva TG, Tunes R, Peruzzo D, Nociti FH Jr, César-Neto JB. Cannabis sativa smoke inhalation decreases bone filling around titanium implants: a histomorphometric study in rats. Implant Dent. 2008 Dec;17(4):461-70. doi: 10.1097/ID.0b013e31818c5a2a. PMID: 19077584.
Scott DA, Dukka H, Saxena D. Potential Mechanisms Underlying Marijuana-Associated Periodontal Tissue Destruction. J Dent Res. 2022 Feb;101(2):133-142. doi: 10.1177/00220345211036072. Epub 2021 Sep 13. PMID: 34515556; PMCID: PMC8905217.
Gu Z, Singh S, Niyogi RG, Lamont GJ, Wang H, Lamont RJ, Scott DA. Marijuana-Derived Cannabinoids Trigger a CB2/PI3K Axis of Suppression of the Innate Response to Oral Pathogens. Front Immunol. 2019 Oct 15;10:2288. doi: 10.3389/fimmu.2019.02288. PMID: 31681262; PMCID: PMC6804395.
McConnell WR, Dewey WL, Harris LS, Borzelleca JF. A study of the effect of delta 9-tetrahydrocannabinol (delta 9-THC) on mammalian salivary flow. J Pharmacol Exp Ther. 1978 Sep;206(3):567-73. PMID: 702321.
Baddour HM, Audemorte TB, Layman FD (1984) The occurrence of diffuse gingival hyperplasia in a patient using marijuana. J Tenn Dent Assoc 64: 39-43.
Rawal SY, Tatakis DN, Tipton DA (2012) Periodontal and oral manifestations of marijuana use. J Tenn Dent Assoc 92: 26-31.
Momen-Heravi F, Kang P (2017) Management of cannabisinduced periodontitis via resective surgical therapy: A clinical report. J Am Dent Assoc 148: 179-184.
Chisini LA, Cademartori MG, Francia A, Mederos M, Grazioli G, Conde MCM, Correa MB. Is the use of Cannabis associated with periodontitis? A systematic review and meta-analysis. J Periodontal Res. 2019 Aug;54(4):311-317. doi: 10.1111/jre.12639. Epub 2019 Jan 24. PMID: 30677134.
Shariff JA, Ahluwalia KP, Papapanou PN. Relationship Between Frequent Recreational Cannabis (Marijuana and Hashish) Use and Periodontitis in Adults in the United States: National Health and Nutrition Examination Survey 2011 to 2012. J Periodontol. 2017 Mar;88(3):273-280. doi: 10.1902/jop.2016.160370. Epub 2016 Oct 8. PMID: 27718772.
Thomson WM, Poulton R, Broadbent JM, Moffitt TE, Caspi A, Beck JD, Welch D, Hancox RJ. Cannabis smoking and periodontal disease among young adults. JAMA. 2008 Feb 6;299(5):525-31. doi: 10.1001/jama.299.5.525. PMID: 18252882; PMCID: PMC2823391.
Nogueira-Filho Gda R, Cadide T, Rosa BT, Neiva TG, Tunes R, Peruzzo D, Nociti FH Jr, César-Neto JB. Cannabis sativa smoke inhalation decreases bone filling around titanium implants: a histomorphometric study in rats. Implant Dent. 2008 Dec;17(4):461-70. doi: 10.1097/ID.0b013e31818c5a2a. PMID: 19077584.
Nogueira‐Filho, Getulio R., Sylvia Todescan, Adnan Shah, Bruno T. Rosa, Urbino da R. Tunes, and Joao B. Cesar Neto. "Impact of cannabis sativa (marijuana) smoke on alveolar bone loss: a histometric study in rats." Journal of periodontology 82, no. 11 (2011): 1602-1607.
Qi X, Liu C, Li G, Al-Alfe D, Paurazas S, Askar M, Yang D, Zhou Z. Evaluation of Cannabinoids on the Odonto/Osteogenesis in Human Dental Pulp Cells In Vitro. J Endod. 2021 Mar;47(3):444-450. doi: 10.1016/j.joen.2020.12.005. Epub 2021 Jan 20. PMID: 33352148.
Baker MB, Binda DD, Nozari A, Kennedy JM, Dienes E, Baker WE. Quantitative Analysis of Propofol Dosage in Cannabis Users: A Systematic Review and Meta-Analysis. J Clin Med. 2025 Jan 28;14(3):858. doi: 10.3390/jcm14030858. PMID: 39941531; PMCID: PMC11818839.
Ripperger D, Atte A, Ritto F. Cannabis Users Require More Anesthetic Agents for General Anesthesia in Ambulatory Oral and Maxillofacial Surgery Procedures. J Oral Maxillofac Surg. 2023 Dec;81(12):1460-1465. doi: 10.1016/j.joms.2023.09.008. Epub 2023 Sep 14. PMID: 37783364.
Shah S, Schwenk ES, Sondekoppam RV, Clarke H, Zakowski M, Rzasa-Lynn RS, Yeung B, Nicholson K, Schwartz G, Hooten WM, Wallace M, Viscusi ER, Narouze S. ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids. Reg Anesth Pain Med. 2023 Mar;48(3):97-117. doi: 10.1136/rapm-2022-104013. Epub 2023 Jan 3. PMID: 36596580.
Echeverria-Villalobos M, Fabian CA, Mitchell JG, Mazzotta E, Fiorda Diaz JC, Noon K, Weaver TE. Cannabinoids and General Anesthetics: Revisiting Molecular Mechanisms of Their Pharmacological Interactions. Anesth Analg. 2025 Jun 1;140(6):1401-1413. doi: 10.1213/ANE.0000000000007313. Epub 2024 Nov 6. PMID: 39504269; PMCID:
Mims, Mark M., Aniruddha C. Parikh, Zainab Sandhu, Noah DeMoss, Rachad Mhawej, and Lurdes Queimado. "Surgery-related considerations in treating people who use cannabis: a review." JAMA Otolaryngology–Head & Neck Surgery (2024).
Ekrami E, Sari S, Kopac O, Wang D, Mascha EJ, Stamper S, Esa WAS, Nair H, Ruetzler K, Turan A. Association Between Cannabis Use and Opioid Consumption, Pain, and Respiratory Complications After Surgery: A Retrospective Cohort Analysis. Anesth Analg. 2024 Oct 1;139(4):724-733. doi: 10.1213/ANE.0000000000006785. Epub 2024 Jan 8. PMID: 38190341.
King DD, Temmermand R, Greenwood JE. Preoperative cannabinoid exposure and postoperative pain: A narrative review. J Clin Anesth. 2025 Dec 16;109:112097. doi: 10.1016/j.jclinane.2025.112097. Epub ahead of print. PMID: 41406677.
Shah, Shalini, Eric S. Schwenk, Rakesh V. Sondekoppam, Hance Clarke, Mark Zakowski, Rachel S. Rzasa-Lynn, Brent Yeung et al. "ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids." Regional Anesthesia & Pain Medicine 48, no. 3 (2023): 97-117.
Guy D, Wootten JC, Wong M, Turski D, Lukewich M, Alboog A, Kandasamy AR, Gregory J, Poolacherla R. Pharmacodynamic effects following co-administration of cannabinoids and opioids: a scoping review of human experimental studies. Pain Med. 2024 Jul 1;25(7):423-434. doi: 10.1093/pm/pnae024. PMID: 38561178.
Echeverria-Villalobos M, Todeschini AB, Stoicea N, Fiorda-Diaz J, Weaver T, Bergese SD. Perioperative care of cannabis users: A comprehensive review of pharmacological and anesthetic considerations. J Clin Anesth. 2019 Nov;57:41-49. doi: 10.1016/j.jclinane.2019.03.011. Epub 2019 Mar 7. PMID: 30852326.
Shah, Shalini, Eric S. Schwenk, Rakesh V. Sondekoppam, Hance Clarke, Mark Zakowski, Rachel S. Rzasa-Lynn, Brent Yeung et al. "ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids." Regional Anesthesia & Pain Medicine 48, no. 3 (2023): 97-117.
Whiting, Penny F., Robert F. Wolff, Sohan Deshpande, Marcello Di Nisio, Steven Duffy, Adrian V. Hernandez, J. Christiaan Keurentjes et al. "Cannabinoids for medical use: a systematic review and meta-analysis." JAMA 313, no. 24 (2015): 2456-2473.
Schlienz NJ, Spindle TR, Cone EJ, Herrmann ES, Bigelow GE, Mitchell JM, Flegel R, LoDico C, Vandrey R. Pharmacodynamic dose effects of oral cannabis ingestion in healthy adults who infrequently use cannabis. Drug Alcohol Depend. 2020 Jun 1;211:107969. doi: 10.1016/j.drugalcdep.2020.107969. Epub 2020 Mar 21. PMID: 32298998; PMCID: PMC8221366.
Le A, Khoo E, Palamar JJ. Associations between Oral Health and Cannabis Use among Adolescents and Young Adults: Implications for Orthodontists. Int J Environ Res Public Health. 2022 Nov 18;19(22):15261. doi: 10.3390/ijerph192215261. PMID: 36429978; PMCID: PMC9691037.
近年来,大麻消费显著增加,其推动因素包括合法化范围扩大,社会态度转变以及高效力制剂的广泛可得性。根据美国疾病控制与预防中心(CDC)的数据,大麻仍是美国使用最普遍的联邦层面非法物质,约22%的12岁及以上人群报告在过去一年使用过大麻。1 流行病学研究进一步提示,近30%的大麻使用者可能符合“大麻使用障碍”(cannabis use disorder, CUD)的诊断标准;且起始年龄更早,使用频率更高,四氢大麻酚(THC)暴露更大者风险更高。2
在门诊口腔颌面外科手术环境中,也观察到大麻使用者需要显著更高剂量的多种麻醉药物:与非使用者相比,大麻使用者使用丙泊酚更多(152.5mg vs 117.5mg),咪达唑仑更多(5.1mg vs 4.7mg),氯胺酮更多(46.1mg vs 40.2mg)以及芬太尼更多(88.6μg vs 75.2μg)。25
Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: Results from the 2021 National Survey on Drug Use and Health (HHS Publication No. PEP22-07-01-005, NSDUH Series H-57). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. 2022. https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report. Accessed on February 9, 2024.
