1) Kameda Dental Clinic
2) The Academy of Clinical Dentistry
3) Department of Periodontology, School of Life Dentistry, Nippon Dental University
4) Department of Comprehensive Dentistry, Nippon Dental University Hospital
Abstract
This study aimed to investigate the prevalence of peri-implant diseases and associated risk factors among patients treated in general dental practices in Japan. A total of 514 dental implants in 163 patients (94 females), with a mean age of 63.6 years, who attended maintenance appointments at five general dental clinics were included. Patient background characteristics and potential risk factors were recorded through clinical charts and interviews during maintenance visits. Additionally, clinical periodontal and peri-implant examinations and Radiographic assessment were performed. The prevalence of peri-implant mucositis and peri-implantitis was calculated on an implant-level basis. Multivariate logistic regression analysis was conducted to evaluate the association between patient background factors, risk indicators, and peri-implantitis.
The prevalence of peri-implant mucositis ranged from 9.53% to 17.51%, while that of peri-implantitis ranged from 3.11% to 11.89%, depending on diagnostic criteria. Multivariate logistic regression analysis revealed that a rough surface topography of the implant body was significantly associated with peri-implantitis, with an odds ratio of 4.85. In conclusion, among implant patients undergoing regular maintenance in general dental practices, the implant-level prevalence of peri-implant diseases was relatively low, and a rough implant surface was significantly correlated with peri-implantitis.
Key words:Peri-implantitis, Peri-implant mucositis, Dental implants, Prevalence, Risk factors, Maintenance, Implant surface, General dental practice
I. Introduction
Inflammatory conditions affecting the tissues surrounding dental implants can be classified into two categories: peri-implant mucositis and peri-implantitis¹). Peri-implant mucositis is characterized by inflammation limited to the peri-implant mucosa without radiographic evidence of marginal bone loss, whereas peri-implantitis involves inflammatory destruction extending to the supporting bone, resulting in progressive alveolar bone resorption. The primary etiological factor for peri-implant diseases is bacterial biofilm accumulation.1 Pathogenic periodontal bacteria have been frequently detected at sites affected by peri-implantitis.2 However, there are structural and biological differences between natural dentition and peri-implant tissues. While inflammation in periodontal tissues is typically confined within the connective tissue, inflammatory processes around implants may rapidly extend to the bone–implant interface.3 Unlike periodontal tissues, peri-implant tissues lack a periodontal ligament and have relatively poor vascularity, which may compromise host defense mechanisms. As a result, once microbial infection leads to disruption at the implant–bone interface, even slow-progressing bone resorption may become self-sustaining. These fundamental differences necessitate lifelong maintenance therapy following implant placement.4
Despite regular maintenance, peri-implant diseases may still develop and represent a major cause of implant failure. A meta-analysis by Lee et al.5 reported a patient-level prevalence of peri-implantitis of 19.83% and an implant-level prevalence of 9.25%. However, most data included in such analyses originate from specialized centers, reflecting outcomes under optimal treatment conditions. Therefore, to obtain more generalizable findings, epidemiological studies conducted in routine general practice settings are essential. In our first report, we demonstrated that among patients maintained in general clinical practice, the patient-level prevalence of peri-implant mucositis was 23.9% and that of peri-implantitis was 15.8%, with a history of periodontitis-related tooth loss and smoking identified as significant risk factors.6
The present study aims to analyze the prevalence of peri-implant diseases at the implant level and identify associated risk factors within a general dental practice setting.
II. Subjects and Methods
This study was approved by the Ethics Committee of The Academy of Clinical Dentistry (Approval No. 22-003). Written informed consent was obtained from all participants. The study design combined a retrospective review of patient records with a cross-sectional assessment based on clinical examination, radiographic evaluation, and data collected via interviews during maintenance visits.
A total of 514 dental implants in 163 patients (mean age: 63.6 years, 94 females) attending five general dental clinics across Japan for maintenance between July 2021 and July 2022 were included. All implants had been functionally loaded for at least one year prior to examination. Patients who had taken systemic antibiotics within three months prior to the examination were excluded.
Clinical Examination
At the time of maintenance visit, the following parameters were recorded for each implant:
- Probing pocket depth (PPD)
- Bleeding on probing (BOP) or suppuration (S)