Hasin DS, Saha TD, Kerridge BT, et al. Prevalence of marijuana use disorders in the United States between 2001-2002 and 2012-2013. JAMA Psychiatry. 2015 Dec;72(12):1235-1242. doi: 10.1001/jamapsychiatry.2015.1858.
Mims MM, Parikh AC, Sandhu Z, DeMoss N, Mhawej R, Queimado L. Surgery-Related Considerations in Treating People Who Use Cannabis: A Review. JAMA Otolaryngol Head Neck Surg. 2024 Oct 1;150(10):918-924. doi: 10.1001/jamaoto.2024.2545. PMID: 39172477.
Nogueira-Filho Gda R, Cadide T, Rosa BT, Neiva TG, Tunes R, Peruzzo D, Nociti FH Jr, César-Neto JB. Cannabis sativa smoke inhalation decreases bone filling around titanium implants: a histomorphometric study in rats. Implant Dent. 2008 Dec;17(4):461-70. doi: 10.1097/ID.0b013e31818c5a2a. PMID: 19077584.
Nogueira-Filho GR, Todescan S, Shah A, Rosa BT, Tunes Uda R, Cesar Neto JB. Impact of cannabis sativa (marijuana) smoke on alveolar bone loss: a histometric study in rats. J Periodontol. 2011 Nov;82(11):1602-7. doi: 10.1902/jop.2011.100362. Epub 2011 Mar 29. PMID: 21513470.
Pulvers K, Jamalian N, Suh E, Faltaoos P, Stewart SL, Aston ER. Nicotine and cannabis routes of administration and dual use among U.S. young adults who identify as Hispanic, non-Hispanic Black, and non-Hispanic White. Prev Med Rep. 2024 Oct 22;48:102912. doi: 10.1016/j.pmedr.2024.102912. PMID: 39526216; PMCID: PMC11550767.
Singh, H., J. Katz, W. Saleh, and S. Cha. "Impact of cannabis on the port of entry-oral tissues: an overview." Int J Oral Dent Health 5, no. 3 (2019): 1-5.
Graves BM, Johnson TJ, Nishida RT, Dias RP, Savareear B, Harynuk JJ, Kazemimanesh M, Olfert JS, Boies AM. Comprehensive characterization of mainstream marijuana and tobacco smoke. Sci Rep. 2020 Apr 28;10(1):7160. doi: 10.1038/s41598-020-63120-6. PMID: 32345986; PMCID: PMC7188852.
Moir D, Rickert WS, Levasseur G, Larose Y, Maertens R, White P, Desjardins S. A comparison of mainstream and sidestream marijuana and tobacco cigarette smoke produced under two machine smoking conditions. Chem Res Toxicol. 2008 Feb;21(2):494-502. doi: 10.1021/tx700275p. Epub 2007 Dec 7. PMID: 18062674.
Nogueira-Filho Gda R, Cadide T, Rosa BT, Neiva TG, Tunes R, Peruzzo D, Nociti FH Jr, César-Neto JB. Cannabis sativa smoke inhalation decreases bone filling around titanium implants: a histomorphometric study in rats. Implant Dent. 2008 Dec;17(4):461-70. doi: 10.1097/ID.0b013e31818c5a2a. PMID: 19077584.
Scott DA, Dukka H, Saxena D. Potential Mechanisms Underlying Marijuana-Associated Periodontal Tissue Destruction. J Dent Res. 2022 Feb;101(2):133-142. doi: 10.1177/00220345211036072. Epub 2021 Sep 13. PMID: 34515556; PMCID: PMC8905217.
Gu Z, Singh S, Niyogi RG, Lamont GJ, Wang H, Lamont RJ, Scott DA. Marijuana-Derived Cannabinoids Trigger a CB2/PI3K Axis of Suppression of the Innate Response to Oral Pathogens. Front Immunol. 2019 Oct 15;10:2288. doi: 10.3389/fimmu.2019.02288. PMID: 31681262; PMCID: PMC6804395.
McConnell WR, Dewey WL, Harris LS, Borzelleca JF. A study of the effect of delta 9-tetrahydrocannabinol (delta 9-THC) on mammalian salivary flow. J Pharmacol Exp Ther. 1978 Sep;206(3):567-73. PMID: 702321.
Baddour HM, Audemorte TB, Layman FD (1984) The occurrence of diffuse gingival hyperplasia in a patient using marijuana. J Tenn Dent Assoc 64: 39-43.
Rawal SY, Tatakis DN, Tipton DA (2012) Periodontal and oral manifestations of marijuana use. J Tenn Dent Assoc 92: 26-31.
Momen-Heravi F, Kang P (2017) Management of cannabisinduced periodontitis via resective surgical therapy: A clinical report. J Am Dent Assoc 148: 179-184.
Chisini LA, Cademartori MG, Francia A, Mederos M, Grazioli G, Conde MCM, Correa MB. Is the use of Cannabis associated with periodontitis? A systematic review and meta-analysis. J Periodontal Res. 2019 Aug;54(4):311-317. doi: 10.1111/jre.12639. Epub 2019 Jan 24. PMID: 30677134.
Shariff JA, Ahluwalia KP, Papapanou PN. Relationship Between Frequent Recreational Cannabis (Marijuana and Hashish) Use and Periodontitis in Adults in the United States: National Health and Nutrition Examination Survey 2011 to 2012. J Periodontol. 2017 Mar;88(3):273-280. doi: 10.1902/jop.2016.160370. Epub 2016 Oct 8. PMID: 27718772.
Thomson WM, Poulton R, Broadbent JM, Moffitt TE, Caspi A, Beck JD, Welch D, Hancox RJ. Cannabis smoking and periodontal disease among young adults. JAMA. 2008 Feb 6;299(5):525-31. doi: 10.1001/jama.299.5.525. PMID: 18252882; PMCID: PMC2823391.
Nogueira-Filho Gda R, Cadide T, Rosa BT, Neiva TG, Tunes R, Peruzzo D, Nociti FH Jr, César-Neto JB. Cannabis sativa smoke inhalation decreases bone filling around titanium implants: a histomorphometric study in rats. Implant Dent. 2008 Dec;17(4):461-70. doi: 10.1097/ID.0b013e31818c5a2a. PMID: 19077584.
Nogueira‐Filho, Getulio R., Sylvia Todescan, Adnan Shah, Bruno T. Rosa, Urbino da R. Tunes, and Joao B. Cesar Neto. "Impact of cannabis sativa (marijuana) smoke on alveolar bone loss: a histometric study in rats." Journal of periodontology 82, no. 11 (2011): 1602-1607.
Qi X, Liu C, Li G, Al-Alfe D, Paurazas S, Askar M, Yang D, Zhou Z. Evaluation of Cannabinoids on the Odonto/Osteogenesis in Human Dental Pulp Cells In Vitro. J Endod. 2021 Mar;47(3):444-450. doi: 10.1016/j.joen.2020.12.005. Epub 2021 Jan 20. PMID: 33352148.
Baker MB, Binda DD, Nozari A, Kennedy JM, Dienes E, Baker WE. Quantitative Analysis of Propofol Dosage in Cannabis Users: A Systematic Review and Meta-Analysis. J Clin Med. 2025 Jan 28;14(3):858. doi: 10.3390/jcm14030858. PMID: 39941531; PMCID: PMC11818839.
Ripperger D, Atte A, Ritto F. Cannabis Users Require More Anesthetic Agents for General Anesthesia in Ambulatory Oral and Maxillofacial Surgery Procedures. J Oral Maxillofac Surg. 2023 Dec;81(12):1460-1465. doi: 10.1016/j.joms.2023.09.008. Epub 2023 Sep 14. PMID: 37783364.
Shah S, Schwenk ES, Sondekoppam RV, Clarke H, Zakowski M, Rzasa-Lynn RS, Yeung B, Nicholson K, Schwartz G, Hooten WM, Wallace M, Viscusi ER, Narouze S. ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids. Reg Anesth Pain Med. 2023 Mar;48(3):97-117. doi: 10.1136/rapm-2022-104013. Epub 2023 Jan 3. PMID: 36596580.
Echeverria-Villalobos M, Fabian CA, Mitchell JG, Mazzotta E, Fiorda Diaz JC, Noon K, Weaver TE. Cannabinoids and General Anesthetics: Revisiting Molecular Mechanisms of Their Pharmacological Interactions. Anesth Analg. 2025 Jun 1;140(6):1401-1413. doi: 10.1213/ANE.0000000000007313. Epub 2024 Nov 6. PMID: 39504269; PMCID:
Mims, Mark M., Aniruddha C. Parikh, Zainab Sandhu, Noah DeMoss, Rachad Mhawej, and Lurdes Queimado. "Surgery-related considerations in treating people who use cannabis: a review." JAMA Otolaryngology–Head & Neck Surgery (2024).
Ekrami E, Sari S, Kopac O, Wang D, Mascha EJ, Stamper S, Esa WAS, Nair H, Ruetzler K, Turan A. Association Between Cannabis Use and Opioid Consumption, Pain, and Respiratory Complications After Surgery: A Retrospective Cohort Analysis. Anesth Analg. 2024 Oct 1;139(4):724-733. doi: 10.1213/ANE.0000000000006785. Epub 2024 Jan 8. PMID: 38190341.
King DD, Temmermand R, Greenwood JE. Preoperative cannabinoid exposure and postoperative pain: A narrative review. J Clin Anesth. 2025 Dec 16;109:112097. doi: 10.1016/j.jclinane.2025.112097. Epub ahead of print. PMID: 41406677.