- Plaque score
- Radiographic marginal bone level (MBL)
Clinical measurements were performed using a plastic periodontal probe. PPD and BOP were assessed at six sites per implant: mesiobuccal, midbuccal, distobuccal, distolingual, midlingual, and mesiolingual, with readings recorded in millimeters. Plaque scores were recorded after disclosing agent application at four aspects: mesial, buccal, distal, and lingual.
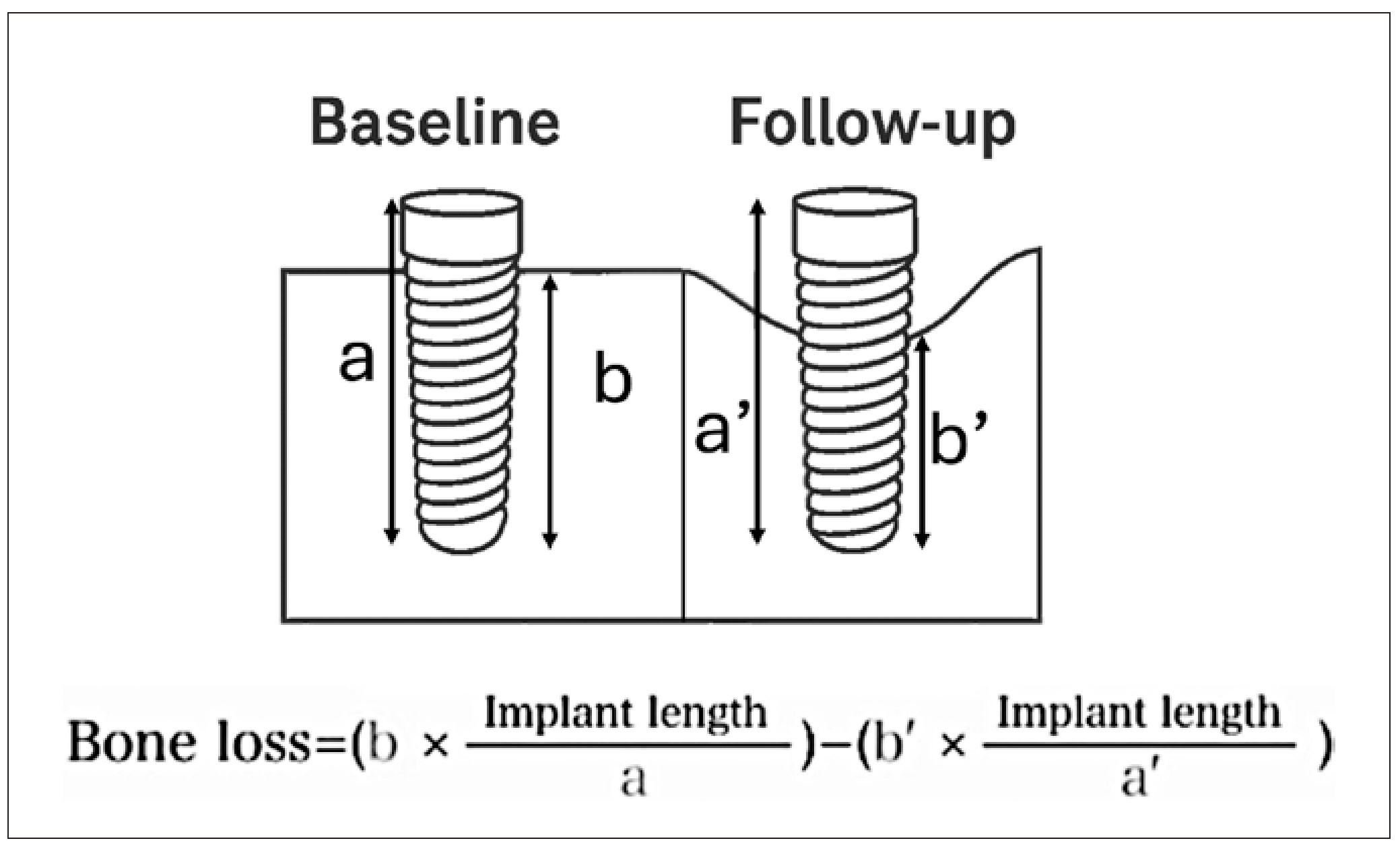
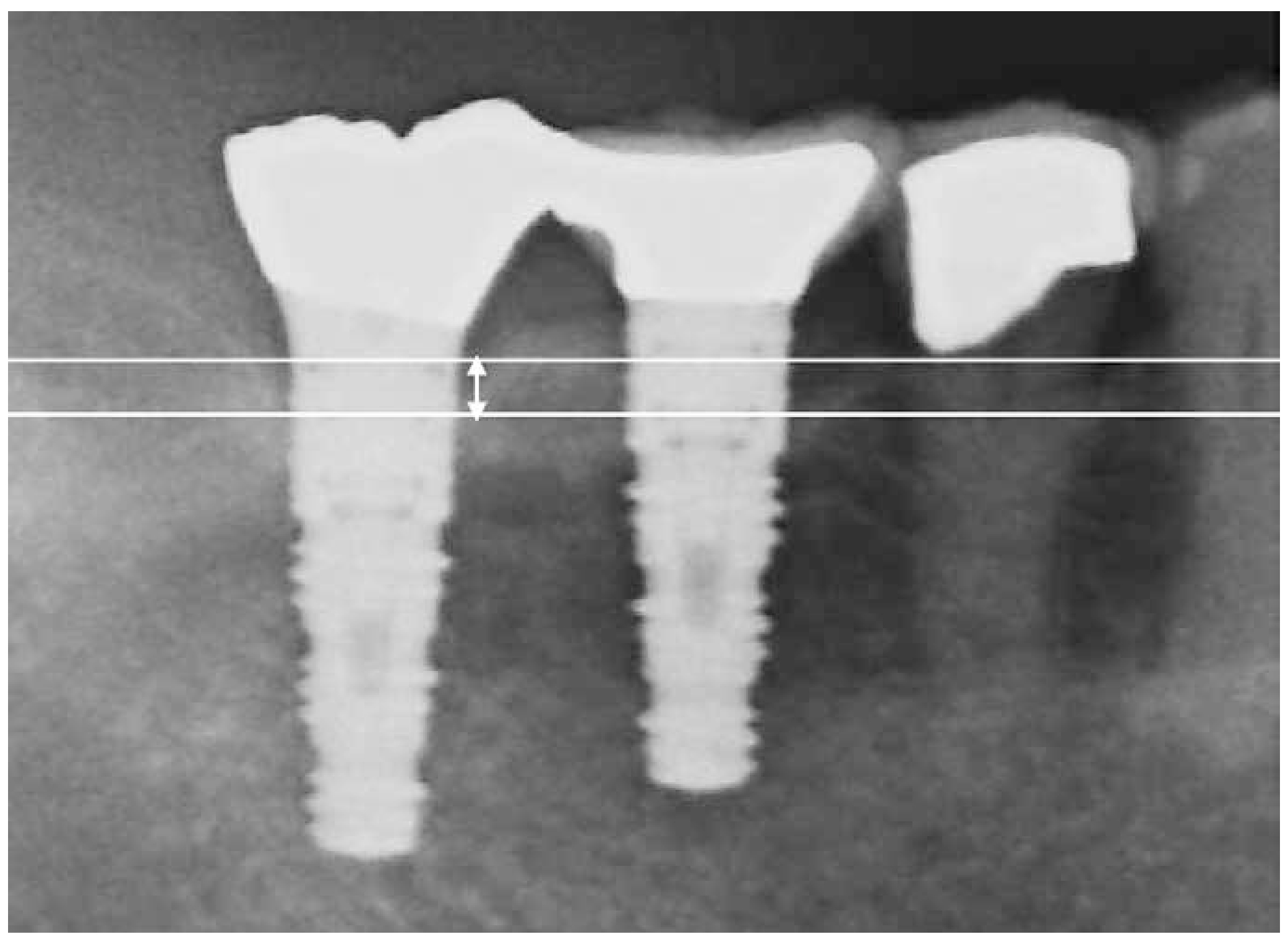
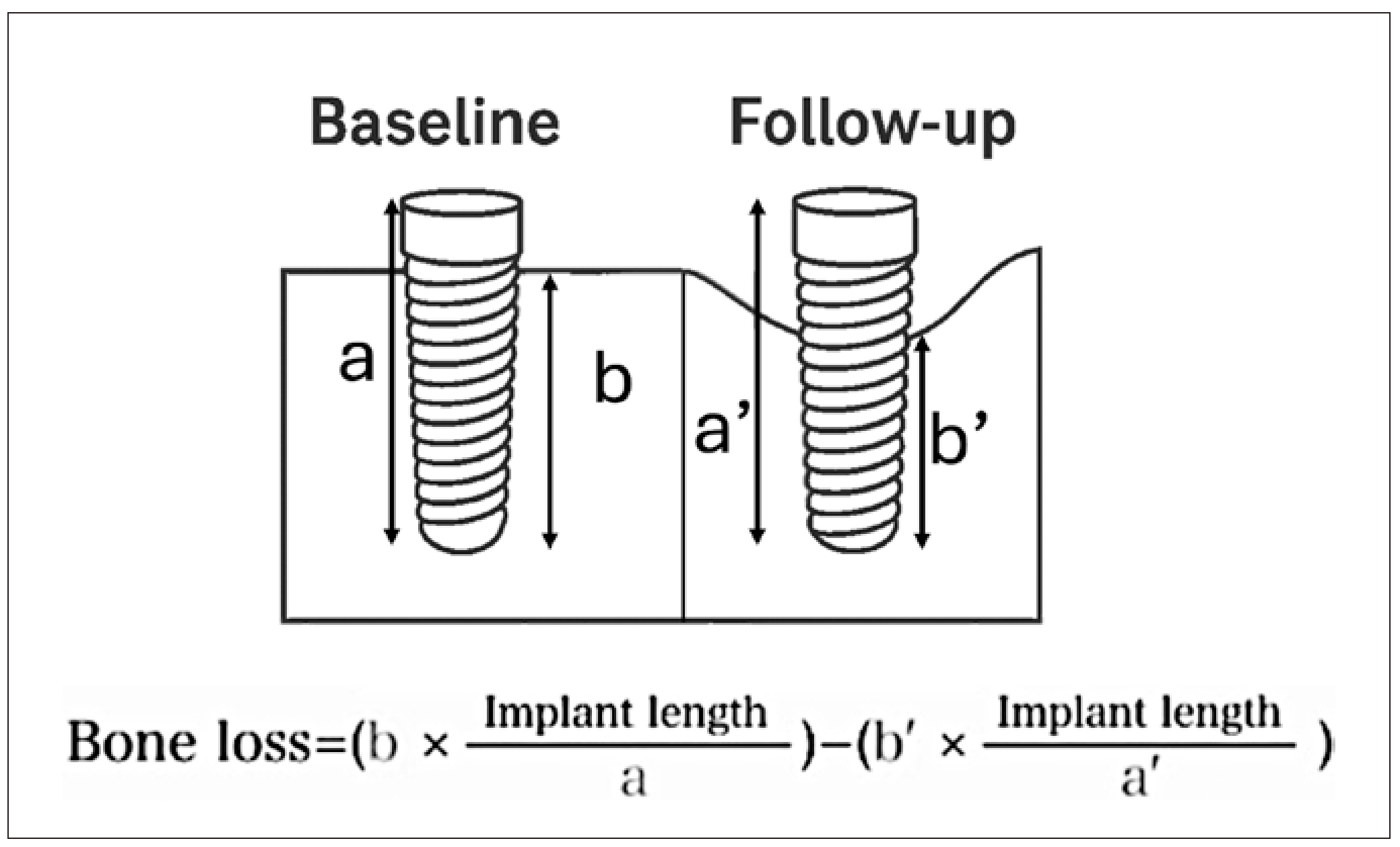
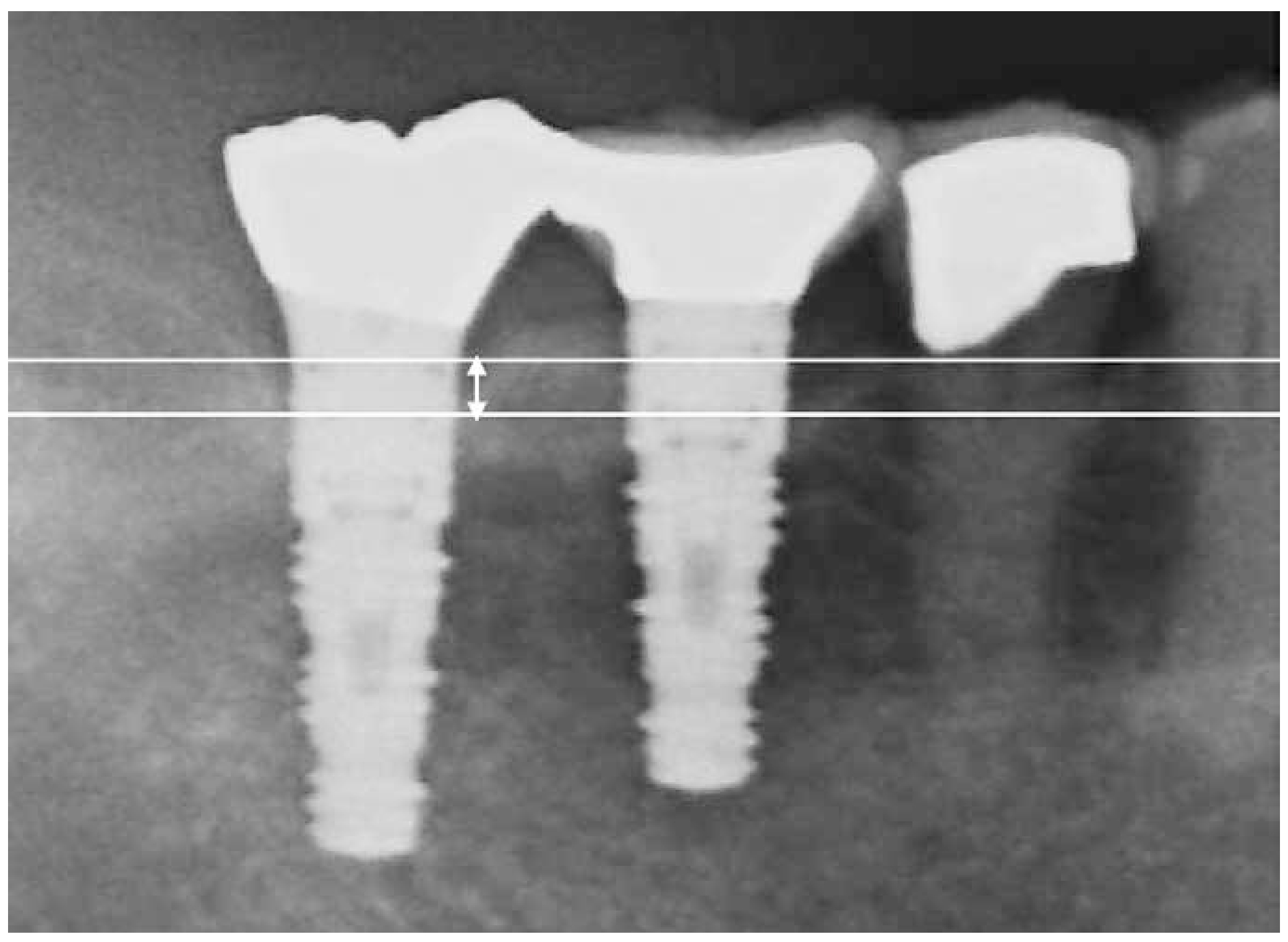
Radiographic images were acquired using either a dental X-ray unit with a long-cone paralleling technique or a panoramic radiograph. Bone volume was calculated by measuring the distance from the marginal bone level to the implant apex (a), and the implant length (b). The ratio of (b/a) was used to estimate relative bone volume. Baseline bone volume was defined as the radiographic measurement taken one year after prosthetic loading. The difference between baseline and current bone volume was defined as marginal bone loss.7,8 (Figure 1: Criterion 1). Alternatively, as Criterion 2, the vertical distance from the marginal bone crest to the base of the intrabony defect was measured as the bone defect depth (Figure 2: length of white arrow).
(Fig.1) Criterion 1(Fig.2) Criterion 2.The white arrow indicates the amount of bone loss, defined as the distance from the bone crest to the base of the bone defect.
For natural teeth, full-mouth recordings of PPD, BOP, suppuration, plaque control record (PCR), and Eichner classification were obtained.
Diagnostic Criteria
Diagnoses were made using modified definitions based on the 2018 consensus report on peri-implant diseases.4 :
Peri-Implant Mucositis
Presence of BOP or suppuration, with less than 1 mm of marginal bone loss.
Peri-Implantitis
Two diagnostic criteria were applied:
- Criterion 1: Presence of BOP or suppuration, with ≥1 mm of marginal bone loss compared to baseline (1 year post-loading).
- Criterion 2: Presence of BOP or suppuration, with PPD ≥6 mm and bone defect depth ≥3 mm observed on current radiographs.
Statistical Analysis
Descriptive statistics were computed for all variables, including mean ± standard deviation for continuous variables and frequencies for categorical variables, at the implant level. Data were stratified by time since prosthetic loading (<5 years, 5–10 years, >10 years), and group comparisons were performed using one-way ANOVA for continuous variables and Chi-square tests for categorical data.
The prevalence of healthy peri-implant tissues, peri-implant mucositis, and peri-implantitis was calculated according to each diagnostic criterion. Patient background characteristics and clinical parameters of natural dentition were compared across diagnostic groups using one-way ANOVA or Chi-square tests, as appropriate.
To assess the association between potential risk factors and peri-implantitis, multivariate logistic regression models were employed. The outcome variables were categorized as: healthy implant, peri-implant mucositis, or peri-implantitis. Two models were constructed: one with "peri-implant disease" (mucositis + peri-implantitis) as the outcome, and another with "peri-implantitis" as the primary outcome, using healthy implants (and in some models, healthy + mucositis) as reference. Independent variables included patient demographics, systemic factors, and clinical parameters showing the strongest bivariate associations with disease. Adjusted odds ratios (aOR) and 95% confidence intervals (CI) were calculated to determine statistical significance.
III. Results
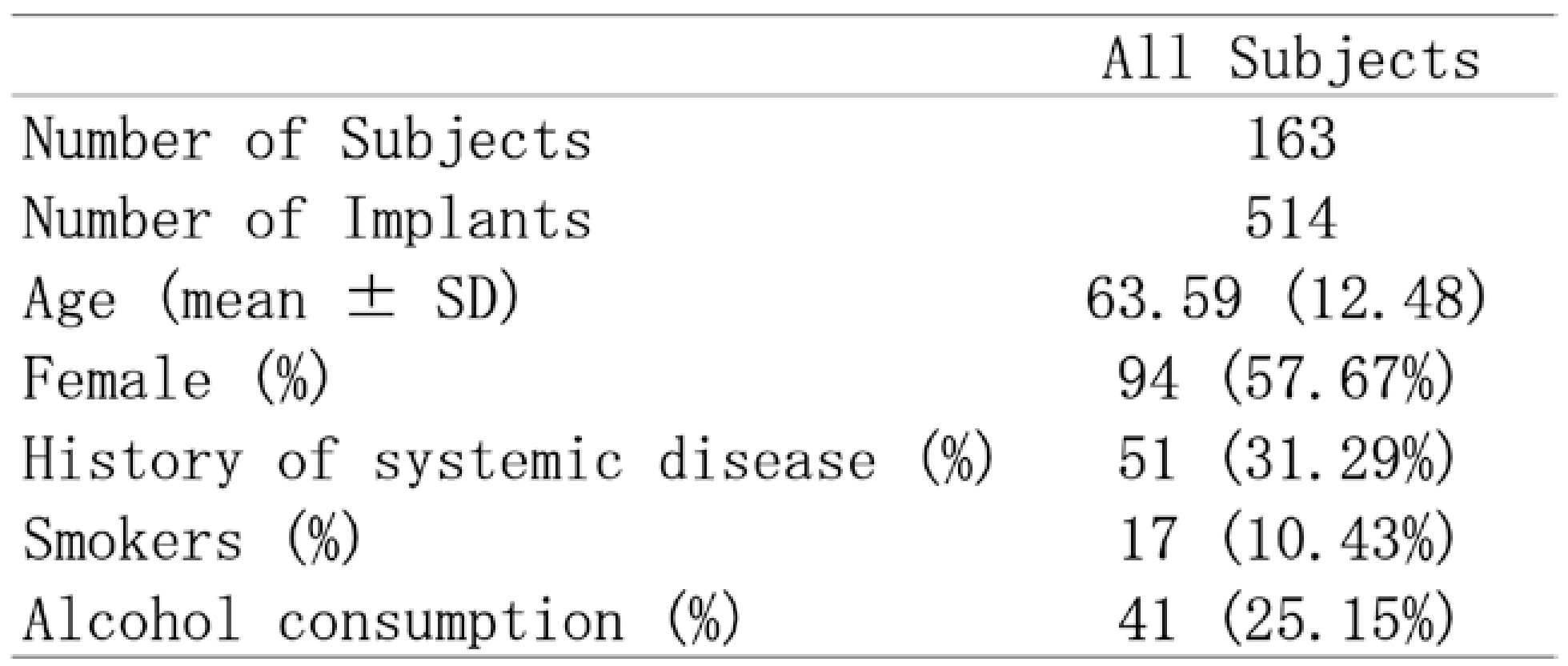
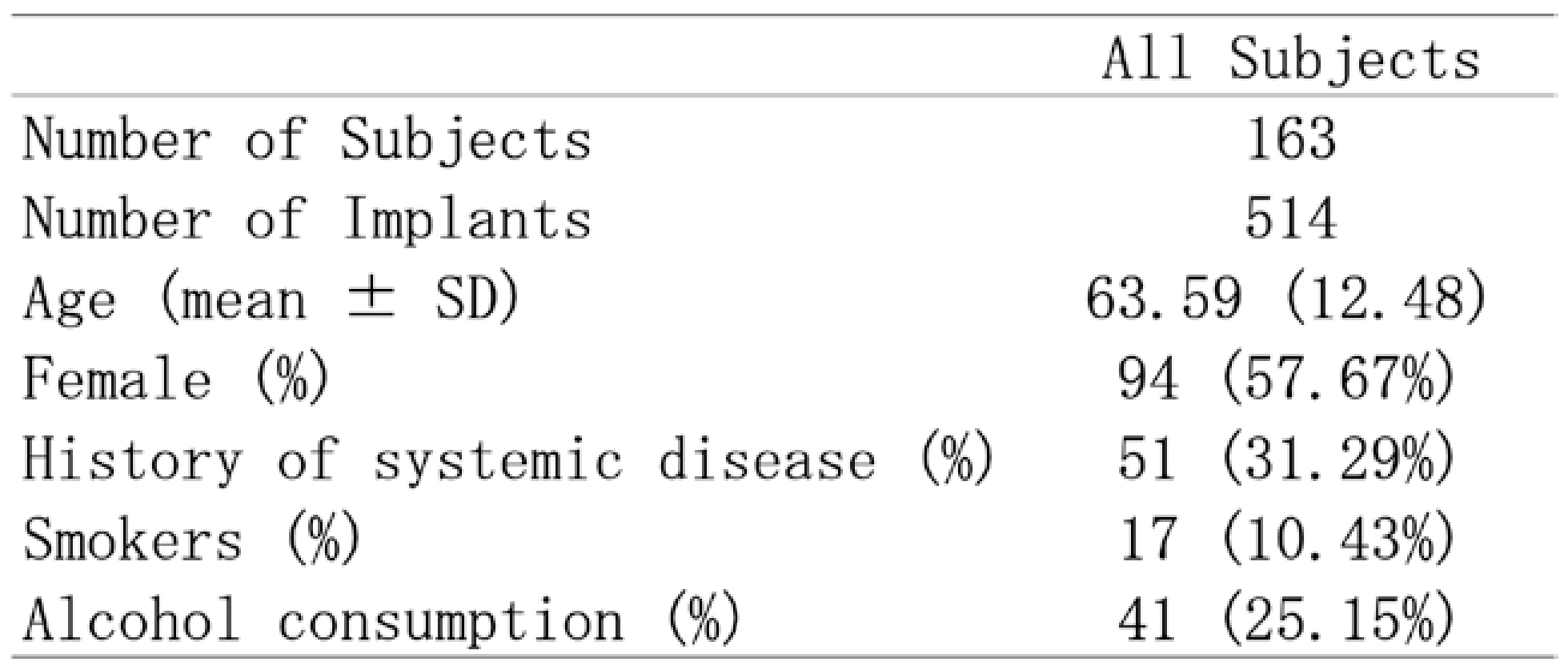
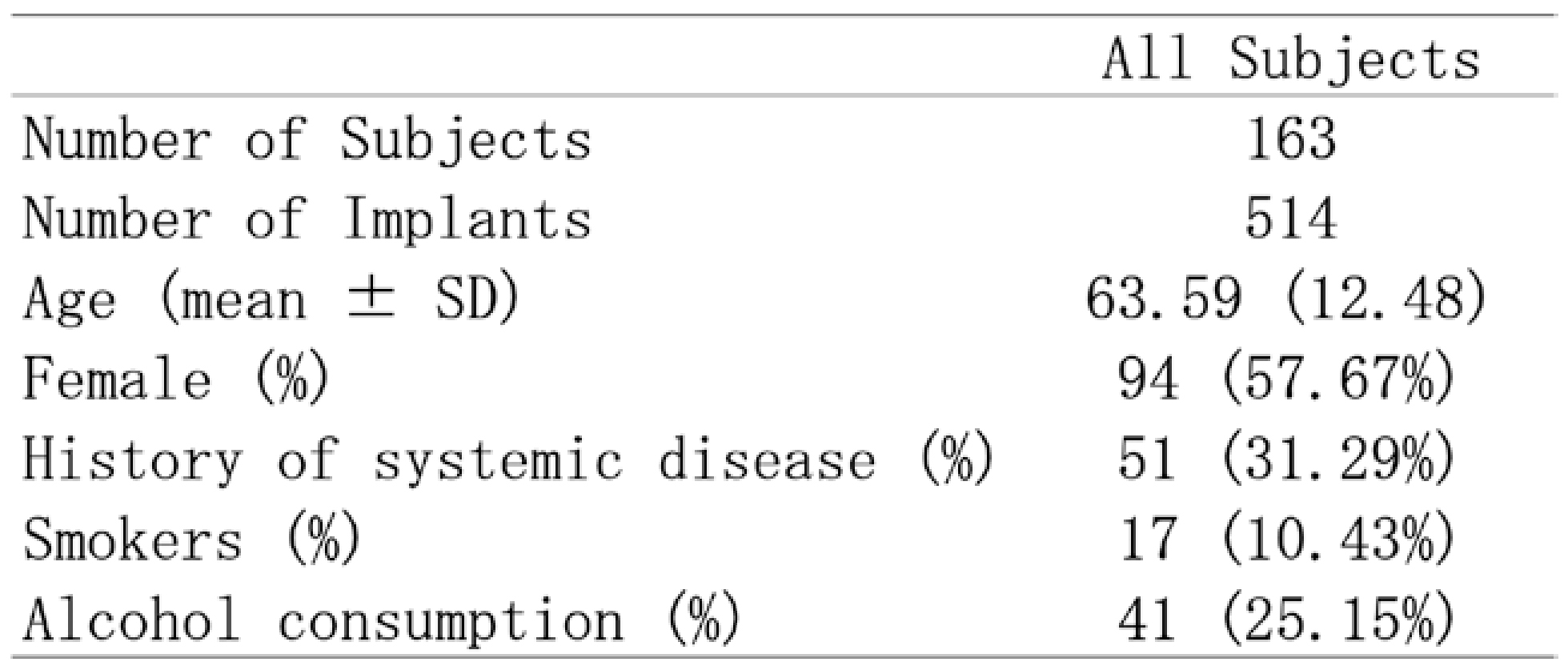
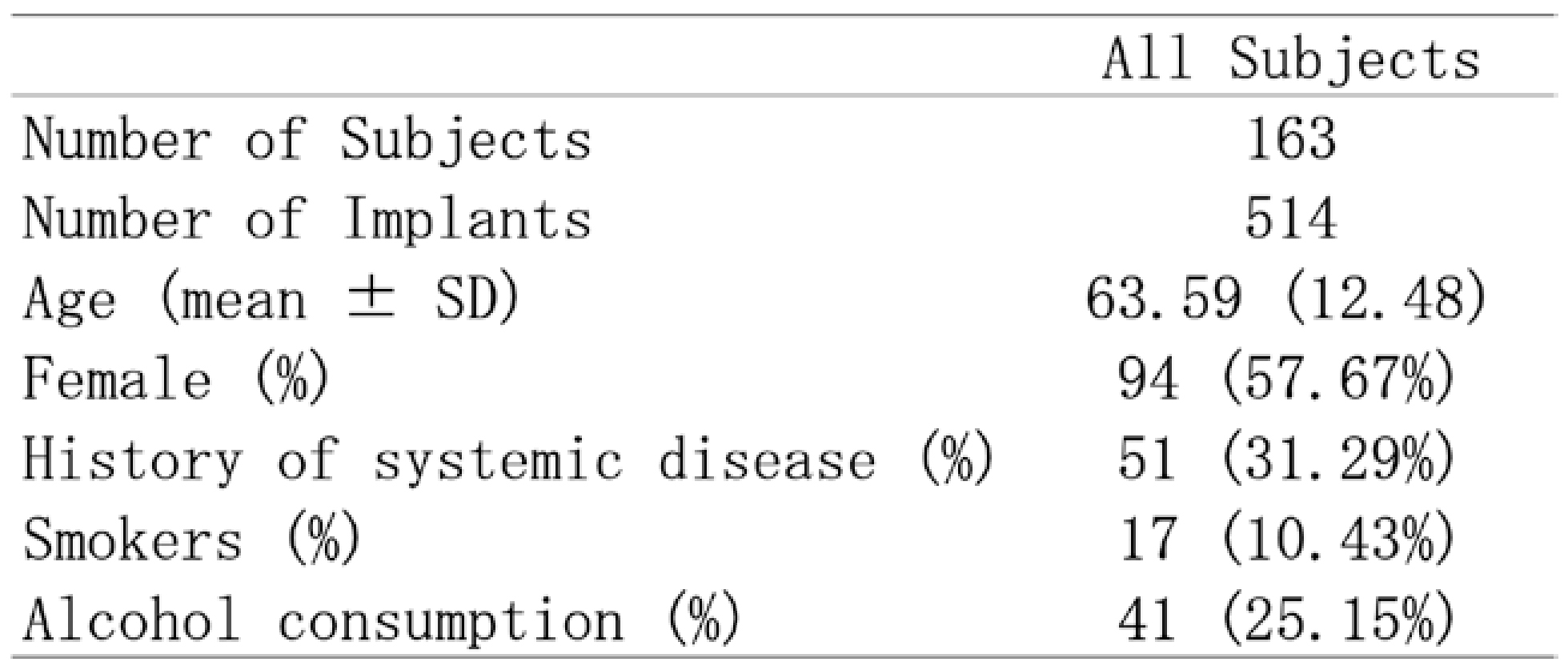
Table 1 presents the demographic and clinical characteristics of the 163 subjects (514 implants). The mean age was 63.59 ± 12.48 years, and 57.67% were female. Systemic disease history was reported in 31.29%, current smokers comprised 10.43%, and 25.15% had a habit of alcohol consumption.
The distribution of peri-implant conditions at the implant level is shown in Table 2. Approximately 80% of implants exhibited healthy peri-implant tissues. Using Criterion 1, the prevalence of peri-implant mucositis was 9.53%, and peri-implantitis was 11.89%. Using Criterion 2, the prevalence of peri-implant mucositis was 17.51%, and peri-implantitis was 3.11%. Thus, Criterion 1 yielded a higher rate of peri-implantitis, while Criterion 2 resulted in a higher rate of mucositis.