Shah, Shalini, Eric S. Schwenk, Rakesh V. Sondekoppam, Hance Clarke, Mark Zakowski, Rachel S. Rzasa-Lynn, Brent Yeung et al. "ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids." Regional Anesthesia & Pain Medicine 48, no. 3 (2023): 97-117.
Guy D, Wootten JC, Wong M, Turski D, Lukewich M, Alboog A, Kandasamy AR, Gregory J, Poolacherla R. Pharmacodynamic effects following co-administration of cannabinoids and opioids: a scoping review of human experimental studies. Pain Med. 2024 Jul 1;25(7):423-434. doi: 10.1093/pm/pnae024. PMID: 38561178.
Echeverria-Villalobos M, Todeschini AB, Stoicea N, Fiorda-Diaz J, Weaver T, Bergese SD. Perioperative care of cannabis users: A comprehensive review of pharmacological and anesthetic considerations. J Clin Anesth. 2019 Nov;57:41-49. doi: 10.1016/j.jclinane.2019.03.011. Epub 2019 Mar 7. PMID: 30852326.
Shah, Shalini, Eric S. Schwenk, Rakesh V. Sondekoppam, Hance Clarke, Mark Zakowski, Rachel S. Rzasa-Lynn, Brent Yeung et al. "ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids." Regional Anesthesia & Pain Medicine 48, no. 3 (2023): 97-117.
Whiting, Penny F., Robert F. Wolff, Sohan Deshpande, Marcello Di Nisio, Steven Duffy, Adrian V. Hernandez, J. Christiaan Keurentjes et al. "Cannabinoids for medical use: a systematic review and meta-analysis." JAMA 313, no. 24 (2015): 2456-2473.
Schlienz NJ, Spindle TR, Cone EJ, Herrmann ES, Bigelow GE, Mitchell JM, Flegel R, LoDico C, Vandrey R. Pharmacodynamic dose effects of oral cannabis ingestion in healthy adults who infrequently use cannabis. Drug Alcohol Depend. 2020 Jun 1;211:107969. doi: 10.1016/j.drugalcdep.2020.107969. Epub 2020 Mar 21. PMID: 32298998; PMCID: PMC8221366.
Le A, Khoo E, Palamar JJ. Associations between Oral Health and Cannabis Use among Adolescents and Young Adults: Implications for Orthodontists. Int J Environ Res Public Health. 2022 Nov 18;19(22):15261. doi: 10.3390/ijerph192215261. PMID: 36429978; PMCID: PMC9691037.
外来での口腔・顎顔面外科手術においても同様に,大麻使用者は複数の麻酔薬について有意に高い用量を必要としたことが示されている.具体的には,大麻使用者は非使用者と比較して以下の用量を投与された:プロポフォール(152.5mg vs 117.5mg),ミダゾラム(5.1mg vs 4.7mg),ケタミン(46.1mg vs 40.2mg),フェンタニル(88.6µg vs 75.2µg).25
Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: Results from the 2021 National Survey on Drug Use and Health (HHS Publication No. PEP22-07-01-005, NSDUH Series H-57). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. 2022. https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report. Accessed on February 9, 2024.
Hasin DS, Saha TD, Kerridge BT, et al. Prevalence of marijuana use disorders in the United States between 2001-2002 and 2012-2013. JAMA Psychiatry. 2015 Dec;72(12):1235-1242. doi: 10.1001/jamapsychiatry.2015.1858.
Mims MM, Parikh AC, Sandhu Z, DeMoss N, Mhawej R, Queimado L. Surgery-Related Considerations in Treating People Who Use Cannabis: A Review. JAMA Otolaryngol Head Neck Surg. 2024 Oct 1;150(10):918-924. doi: 10.1001/jamaoto.2024.2545. PMID: 39172477.
Nogueira-Filho Gda R, Cadide T, Rosa BT, Neiva TG, Tunes R, Peruzzo D, Nociti FH Jr, César-Neto JB. Cannabis sativa smoke inhalation decreases bone filling around titanium implants: a histomorphometric study in rats. Implant Dent. 2008 Dec;17(4):461-70. doi: 10.1097/ID.0b013e31818c5a2a. PMID: 19077584.
Nogueira-Filho GR, Todescan S, Shah A, Rosa BT, Tunes Uda R, Cesar Neto JB. Impact of cannabis sativa (marijuana) smoke on alveolar bone loss: a histometric study in rats. J Periodontol. 2011 Nov;82(11):1602-7. doi: 10.1902/jop.2011.100362. Epub 2011 Mar 29. PMID: 21513470.
Pulvers K, Jamalian N, Suh E, Faltaoos P, Stewart SL, Aston ER. Nicotine and cannabis routes of administration and dual use among U.S. young adults who identify as Hispanic, non-Hispanic Black, and non-Hispanic White. Prev Med Rep. 2024 Oct 22;48:102912. doi: 10.1016/j.pmedr.2024.102912. PMID: 39526216; PMCID: PMC11550767.
Singh, H., J. Katz, W. Saleh, and S. Cha. "Impact of cannabis on the port of entry-oral tissues: an overview." Int J Oral Dent Health 5, no. 3 (2019): 1-5.
Graves BM, Johnson TJ, Nishida RT, Dias RP, Savareear B, Harynuk JJ, Kazemimanesh M, Olfert JS, Boies AM. Comprehensive characterization of mainstream marijuana and tobacco smoke. Sci Rep. 2020 Apr 28;10(1):7160. doi: 10.1038/s41598-020-63120-6. PMID: 32345986; PMCID: PMC7188852.
Moir D, Rickert WS, Levasseur G, Larose Y, Maertens R, White P, Desjardins S. A comparison of mainstream and sidestream marijuana and tobacco cigarette smoke produced under two machine smoking conditions. Chem Res Toxicol. 2008 Feb;21(2):494-502. doi: 10.1021/tx700275p. Epub 2007 Dec 7. PMID: 18062674.
Nogueira-Filho Gda R, Cadide T, Rosa BT, Neiva TG, Tunes R, Peruzzo D, Nociti FH Jr, César-Neto JB. Cannabis sativa smoke inhalation decreases bone filling around titanium implants: a histomorphometric study in rats. Implant Dent. 2008 Dec;17(4):461-70. doi: 10.1097/ID.0b013e31818c5a2a. PMID: 19077584.
Scott DA, Dukka H, Saxena D. Potential Mechanisms Underlying Marijuana-Associated Periodontal Tissue Destruction. J Dent Res. 2022 Feb;101(2):133-142. doi: 10.1177/00220345211036072. Epub 2021 Sep 13. PMID: 34515556; PMCID: PMC8905217.
Gu Z, Singh S, Niyogi RG, Lamont GJ, Wang H, Lamont RJ, Scott DA. Marijuana-Derived Cannabinoids Trigger a CB2/PI3K Axis of Suppression of the Innate Response to Oral Pathogens. Front Immunol. 2019 Oct 15;10:2288. doi: 10.3389/fimmu.2019.02288. PMID: 31681262; PMCID: PMC6804395.
McConnell WR, Dewey WL, Harris LS, Borzelleca JF. A study of the effect of delta 9-tetrahydrocannabinol (delta 9-THC) on mammalian salivary flow. J Pharmacol Exp Ther. 1978 Sep;206(3):567-73. PMID: 702321.
Baddour HM, Audemorte TB, Layman FD (1984) The occurrence of diffuse gingival hyperplasia in a patient using marijuana. J Tenn Dent Assoc 64: 39-43.
Rawal SY, Tatakis DN, Tipton DA (2012) Periodontal and oral manifestations of marijuana use. J Tenn Dent Assoc 92: 26-31.
Momen-Heravi F, Kang P (2017) Management of cannabisinduced periodontitis via resective surgical therapy: A clinical report. J Am Dent Assoc 148: 179-184.
Chisini LA, Cademartori MG, Francia A, Mederos M, Grazioli G, Conde MCM, Correa MB. Is the use of Cannabis associated with periodontitis? A systematic review and meta-analysis. J Periodontal Res. 2019 Aug;54(4):311-317. doi: 10.1111/jre.12639. Epub 2019 Jan 24. PMID: 30677134.
Shariff JA, Ahluwalia KP, Papapanou PN. Relationship Between Frequent Recreational Cannabis (Marijuana and Hashish) Use and Periodontitis in Adults in the United States: National Health and Nutrition Examination Survey 2011 to 2012. J Periodontol. 2017 Mar;88(3):273-280. doi: 10.1902/jop.2016.160370. Epub 2016 Oct 8. PMID: 27718772.
Thomson WM, Poulton R, Broadbent JM, Moffitt TE, Caspi A, Beck JD, Welch D, Hancox RJ. Cannabis smoking and periodontal disease among young adults. JAMA. 2008 Feb 6;299(5):525-31. doi: 10.1001/jama.299.5.525. PMID: 18252882; PMCID: PMC2823391.
Nogueira-Filho Gda R, Cadide T, Rosa BT, Neiva TG, Tunes R, Peruzzo D, Nociti FH Jr, César-Neto JB. Cannabis sativa smoke inhalation decreases bone filling around titanium implants: a histomorphometric study in rats. Implant Dent. 2008 Dec;17(4):461-70. doi: 10.1097/ID.0b013e31818c5a2a. PMID: 19077584.
Nogueira‐Filho, Getulio R., Sylvia Todescan, Adnan Shah, Bruno T. Rosa, Urbino da R. Tunes, and Joao B. Cesar Neto. "Impact of cannabis sativa (marijuana) smoke on alveolar bone loss: a histometric study in rats." Journal of periodontology 82, no. 11 (2011): 1602-1607.
Qi X, Liu C, Li G, Al-Alfe D, Paurazas S, Askar M, Yang D, Zhou Z. Evaluation of Cannabinoids on the Odonto/Osteogenesis in Human Dental Pulp Cells In Vitro. J Endod. 2021 Mar;47(3):444-450. doi: 10.1016/j.joen.2020.12.005. Epub 2021 Jan 20. PMID: 33352148.