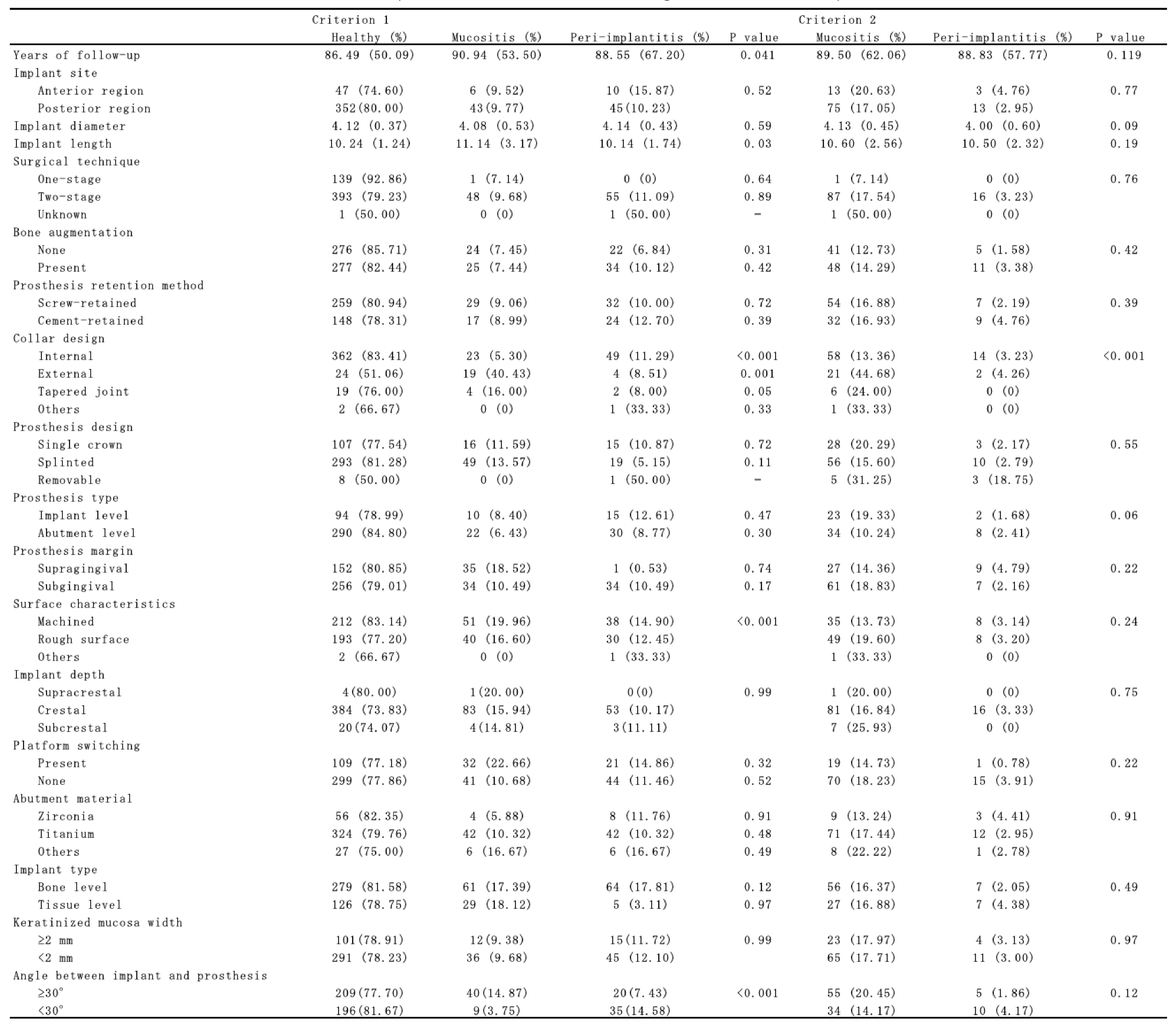
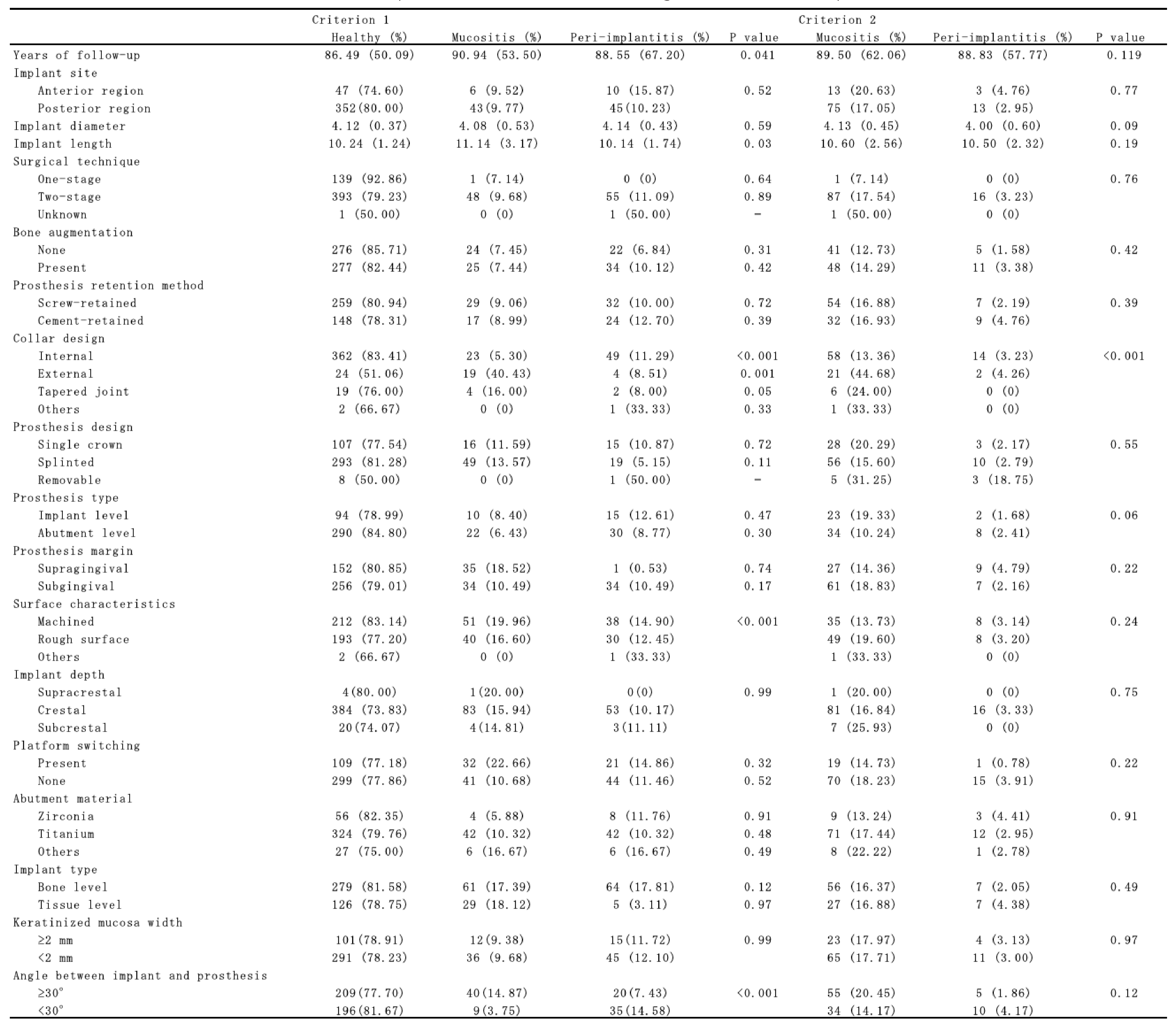
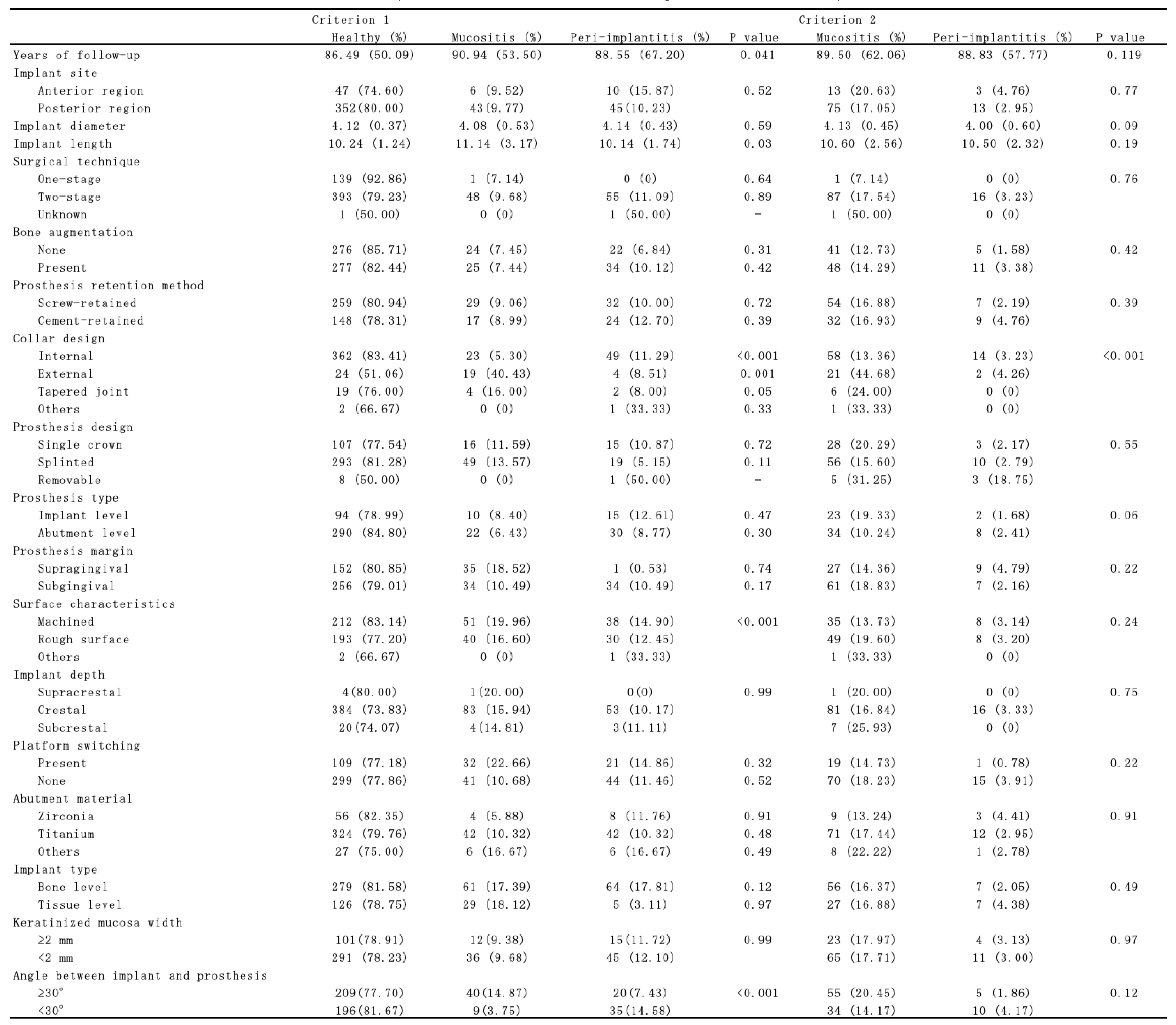
Table 3 shows implant-level health status according to various factors. Under Criterion 1, internal abutment connection exhibited peri-implant mucositis and peri-implantitis rate of 5,37% and 11,29%, respectively. Implant with machined collar surfaces exhibited peri-implant mucositis and peri-implantitis rates of 16.00% and 6.80%, respectively. Bone-level implants demonstrated peri-implant mucositis and peri-implantitis rates of 11.40% and 7.02%. In addition, implants with a prosthetic angulation ≥30° between the implant body and the prosthesis demonstrated peri-implant mucositis and peri-implantitis rates of 14.87% and 7.43%, respectively, with statistically significant differences observed.
Under Criterion 2, internal connection abutments were associated with significantly lower peri-implantitis (3.23%) and higher mucositis (13.36%).