Baker MB, Binda DD, Nozari A, Kennedy JM, Dienes E, Baker WE. Quantitative Analysis of Propofol Dosage in Cannabis Users: A Systematic Review and Meta-Analysis. J Clin Med. 2025 Jan 28;14(3):858. doi: 10.3390/jcm14030858. PMID: 39941531; PMCID: PMC11818839.
Ripperger D, Atte A, Ritto F. Cannabis Users Require More Anesthetic Agents for General Anesthesia in Ambulatory Oral and Maxillofacial Surgery Procedures. J Oral Maxillofac Surg. 2023 Dec;81(12):1460-1465. doi: 10.1016/j.joms.2023.09.008. Epub 2023 Sep 14. PMID: 37783364.
Shah S, Schwenk ES, Sondekoppam RV, Clarke H, Zakowski M, Rzasa-Lynn RS, Yeung B, Nicholson K, Schwartz G, Hooten WM, Wallace M, Viscusi ER, Narouze S. ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids. Reg Anesth Pain Med. 2023 Mar;48(3):97-117. doi: 10.1136/rapm-2022-104013. Epub 2023 Jan 3. PMID: 36596580.
Echeverria-Villalobos M, Fabian CA, Mitchell JG, Mazzotta E, Fiorda Diaz JC, Noon K, Weaver TE. Cannabinoids and General Anesthetics: Revisiting Molecular Mechanisms of Their Pharmacological Interactions. Anesth Analg. 2025 Jun 1;140(6):1401-1413. doi: 10.1213/ANE.0000000000007313. Epub 2024 Nov 6. PMID: 39504269; PMCID:
Mims, Mark M., Aniruddha C. Parikh, Zainab Sandhu, Noah DeMoss, Rachad Mhawej, and Lurdes Queimado. "Surgery-related considerations in treating people who use cannabis: a review." JAMA Otolaryngology–Head & Neck Surgery (2024).
Ekrami E, Sari S, Kopac O, Wang D, Mascha EJ, Stamper S, Esa WAS, Nair H, Ruetzler K, Turan A. Association Between Cannabis Use and Opioid Consumption, Pain, and Respiratory Complications After Surgery: A Retrospective Cohort Analysis. Anesth Analg. 2024 Oct 1;139(4):724-733. doi: 10.1213/ANE.0000000000006785. Epub 2024 Jan 8. PMID: 38190341.
King DD, Temmermand R, Greenwood JE. Preoperative cannabinoid exposure and postoperative pain: A narrative review. J Clin Anesth. 2025 Dec 16;109:112097. doi: 10.1016/j.jclinane.2025.112097. Epub ahead of print. PMID: 41406677.
Shah, Shalini, Eric S. Schwenk, Rakesh V. Sondekoppam, Hance Clarke, Mark Zakowski, Rachel S. Rzasa-Lynn, Brent Yeung et al. "ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids." Regional Anesthesia & Pain Medicine 48, no. 3 (2023): 97-117.
Guy D, Wootten JC, Wong M, Turski D, Lukewich M, Alboog A, Kandasamy AR, Gregory J, Poolacherla R. Pharmacodynamic effects following co-administration of cannabinoids and opioids: a scoping review of human experimental studies. Pain Med. 2024 Jul 1;25(7):423-434. doi: 10.1093/pm/pnae024. PMID: 38561178.
Echeverria-Villalobos M, Todeschini AB, Stoicea N, Fiorda-Diaz J, Weaver T, Bergese SD. Perioperative care of cannabis users: A comprehensive review of pharmacological and anesthetic considerations. J Clin Anesth. 2019 Nov;57:41-49. doi: 10.1016/j.jclinane.2019.03.011. Epub 2019 Mar 7. PMID: 30852326.
Shah, Shalini, Eric S. Schwenk, Rakesh V. Sondekoppam, Hance Clarke, Mark Zakowski, Rachel S. Rzasa-Lynn, Brent Yeung et al. "ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids." Regional Anesthesia & Pain Medicine 48, no. 3 (2023): 97-117.
Whiting, Penny F., Robert F. Wolff, Sohan Deshpande, Marcello Di Nisio, Steven Duffy, Adrian V. Hernandez, J. Christiaan Keurentjes et al. "Cannabinoids for medical use: a systematic review and meta-analysis." JAMA 313, no. 24 (2015): 2456-2473.
Schlienz NJ, Spindle TR, Cone EJ, Herrmann ES, Bigelow GE, Mitchell JM, Flegel R, LoDico C, Vandrey R. Pharmacodynamic dose effects of oral cannabis ingestion in healthy adults who infrequently use cannabis. Drug Alcohol Depend. 2020 Jun 1;211:107969. doi: 10.1016/j.drugalcdep.2020.107969. Epub 2020 Mar 21. PMID: 32298998; PMCID: PMC8221366.
Le A, Khoo E, Palamar JJ. Associations between Oral Health and Cannabis Use among Adolescents and Young Adults: Implications for Orthodontists. Int J Environ Res Public Health. 2022 Nov 18;19(22):15261. doi: 10.3390/ijerph192215261. PMID: 36429978; PMCID: PMC9691037.
El consumo de cannabis ha aumentado sustancialmente en años recientes, impulsado por la expansión de su legalización, cambios en las actitudes sociales y la amplia disponibilidad de formulaciones de alta potencia. Según datos de los Centros para el Control y la Prevención de Enfermedades (CDC), el cannabis sigue siendo la sustancia ilegal a nivel federal más utilizada en Estados Unidos, y aproximadamente el 22% de las personas de 12 años o más reportaron haberlo usado en el último año.1 Estudios epidemiológicos sugieren además que casi el 30% de los consumidores de cannabis podrían cumplir con los criterios diagnósticos para trastorno por uso de cannabis (TUC), con un riesgo mayor asociado al inicio temprano, mayor frecuencia de uso y mayor exposición al tetrahidrocannabinol (THC).2
Aunque el uso de cannabis suele percibirse como relativamente benigno, sus efectos farmacológicos se extienden a múltiples sistemas orgánicos mediante la activación del sistema endocannabinoide. En relación con la salud bucal, los receptores cannabinoides se expresan en células inmunitarias, tejido óseo y mucosa oral, lo que sugiere efectos potenciales sobre la respuesta inflamatoria, la cicatrización de heridas y el metabolismo óseo. Estos procesos biológicos son determinantes críticos del éxito en la terapia con implantes dentales, incluida la osteointegración y la estabilidad a largo plazo de los tejidos periimplantarios.
A pesar de la creciente prevalencia del consumo de cannabis entre adultos —especialmente en los grupos etarios con mayor probabilidad de buscar rehabilitación con implantes—, sus implicaciones en la implantología dental siguen siendo poco reconocidas e insuficientemente caracterizadas. Evidencia emergente indica que el uso de cannabis podría asociarse con alteraciones en la función inmunitaria, deterioro en la cicatrización y cambios en la biología ósea, factores que podrían influir en la salud periimplantaria y el éxito del implante.3 Sin embargo, los datos existentes son limitados, heterogéneos y a menudo extrapolados de modelos no dentales.
Esta revisión narrativa no propone pautas clínicas formales ni afirma relaciones causales entre el uso de cannabis y el fracaso de implantes dentales. Más bien, tiene como objetivo sintetizar la plausibilidad biológica, la evidencia clínica y experimental emergente, y los principios establecidos sobre cicatrización y biología ósea, para apoyar la evaluación de riesgos, la orientación al paciente y la toma de decisiones clínicas en implantología dental.
Mecanismo de acción
El principal constituyente psicoactivo del cannabis, el Δ9 -tetrahidrocannabinol (THC), ejerce sus efectos principalmente mediante la activación de los receptores cannabinoides tipo 1 (CB1) y tipo 2 (CB2). Los receptores CB1 se expresan abundantemente en el sistema nervioso central y son en gran parte responsables de los efectos psicoactivos del THC, mientras que los receptores CB2 están predominantemente asociados con la modulación inmunitaria y se expresan en células inmunitarias, tejido óseo y órganos periféricos, incluyendo la vasculatura.
El THC produce efectos psicoactivos rápidos y predecibles, lo que contribuye a su uso generalizado por beneficios percibidos como relajación, reducción del estrés, euforia y analgesia. No obstante, la activación del sistema endocannabinoide también influye en las vías inflamatorias, la función de las células inmunitarias, el tono vascular y el metabolismo óseo —procesos biológicos directamente relevantes para la cicatrización y la osteointegración en la terapia con implantes dentales.
Aunque el uso de cannabis suele percibirse como “natural” o más seguro que el alcohol o los medicamentos recetados, los productos contemporáneos contienen concentraciones de THC sustancialmente más altas que las históricamente encontradas. Como resultado, los efectos fisiológicos y clínicos pueden variar considerablemente y están influenciados por la dosis, la frecuencia de uso, la vía de administración y la susceptibilidad individual. Estos factores complican la evaluación de riesgos y subrayan la necesidad de considerar cuidadosamente el uso de cannabis en pacientes sometidos a procedimientos quirúrgicos relacionados con implantes.4,5
Vía de administración
El cannabis puede administrarse por múltiples vías, cada una asociada con características farmacocinéticas distintas, patrones de exposición sistémica e interacciones locales con los tejidos que pueden influir en la cicatrización periimplantaria y la osteointegración. Las variaciones en la vía de administración afectan la velocidad y el grado de absorción de los cannabinoides, las concentraciones plasmáticas máximas, la duración de la actividad biológica y las vías metabólicas, factores que pueden alterar la respuesta inmunitaria, la dinámica vascular y la remodelación ósea. Además, ciertos métodos de administración exponen directamente los tejidos orales y peri-orales a agresiones físicas, térmicas o químicas, mientras que otros ejercen principalmente efectos sistémicos. Por lo tanto, la vía de administración del cannabis representa una variable importante, aunque a menudo subestimada, al evaluar los riesgos potenciales asociados con la cirugía de implantes y la estabilidad del tejido periimplantario.6 (Figura 1) A continuación se presentan las vías de administración más comunes.
Los métodos de inhalación —incluyendo fumar, vapear y “dabbing”— provocan una absorción sistémica rápida y mayores concentraciones plasmáticas máximas de Δ9 -tetrahidrocannabinol (THC). Sin embargo, estas vías también exponen los tejidos orales y peri-orales a lesiones térmicas, subproductos de la combustión, material particulado y, en algunos casos, solventes residuales, lo que puede contribuir a la irritación mucosa, la vasoconstricción local y la cicatrización deficiente del tejido blando.
Las vías orales de administración, como comestibles, cápsulas y aceites, se caracterizan por un inicio retardado y efectos sistémicos prolongados debido a la absorción gastrointestinal y el metabolismo hepático de primer paso. Estos métodos generalmente implican una exposición mínima directa de los tejidos orales, pero aún pueden ejercer efectos sistémicos sobre la respuesta inmunitaria, la inflamación y el metabolismo óseo relevantes para la cicatrización del implante.
Los sistemas de administración oromucosal y sublingual, incluyendo aerosoles y tinturas, proporcionan una absorción más rápida que la ingestión oral, sin las agresiones térmicas y relacionadas con la combustión asociadas a la inhalación. Aunque ocurre exposición mucosa local, estos métodos pueden causar menos irritación tisular en comparación con fumar o vapear.
El reconocimiento de la vía de administración del cannabis es clínicamente importante, ya que las diferencias en el método de administración, la frecuencia de uso y la composición de cannabinoides (formulaciones dominadas por THC frente a aquellas predominadas por cannabidiol) pueden afectar de manera diferencial la fisiología sistémica y el entorno local periimplantario, esencial para una osteointegración predecible y la estabilidad a largo plazo del tejido blando.7
(Fig.1) Planta de cannabis y productos inhalados de cannabis.
(A) Hojas de *Cannabis sativa* que representan la planta fuente de la cual se derivan los productos médicos y recreativos de cannabis.
(B) Ejemplos de formas inhaladas de cannabis, incluyendo cigarrillos enrollados y flores secas de cannabis, que exponen la cavidad oral y los tejidos periimplantarios al calor, subproductos de la combustión y cannabinoides concentrados que pueden influir en la inflamación oral y la salud periimplantaria.
Implicaciones en implantes dentales
El uso de cannabis puede afectar directamente la terapia con implantes dentales a través de las siguientes vías:
1. Lesión térmica y química
La inhalación de cannabis quemado expone la cavidad oral y los tejidos periimplantarios a una mezcla compleja de irritantes y subproductos tóxicos, incluyendo monóxido de carbono, alquitrán, compuestos orgánicos volátiles e hidrocarburos aromáticos policíclicos —muchos de los cuales se asemejan a los presentes en el humo del tabaco.8 Estas sustancias ejercen efectos citotóxicos y proinflamatorios directos sobre la mucosa oral, deteriorando la función de los fibroblastos y las células epiteliales, esenciales para la reparación del tejido blando y el cierre de la herida. La exposición a estos compuestos aumenta el estrés oxidativo, interrumpe la síntesis y deposición de colágeno e interfiere con la formación de un sello estable de tejido blando alrededor de los implantes dentales.9 Tales alteraciones comprometen la cicatrización mucosa temprana y pueden predisponer los tejidos periimplantarios a la invasión bacteriana.
Estudios preclínicos en animales sugieren que la exposición crónica al humo de cannabis reduce el contacto hueso-implante y disminuye el relleno óseo periimplantario, lo que indica un deterioro del proceso de osteointegración.10 Estos hallazgos sugieren que los componentes térmicos y químicos del humo de cannabis podrían debilitar la fijación del implante y aumentar la susceptibilidad al fracaso biomecánico temprano, subrayando la importancia de abordar los hábitos de inhalación en pacientes sometidos a terapia con implantes.
2. Alteraciones del microbioma oral
El uso de cannabis se ha asociado cada vez más con alteraciones medibles del microbioma oral, y varios estudios demuestran un desplazamiento hacia comunidades microbianas asociadas con enfermedad periodontal y periimplantaria. La exposición regular a cannabinoides —particularmente mediante inhalación— parece promover la colonización y proliferación de especies patógenas como *Porphyromonas gingivalis*, *Tannerella forsythia* y otros organismos anaerobios gramnegativos implicados en la inflamación mucosa periimplantaria y la pérdida de hueso alveolar.11 Estos cambios microbianos pueden estar impulsados en parte por la xerostomía relacionada con el THC, la alteración de la composición salival y los cambios en la inmunidad mucosa, factores que crean un nicho ecológico favorable a la disbiosis. Al agravar este efecto, la inmunomodulación asociada al cannabis —caracterizada por la reducción de la función de neutrófilos, la alteración de la activación de macrófagos y la supresión de vías clave de señalización inflamatoria— disminuye aún más la capacidad del huésped para controlar la formación de biopelículas patógenas. La convergencia de la disbiosis microbiana y la vigilancia inmunitaria deteriorada establece un entorno biológico propicio para la mucositis periimplantaria y su progresión a periimplantitis, lo que representa un riesgo significativo para la estabilidad a largo plazo del implante.12
3. Xerostomía y alteración de la función salival
Se ha demostrado que el uso de cannabis, particularmente productos ricos en Δ9-tetrahidrocannabinol (THC), reduce el flujo salival mediante la inhibición de la estimulación parasimpática de las glándulas salivales mayores. Esta xerostomía inducida por el THC interrumpe las funciones protectoras de la saliva, incluyendo la limpieza mecánica, la capacidad amortiguadora y la actividad antimicrobiana. La disminución de la producción salival resulta en una mayor carga bacteriana oral y facilita la acumulación de placa dental, creando un microambiente que favorece la proliferación y maduración de biopelículas periimplantarias patógenas.13,14 Estos cambios microbianos son clínicamente significativos, ya que las biopelículas asociadas con condiciones de baja saliva tienen mayor probabilidad de albergar patógenos periimplantarios capaces de iniciar o exacerbar la inflamación mucosa. Con el tiempo, esta ecología microbiana alterada contribuye a la inflamación del tejido blando, la pérdida ósea marginal y la destrucción acelerada del tejido periimplantario, comprometiendo así la estabilidad a largo plazo de los implantes dentales. (Figura 2)
(Fig.2) Xerostomía en un paciente con uso regular reportado de THC, que demuestra una disminución en la acumulación salival y mucosa oral seca. La hipofunción salival asociada al THC puede deteriorar los mecanismos de defensa oral y aumentar el riesgo de enfermedad periodontal y periimplantaria.
4. Engrosamiento gingival
Varios investigadores han reportado una asociación entre el uso crónico de cannabis y el engrosamiento gingival. Baddour et al. describieron por primera vez el sobrecrecimiento gingival en individuos con exposición prolongada a marihuana, sugiriendo una posible relación independiente de la inflamación inducida por placa.15 Rawal et al. reportaron hallazgos similares, observando una apariencia gingival característica, rugosa o nodular, sin evidencia de pérdida de inserción clínica en consumidores crónicos de cannabis.16
En contraste, Momen-Heravi et al. describieron un caso de abuso crónico de cannabis asociado con pérdida moderada a severa de inserción periodontal acompañada de engrosamiento gingival periférico, más pronunciado en la mandíbula anterior.17 Estos hallazgos sugieren que los cambios gingivales observados en consumidores de cannabis pueden variar en gravedad y presentación clínica, posiblemente influenciados por la duración del uso, la frecuencia de exposición, el estado de higiene oral y factores de riesgo concurrentes.
Aunque los mecanismos subyacentes aún no se comprenden completamente, las explicaciones propuestas incluyen alteraciones mediadas por cannabinoides en la respuesta inmunitaria, la regulación inflamatoria y la actividad de los fibroblastos gingivales. En conjunto, estos reportes destacan la necesidad de una mayor conciencia clínica sobre los cambios gingivales en pacientes con uso crónico de cannabis, particularmente en el contexto de la terapia periodontal e implantológica.
5. Enfermedad periodontal y periimplantaria
Un creciente cuerpo de investigación epidemiológica y experimental proporciona evidencia biológicamente plausible y clínicamente relevante que vincula el uso de cannabis con resultados adversos periodontales y periimplantarios.18 Estudios poblacionales demuestran consistentemente que los individuos que consumen cannabis presentan una mayor prevalencia y severidad de enfermedad periodontal, incluyendo mayor pérdida de inserción clínica, profundidades de sondaje mayores y destrucción acelerada del hueso alveolar, incluso después de controlar factores de confusión establecidos como el tabaquismo, el consumo de alcohol y el estatus socioeconómico. El uso intenso o crónico de cannabis parece amplificar aún más estos efectos, con individuos afectados que muestran una inflamación gingival más pronunciada y bolsas periodontales más profundas, lo que sugiere una posible relación dosis-respuesta.19,20
Complementando estas observaciones clínicas, modelos experimentales y animales han demostrado que la exposición al humo de cannabis afecta adversamente fases críticas de la curación ósea. Específicamente, la exposición al cannabis se ha asociado con menor relleno óseo, volumen óseo disminuido y contacto hueso-implante reducido durante la osteointegración. Estos hallazgos brindan plausibilidad biológica para una cicatrización comprometida del implante y generan preocupación tanto por el fracaso temprano como tardío del implante.
Más allá de su asociación con la destrucción periodontal, el uso de cannabis también podría contribuir a la pérdida ósea marginal alrededor de los implantes dentales. Evidencia emergente sugiere que los cannabinoides y la exposición al humo de cannabis pueden alterar la remodelación ósea normal al modificar la actividad de osteoblastos y osteoclastos, deteriorar la angiogénesis y modular vías de señalización inflamatoria esenciales para el mantenimiento del hueso periimplantario. Estudios experimentales han demostrado una disminución en la formación ósea, reducción de la densidad ósea y compromiso del contacto hueso-implante en presencia de exposición al humo de cannabis.21 Además, el uso crónico de cannabis podría exacerbar indirectamente la pérdida ósea periimplantaria a través de la disfunción inmunitaria, el aumento de la expresión de citoquinas proinflamatorias y los cambios microbianos dentro del surco periimplantario.22
Aunque los datos clínicos que evalúan específicamente la pérdida ósea marginal del implante en pacientes consumidores de cannabis siguen siendo limitados, la convergencia de hallazgos epidemiológicos, datos experimentales y mecanismos biológicos proporciona una justificación convincente para una mayor preocupación. En conjunto, estos datos sugieren que el uso de cannabis —mediante la modulación inmunitaria, efectos vasculares, disbiosis microbiana y citotoxicidad potencial— podría comprometer tanto los tejidos periodontales naturales como el entorno biológico necesario para una osteointegración predecible y la estabilidad periimplantaria a largo plazo, particularmente en pacientes con exposición intensa o prolongada.23 (Figura 3)
(Fig.3)
(a) Fotografía clínica que demuestra enfermedad periodontal avanzada que afecta la dentición natural, caracterizada por inflamación gingival, pérdida de inserción y destrucción del hueso alveolar. La enfermedad periodontal en consumidores de cannabis ha sido reportada consistentemente en estudios epidemiológicos y está respaldada por mecanismos biológicos que incluyen alteración de la respuesta inmunitaria, xerostomía y disbiosis microbiana.
(b, c) Imágenes clínicas que demuestran inflamación mucosa periimplantaria y pérdida ósea periimplantaria en pacientes con antecedentes de uso crónico de tetrahidrocannabinol (THC). Si bien el cannabis tiene efectos adversos documentados sobre los tejidos periodontales, evidencia emergente sugiere que su impacto biológico podría ser particularmente relevante para los tejidos periimplantarios, donde la modulación inmunitaria, la cicatrización deteriorada y la remodelación ósea alterada podrían aumentar la susceptibilidad a la enfermedad periimplantaria.
6. Efectos sobre la anestesia y la analgesia
El uso de cannabis tiene importantes implicaciones para el manejo perioperatorio en entornos dentales.
Sedación: El uso de cannabis se ha asociado con mayores requerimientos anestésicos tanto en entornos dentales como quirúrgicos. Un metaanálisis reciente reportó que los individuos que consumen cannabis requirieron en promedio 47,33mg más de propofol que los no consumidores, y los pacientes sometidos a anestesia general requirieron 30,57mg adicionales en comparación con los controles. Estos hallazgos sugieren diferencias clínicamente significativas en los requerimientos de dosificación anestésica entre los consumidores de cannabis.24
En el entorno ambulatorio de cirugía oral y maxilofacial, se ha demostrado igualmente que los consumidores de cannabis requieren dosis significativamente mayores de múltiples agentes anestésicos. Específicamente, los consumidores de cannabis recibieron mayores cantidades de propofol (152,5mg vs 117,5mg), midazolam (5,1mg vs 4,7mg), ketamina (46,1mg vs 40,2mg) y fentanilo (88,6µg vs 75,2µg) en comparación con los no consumidores.25
El cannabis también puede interactuar con benzodiacepinas, sedantes y otros agentes que actúan en el sistema nervioso central, lo que resulta en niveles impredecibles de sedación, recuperación retardada o depresión respiratoria potenciada cuando se usan concomitantemente. Además, la exposición perioperatoria al cannabis —particularmente la inhalación reciente de productos ricos en THC— se ha asociado con taquicardia, variabilidad de la presión arterial, ansiedad intensificada, disforia y percepción alterada del dolor en el período postoperatorio.26,27,28
La necesidad de una mayor dosificación anestésica en consumidores de cannabis se considera multifactorial y podría relacionarse con alteraciones inducidas por cannabinoides en la sensibilidad de los receptores del sistema nervioso central, tolerancia farmacodinámica e interacciones con las vías de los receptores de ácido γ-aminobutírico (GABA), N-metil-D-aspartato (NMDA) y opioides. Desde una perspectiva clínica, estos hallazgos subrayan la importancia de la evaluación preoperatoria del uso de cannabis y una vigilancia reforzada durante la planificación de la sedación y la anestesia en procedimientos de implantes dentales y cirugía oral.
Analgesia: La evidencia clínica y experimental disponible indica que el uso de cannabis se asocia con mayores puntuaciones de dolor postoperatorio y mayores requerimientos de opioides en comparación con los no consumidores, lo que sugiere una eficacia analgésica opioide disminuida en esta población. Revisiones sistemáticas y ensayos controlados aleatorizados no han demostrado consistentemente efectos ahorradores de opioides de los cannabinoides en el entorno postoperatorio agudo y, en algunos casos, han reportado una atenuación de la analgesia mediada por opioides.29,30
Además de las preocupaciones sobre la eficacia analgésica, el uso concomitante de cannabinoides y opioides se ha asociado con un mayor riesgo de efectos adversos perioperatorios, incluyendo inestabilidad hemodinámica y depresión aditiva del sistema nervioso central.31,32 Aunque la depresión respiratoria severa no se ha observado consistentemente, la variabilidad en la respuesta del paciente y el potencial de interacciones farmacodinámicas justifican una consideración clínica cuidadosa.
Dado estos hallazgos, los clínicos deben ejercer una precaución significativa al recetar o administrar opioides a pacientes que consumen cannabis, particularmente aquellos con exposición crónica o intensa. Se recomienda la evaluación preoperatoria del uso de cannabis, la planificación analgésica individualizada y un monitoreo postoperatorio reforzado para mitigar riesgos potenciales. Actualmente, la evidencia es insuficiente para respaldar una escalada o reducción rutinaria de la dosis de opioides en esta población, lo que subraya la necesidad de un uso juicioso y estrechamente monitoreado de opioides, así como la consideración de estrategias analgésicas multimodales.33,34
Formas alternativas de cannabis: Comestibles
Aunque los productos comestibles de cannabis no exponen la cavidad oral a los irritantes térmicos o químicos asociados con el cannabis fumado o vaporizado, sus efectos farmacológicos sistémicos aún pueden ser relevantes para la cicatrización periimplantaria. La ingestión oral de cannabis resulta en un inicio retardado pero elevaciones prolongadas de los niveles circulantes de Δ9-tetrahidrocannabinol (THC) debido a la absorción gastrointestinal y el metabolismo hepático de primer paso. Esta exposición sistémica prolongada podría amplificar o prolongar los efectos mediados por cannabinoides sobre la función inmunitaria, la señalización inflamatoria y la regulación vascular.35
Aunque estos efectos no se han evaluado específicamente en poblaciones con implantes dentales, son biológicamente relevantes dadas las funciones esenciales de la vigilancia inmunitaria, la angiogénesis y la integridad microvascular en la osteointegración temprana y la cicatrización del tejido blando. Por lo tanto, la exposición sistémica prolongada a cannabinoides podría tener implicaciones indirectas para la estabilidad del tejido periimplantario, particularmente en pacientes con uso frecuente o en dosis altas de comestibles.36
Además, muchos productos comestibles de cannabis disponibles comercialmente contienen altos niveles de carbohidratos fermentables, lo que podría contribuir al aumento de la acumulación de placa y la formación de biopelículas cariogénicas. En individuos susceptibles, esto podría aumentar indirectamente el riesgo de inflamación mucosa periimplantaria y comprometer la salud periimplantaria a largo plazo.37 Aunque actualmente falta evidencia clínica directa que vincule el uso de comestibles de cannabis con resultados adversos en implantes, estas consideraciones mecanicistas respaldan la inclusión del consumo de comestibles de cannabis en las historias clínicas integrales. Los clínicos deben incorporar esta información en la evaluación individualizada de riesgos, la orientación al paciente y los protocolos de mantenimiento postoperatorio. (Figura 4)
(Fig.4) Los comestibles de cannabis no exponen la cavidad oral al calor ni a irritantes químicos, pero producen una exposición sistémica retardada y prolongada al THC, lo que podría influir en la respuesta inmunitaria, la inflamación y la regulación vascular relevantes para la cicatrización periimplantaria. Además, el alto contenido de azúcar de muchos comestibles podría aumentar la acumulación de placa y contribuir indirectamente a la inflamación mucosa periimplantaria.
Recomendaciones clínicas para los proveedores de implantes
1. Toma integral de la historia clínica
Una historia detallada del uso de cannabis debe incorporarse en cada evaluación de implante, ya que esta información es esencial para anticipar posibles complicaciones intraoperatorias y postoperatorias. Los clínicos deben verificar que el uso de cannabis esté explícitamente incluido en el formulario de admisión médica, ya que muchas prácticas dentales no capturan rutinariamente esta información, lo que lleva a riesgos perioperatorios no reconocidos. La documentación debe incluir la frecuencia, duración y cantidad de consumo de cannabis, así como la vía específica de administración. La estimación de la potencia de THC es importante, ya que las formulaciones concentradas o en aerosol pueden ejercer efectos fisiológicos e inmunológicos más pronunciados. También debe establecerse el momento de la exposición más reciente del paciente al cannabis, dada su influencia en los requerimientos anestésicos y las respuestas perioperatorias. Además, los proveedores deben determinar si el cannabis se usa con fines recreativos o por una indicación médica, ya que las afecciones sistémicas concurrentes o los medicamentos psicotrópicos concomitantes podrían influir aún más en el riesgo quirúrgico y la planificación del tratamiento. (Figura 5)
(Fig.5) Cuestionario médico específico para cannabis.
Ejemplo de un formulario de admisión utilizado para documentar el uso de cannabis, incluyendo frecuencia, vía de administración, duración y potencia, para apoyar la evaluación de riesgos y la toma de decisiones clínicas en el cuidado de implantes.
2. Estratificación de riesgo preoperatorio
Tras obtener la historia clínica, los clínicos deben evaluar los factores de riesgo individuales que podrían predisponer a los pacientes consumidores de cannabis a complicaciones periimplantarias. Los fumadores o vapeadores diarios de cannabis, así como los usuarios de concentrados de alta potencia, podrían exhibir un mayor deterioro en la función inmunitaria, la perfusión vascular y el metabolismo óseo. Los pacientes con enfermedad periodontal preexistente constituyen un grupo de riesgo particularmente alto, ya que la inflamación periodontal se asocia fuertemente con resultados periimplantarios adversos. Las personas con xerostomía o prácticas de higiene oral subóptimas también deben considerarse en riesgo elevado, ya que el flujo salival reducido y el control inadecuado de la placa promueven el desarrollo de biopelículas patógenas capaces de acelerar la destrucción mucosa y ósea periimplantaria.
3. Recomendaciones de cesación de cannabis
Actualmente, no existen pautas perioperatorias basadas en evidencia que aborden específicamente la cesación de cannabis en pacientes sometidos a cirugía de implantes dentales. Sin embargo, las recomendaciones pueden extrapolarse razonablemente de datos establecidos sobre cicatrización de heridas, reactividad vascular, modulación inmunitaria y los efectos conocidos de los combustibles inhalados sobre los resultados postoperatorios. Basándose en estos principios, se aconseja que los pacientes se abstengan del uso de cannabis durante todo el período perioperatorio —definido como aproximadamente una semana antes de la colocación del implante y un mínimo de cuatro semanas posteriores a la cirugía— para optimizar la oxigenación tisular, reducir la carga inflamatoria, estabilizar las respuestas cardiovasculares y apoyar la osteointegración temprana.
Para las personas que usan cannabis bajo supervisión médica para una indicación terapéutica definida, cualquier modificación perioperatoria de su régimen debe abordarse con cautela. En tales casos, se debe consultar al médico prescriptor para evaluar la seguridad de la cesación temporal o el ajuste de la dosis. La toma de decisiones colaborativa es esencial para garantizar que la reducción del riesgo perioperatorio no comprometa el manejo de la afección subyacente para la cual se recetó el cannabis. Este enfoque interdisciplinario permite una planificación individualizada del tratamiento mientras prioriza la seguridad quirúrgica y una integración predecible del implante.
4. Consentimiento informado
El consentimiento informado (verbal y escrito) es un componente crítico del proceso de planificación preoperatoria para garantizar que los pacientes comprendan los riesgos del uso de THC y del procedimiento de implante previsto.
a. Verbal
Riesgos específicos: Dado el rápido aumento de formulaciones de THC de alta potencia y sistemas de administración concentrados, los clínicos deben enfatizar que el impacto a largo plazo de estos productos sobre la supervivencia del implante sigue siendo insuficientemente concluyente; sin embargo, la evidencia actual sugiere el potencial de efectos adversos. Por lo tanto, el proceso de consentimiento debe incluir la discusión del riesgo de fracasos tempranos relacionados con la osteointegración deteriorada y fracasos tardíos asociados con inflamación periimplantaria o pérdida ósea. Los pacientes deben ser conscientes de que estas complicaciones podrían requerir intervenciones adicionales, incluyendo revisión quirúrgica, injertos o reemplazo del implante.
Presencia de testigo independiente: Idealmente, un testigo (miembro del personal) debe estar presente y documentar (en el formulario de consentimiento) la confirmación de que el paciente fue plenamente informado.
b. Escrito
Se debe obtener un formulario de consentimiento informado escrito y completo, que detalle explícitamente los riesgos específicos que el THC representa para el proceso de implante dental. Este documento debe describir claramente las complicaciones potenciales asociadas con estos productos, incluyendo osteointegración deteriorada, mayor riesgo de fracaso del implante y cicatrización retardada. Para garantizar una decisión informada, los pacientes deben revisar y firmar el formulario de consentimiento (documentando el reconocimiento del paciente) antes del procedimiento programado. Este proceso permite suficiente tiempo para que el paciente comprenda plenamente los riesgos asociados y obtenga aclaraciones sobre cualquier inquietud. (Figura 6)
(Fig.6) Formulario de consentimiento informado del Instituto de Implantes Resnik para cannabis/tabaco:
Ejemplo representativo de documentos escritos de consentimiento informado utilizados para revelar los riesgos potenciales asociados con el uso de cannabis y tabaco en la terapia con implantes dentales, incluyendo osteointegración deteriorada, cicatrización retardada y mayor riesgo de complicaciones del implante.
5. Protocolos postoperatorios mejorados
Dado que los consumidores de cannabis podrían tener un mayor riesgo de inflamación periimplantaria y complicaciones en la cicatrización, se recomiendan protocolos modificados de cuidado postoperatorio. Podrían ser necesarias visitas de seguimiento más frecuentes y citas profesionales de higiene para manejar la biopelícula de placa durante la fase temprana de cicatrización. Los enjuagues antimicrobianos complementarios, como la clorhexidina, podrían ser beneficiosos para reducir la carga bacteriana y apoyar la salud mucosa. Se debe proporcionar educación detallada sobre los métodos diarios de control de placa, enfatizando la importancia de la interrupción mecánica de la biopelícula alrededor de los implantes. Para pacientes con xerostomía relacionada con el cannabis, se pueden implementar estrategias de manejo —como mayor hidratación, estimulantes salivales o sustitutos salivales— para mejorar la limpieza oral y apoyar la estabilidad del tejido periimplantario.
Conclusión
La exposición al cannabis representa una variable clínica cada vez más relevante en la implantología dental, impulsada por la creciente prevalencia, el aumento de la potencia de los productos y el uso generalizado de sistemas de administración por inhalación. La evidencia actual demuestra que el cannabis —particularmente cuando se fuma o se vapea— puede afectar adversamente múltiples vías fisiológicas esenciales para el éxito del implante, incluyendo la cicatrización del tejido blando, la función salival, la vigilancia inmunitaria, la regulación vascular y la remodelación ósea. Estos efectos biológicos crean un entorno más permisivo para la inflamación periimplantaria, aceleran la maduración de la biopelícula y podrían deteriorar la osteointegración temprana, aumentando así la probabilidad tanto de complicaciones tempranas como tardías del implante.
Aunque los datos clínicos definitivos a largo plazo siguen siendo limitados, los hallazgos mecanicistas y preclínicos, combinados con asociaciones epidemiológicas consistentes con la enfermedad periodontal, justifican un enfoque preventivo en la planificación del tratamiento. Por lo tanto, la evaluación rutinaria del uso de cannabis debe incorporarse en la historia clínica de cada paciente con implante, prestando especial atención a la frecuencia, la vía de administración y el momento de la última exposición. La estratificación de riesgos, las recomendaciones de cesación perioperatoria, el mantenimiento postoperatorio mejorado y un consentimiento informado exhaustivo son componentes críticos de la atención basada en evidencia en esta población.
A medida que la legalización continúa ampliando el acceso y proliferan nuevas formulaciones de alta potencia, la comunidad dental debe permanecer atenta a los datos científicos en evolución y refinar los protocolos clínicos en consecuencia. Reconocer el uso de cannabis como un modificador de riesgo significativo —y abordarlo de manera proactiva mediante la comunicación interdisciplinaria, la educación del paciente y el manejo perioperatorio personalizado— será esencial para garantizar resultados seguros, predecibles y duraderos en la terapia con implantes dentales.
References
Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: Results from the 2021 National Survey on Drug Use and Health (HHS Publication No. PEP22-07-01-005, NSDUH Series H-57). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. 2022. https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report. Accessed on February 9, 2024.
Hasin DS, Saha TD, Kerridge BT, et al. Prevalence of marijuana use disorders in the United States between 2001-2002 and 2012-2013. JAMA Psychiatry. 2015 Dec;72(12):1235-1242. doi: 10.1001/jamapsychiatry.2015.1858.
Mims MM, Parikh AC, Sandhu Z, DeMoss N, Mhawej R, Queimado L. Surgery-Related Considerations in Treating People Who Use Cannabis: A Review. JAMA Otolaryngol Head Neck Surg. 2024 Oct 1;150(10):918-924. doi: 10.1001/jamaoto.2024.2545. PMID: 39172477.
Nogueira-Filho Gda R, Cadide T, Rosa BT, Neiva TG, Tunes R, Peruzzo D, Nociti FH Jr, César-Neto JB. Cannabis sativa smoke inhalation decreases bone filling around titanium implants: a histomorphometric study in rats. Implant Dent. 2008 Dec;17(4):461-70. doi: 10.1097/ID.0b013e31818c5a2a. PMID: 19077584.
Nogueira-Filho GR, Todescan S, Shah A, Rosa BT, Tunes Uda R, Cesar Neto JB. Impact of cannabis sativa (marijuana) smoke on alveolar bone loss: a histometric study in rats. J Periodontol. 2011 Nov;82(11):1602-7. doi: 10.1902/jop.2011.100362. Epub 2011 Mar 29. PMID: 21513470.
Pulvers K, Jamalian N, Suh E, Faltaoos P, Stewart SL, Aston ER. Nicotine and cannabis routes of administration and dual use among U.S. young adults who identify as Hispanic, non-Hispanic Black, and non-Hispanic White. Prev Med Rep. 2024 Oct 22;48:102912. doi: 10.1016/j.pmedr.2024.102912. PMID: 39526216; PMCID: PMC11550767.
Singh, H., J. Katz, W. Saleh, and S. Cha. "Impact of cannabis on the port of entry-oral tissues: an overview." Int J Oral Dent Health 5, no. 3 (2019): 1-5.
Graves BM, Johnson TJ, Nishida RT, Dias RP, Savareear B, Harynuk JJ, Kazemimanesh M, Olfert JS, Boies AM. Comprehensive characterization of mainstream marijuana and tobacco smoke. Sci Rep. 2020 Apr 28;10(1):7160. doi: 10.1038/s41598-020-63120-6. PMID: 32345986; PMCID: PMC7188852.
Moir D, Rickert WS, Levasseur G, Larose Y, Maertens R, White P, Desjardins S. A comparison of mainstream and sidestream marijuana and tobacco cigarette smoke produced under two machine smoking conditions. Chem Res Toxicol. 2008 Feb;21(2):494-502. doi: 10.1021/tx700275p. Epub 2007 Dec 7. PMID: 18062674.
Nogueira-Filho Gda R, Cadide T, Rosa BT, Neiva TG, Tunes R, Peruzzo D, Nociti FH Jr, César-Neto JB. Cannabis sativa smoke inhalation decreases bone filling around titanium implants: a histomorphometric study in rats. Implant Dent. 2008 Dec;17(4):461-70. doi: 10.1097/ID.0b013e31818c5a2a. PMID: 19077584.
Scott DA, Dukka H, Saxena D. Potential Mechanisms Underlying Marijuana-Associated Periodontal Tissue Destruction. J Dent Res. 2022 Feb;101(2):133-142. doi: 10.1177/00220345211036072. Epub 2021 Sep 13. PMID: 34515556; PMCID: PMC8905217.
Gu Z, Singh S, Niyogi RG, Lamont GJ, Wang H, Lamont RJ, Scott DA. Marijuana-Derived Cannabinoids Trigger a CB2/PI3K Axis of Suppression of the Innate Response to Oral Pathogens. Front Immunol. 2019 Oct 15;10:2288. doi: 10.3389/fimmu.2019.02288. PMID: 31681262; PMCID: PMC6804395.
McConnell WR, Dewey WL, Harris LS, Borzelleca JF. A study of the effect of delta 9-tetrahydrocannabinol (delta 9-THC) on mammalian salivary flow. J Pharmacol Exp Ther. 1978 Sep;206(3):567-73. PMID: 702321.
Baddour HM, Audemorte TB, Layman FD (1984) The occurrence of diffuse gingival hyperplasia in a patient using marijuana. J Tenn Dent Assoc 64: 39-43.
Rawal SY, Tatakis DN, Tipton DA (2012) Periodontal and oral manifestations of marijuana use. J Tenn Dent Assoc 92: 26-31.
Momen-Heravi F, Kang P (2017) Management of cannabisinduced periodontitis via resective surgical therapy: A clinical report. J Am Dent Assoc 148: 179-184.
Chisini LA, Cademartori MG, Francia A, Mederos M, Grazioli G, Conde MCM, Correa MB. Is the use of Cannabis associated with periodontitis? A systematic review and meta-analysis. J Periodontal Res. 2019 Aug;54(4):311-317. doi: 10.1111/jre.12639. Epub 2019 Jan 24. PMID: 30677134.
Shariff JA, Ahluwalia KP, Papapanou PN. Relationship Between Frequent Recreational Cannabis (Marijuana and Hashish) Use and Periodontitis in Adults in the United States: National Health and Nutrition Examination Survey 2011 to 2012. J Periodontol. 2017 Mar;88(3):273-280. doi: 10.1902/jop.2016.160370. Epub 2016 Oct 8. PMID: 27718772.
Thomson WM, Poulton R, Broadbent JM, Moffitt TE, Caspi A, Beck JD, Welch D, Hancox RJ. Cannabis smoking and periodontal disease among young adults. JAMA. 2008 Feb 6;299(5):525-31. doi: 10.1001/jama.299.5.525. PMID: 18252882; PMCID: PMC2823391.
Nogueira-Filho Gda R, Cadide T, Rosa BT, Neiva TG, Tunes R, Peruzzo D, Nociti FH Jr, César-Neto JB. Cannabis sativa smoke inhalation decreases bone filling around titanium implants: a histomorphometric study in rats. Implant Dent. 2008 Dec;17(4):461-70. doi: 10.1097/ID.0b013e31818c5a2a. PMID: 19077584.
Nogueira‐Filho, Getulio R., Sylvia Todescan, Adnan Shah, Bruno T. Rosa, Urbino da R. Tunes, and Joao B. Cesar Neto. "Impact of cannabis sativa (marijuana) smoke on alveolar bone loss: a histometric study in rats." Journal of periodontology 82, no. 11 (2011): 1602-1607.
Qi X, Liu C, Li G, Al-Alfe D, Paurazas S, Askar M, Yang D, Zhou Z. Evaluation of Cannabinoids on the Odonto/Osteogenesis in Human Dental Pulp Cells In Vitro. J Endod. 2021 Mar;47(3):444-450. doi: 10.1016/j.joen.2020.12.005. Epub 2021 Jan 20. PMID: 33352148.
Baker MB, Binda DD, Nozari A, Kennedy JM, Dienes E, Baker WE. Quantitative Analysis of Propofol Dosage in Cannabis Users: A Systematic Review and Meta-Analysis. J Clin Med. 2025 Jan 28;14(3):858. doi: 10.3390/jcm14030858. PMID: 39941531; PMCID: PMC11818839.
Ripperger D, Atte A, Ritto F. Cannabis Users Require More Anesthetic Agents for General Anesthesia in Ambulatory Oral and Maxillofacial Surgery Procedures. J Oral Maxillofac Surg. 2023 Dec;81(12):1460-1465. doi: 10.1016/j.joms.2023.09.008. Epub 2023 Sep 14. PMID: 37783364.
Shah S, Schwenk ES, Sondekoppam RV, Clarke H, Zakowski M, Rzasa-Lynn RS, Yeung B, Nicholson K, Schwartz G, Hooten WM, Wallace M, Viscusi ER, Narouze S. ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids. Reg Anesth Pain Med. 2023 Mar;48(3):97-117. doi: 10.1136/rapm-2022-104013. Epub 2023 Jan 3. PMID: 36596580.
Echeverria-Villalobos M, Fabian CA, Mitchell JG, Mazzotta E, Fiorda Diaz JC, Noon K, Weaver TE. Cannabinoids and General Anesthetics: Revisiting Molecular Mechanisms of Their Pharmacological Interactions. Anesth Analg. 2025 Jun 1;140(6):1401-1413. doi: 10.1213/ANE.0000000000007313. Epub 2024 Nov 6. PMID: 39504269; PMCID:
Mims, Mark M., Aniruddha C. Parikh, Zainab Sandhu, Noah DeMoss, Rachad Mhawej, and Lurdes Queimado. "Surgery-related considerations in treating people who use cannabis: a review." JAMA Otolaryngology–Head & Neck Surgery (2024).
Ekrami E, Sari S, Kopac O, Wang D, Mascha EJ, Stamper S, Esa WAS, Nair H, Ruetzler K, Turan A. Association Between Cannabis Use and Opioid Consumption, Pain, and Respiratory Complications After Surgery: A Retrospective Cohort Analysis. Anesth Analg. 2024 Oct 1;139(4):724-733. doi: 10.1213/ANE.0000000000006785. Epub 2024 Jan 8. PMID: 38190341.
King DD, Temmermand R, Greenwood JE. Preoperative cannabinoid exposure and postoperative pain: A narrative review. J Clin Anesth. 2025 Dec 16;109:112097. doi: 10.1016/j.jclinane.2025.112097. Epub ahead of print. PMID: 41406677.
Shah, Shalini, Eric S. Schwenk, Rakesh V. Sondekoppam, Hance Clarke, Mark Zakowski, Rachel S. Rzasa-Lynn, Brent Yeung et al. "ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids." Regional Anesthesia & Pain Medicine 48, no. 3 (2023): 97-117.
Guy D, Wootten JC, Wong M, Turski D, Lukewich M, Alboog A, Kandasamy AR, Gregory J, Poolacherla R. Pharmacodynamic effects following co-administration of cannabinoids and opioids: a scoping review of human experimental studies. Pain Med. 2024 Jul 1;25(7):423-434. doi: 10.1093/pm/pnae024. PMID: 38561178.
Echeverria-Villalobos M, Todeschini AB, Stoicea N, Fiorda-Diaz J, Weaver T, Bergese SD. Perioperative care of cannabis users: A comprehensive review of pharmacological and anesthetic considerations. J Clin Anesth. 2019 Nov;57:41-49. doi: 10.1016/j.jclinane.2019.03.011. Epub 2019 Mar 7. PMID: 30852326.
Shah, Shalini, Eric S. Schwenk, Rakesh V. Sondekoppam, Hance Clarke, Mark Zakowski, Rachel S. Rzasa-Lynn, Brent Yeung et al. "ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids." Regional Anesthesia & Pain Medicine 48, no. 3 (2023): 97-117.
Whiting, Penny F., Robert F. Wolff, Sohan Deshpande, Marcello Di Nisio, Steven Duffy, Adrian V. Hernandez, J. Christiaan Keurentjes et al. "Cannabinoids for medical use: a systematic review and meta-analysis." JAMA 313, no. 24 (2015): 2456-2473.
Schlienz NJ, Spindle TR, Cone EJ, Herrmann ES, Bigelow GE, Mitchell JM, Flegel R, LoDico C, Vandrey R. Pharmacodynamic dose effects of oral cannabis ingestion in healthy adults who infrequently use cannabis. Drug Alcohol Depend. 2020 Jun 1;211:107969. doi: 10.1016/j.drugalcdep.2020.107969. Epub 2020 Mar 21. PMID: 32298998; PMCID: PMC8221366.
Le A, Khoo E, Palamar JJ. Associations between Oral Health and Cannabis Use among Adolescents and Young Adults: Implications for Orthodontists. Int J Environ Res Public Health. 2022 Nov 18;19(22):15261. doi: 10.3390/ijerph192215261. PMID: 36429978; PMCID: PMC9691037.