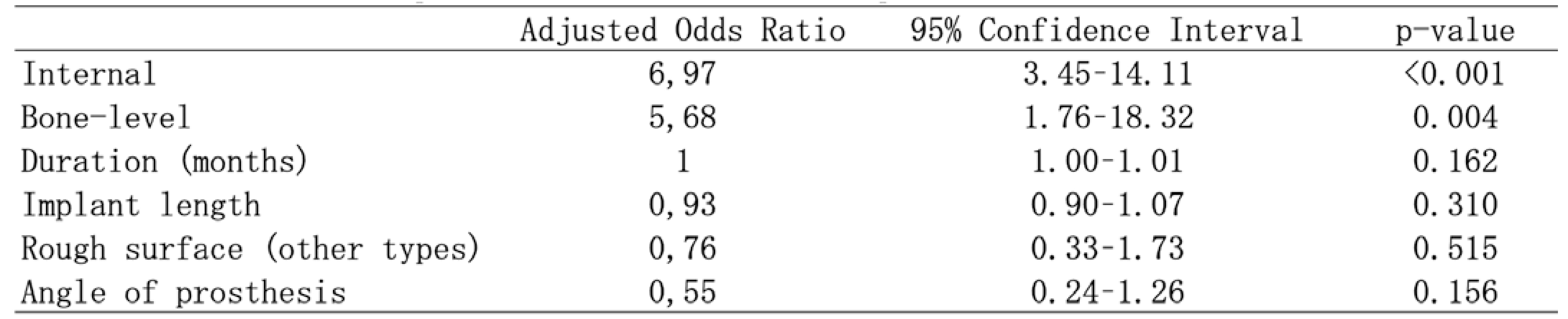
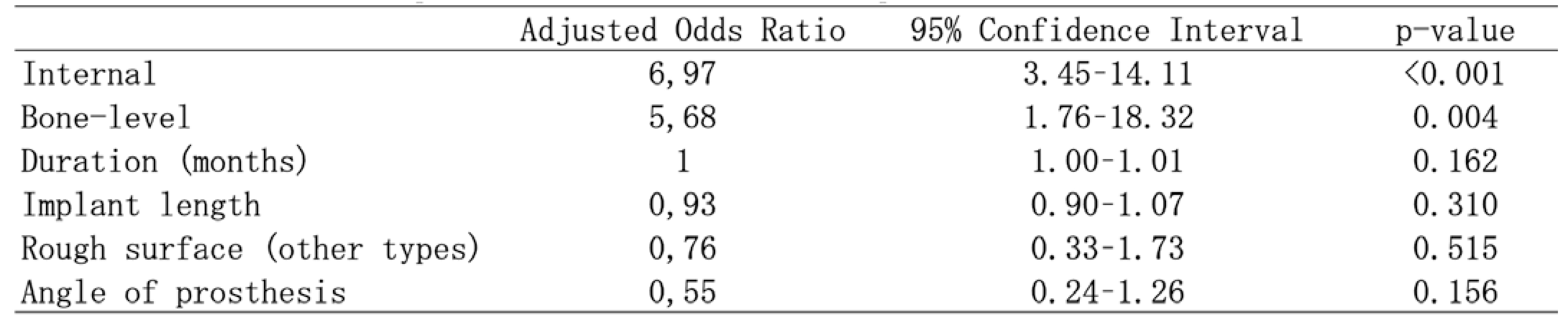
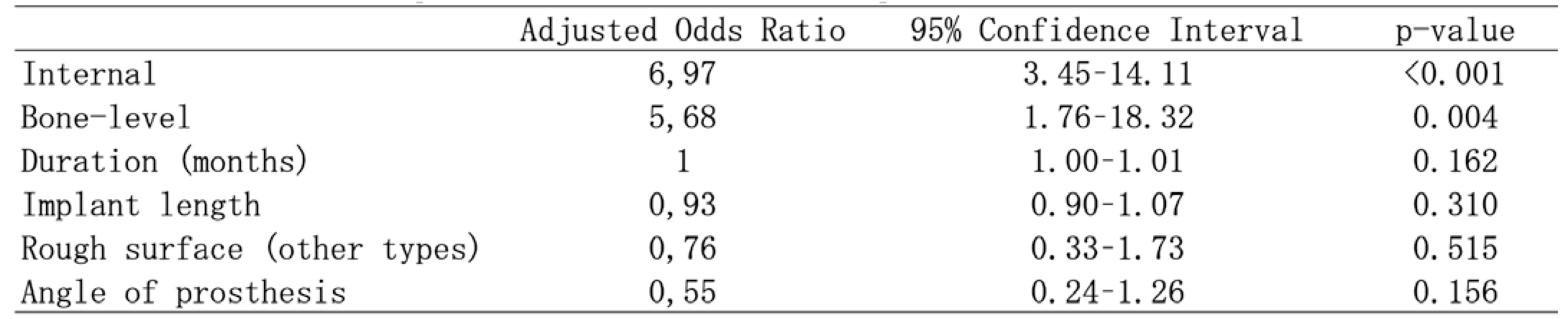
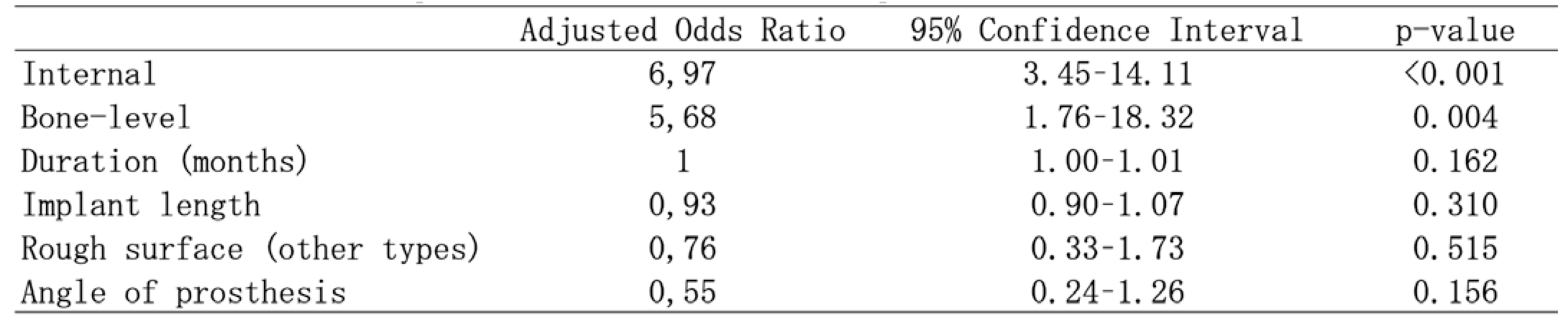
Multivariate logistic regression analysis was performed only for Criterion 1, due to the low prevalence of peri-implantitis under Criterion 2 (Table 4). Internal connection abutments (aOR = 6.97) and bone-level implants (aOR = 5.68) were significantly associated with increased risk of peri-implant mucositis and peri-implantitis. For peri-implantitis specifically (Criterion 1), implants with a rough surface topography at the coronal portion showed a significantly increased risk, with an adjusted odds ratio of 4.48 (Table 5).
(Table 1)Patients characteristics(Table 2)Total Number (Frequency %) of Implant Sites with Healthy Peri-implant Tissues, Peri-implant Mucositis, and Peri-implantitis(Table 3)Peri-implant tissue conditions according to factors at the implant level(Table 4)Results of moltivatiable logistic regression analysis for risk factors of Peri-implant mucositis and Peri-implantitis(Table 5)Results of multivariable logistic regression analysis for risk factors of peri-implantitis (Criterion 1)
IV. Discussion
In this study, the implant-level prevalence of peri-implant mucositis and peri-implantitis varied significantly depending on diagnostic criteria: 9.53% and 11.89% under Criterion 1, and 17.51% and 3.11% under Criterion 2, respectively. This discrepancy highlights the impact of case definition on epidemiological outcomes. Criterion 1 relies on longitudinal radiographic comparison from a baseline (1 year post-loading), enabling detection of progressive bone loss. In contrast, Criterion 2 uses a cross-sectional assessment of current bone defect depth without reference to baseline, making it unable to distinguish progressive from non-progressive lesions. Consequently, some cases with ongoing disease progression may have been missed under Criterion 2. This underscores the need for standardized diagnostic criteria and the establishment of normative values for clinical parameters such as PPD in peri-implant health.
Approximately 80% of implants were maintained in a healthy state, which is notably higher than the ~60% healthy implant rate reported in the meta-analysis by Lee et al.5 This favorable outcome may be attributed to the high frequency of maintenance visits (mean: 4.06 visits per year). Previous studies have shown that regular maintenance is associated with lower incidence of peri-implantitis,9 a finding supported by the present data.
This study identified several implant-related factors significantly associated with peri-implant disease: internal abutment connection design, bone-level implant type, and particularly, a rough surface topography at the implant collar. However, these features are commonly found in modern implant systems. Given their widespread use, it may be premature to label them as definitive risk factors without considering confounding variables such as prosthetic fit, emergence profile, and oral hygiene accessibility, which may vary by manufacturer or clinician.
Notably, implants with rough surfaces at the coronal portion demonstrated a significantly higher risk of peri-implantitis (aOR = 4.48), suggesting that surface topography plays a critical role in disease development. This finding aligns with previous evidence indicating that rough surfaces may retain more biofilm and are more difficult to decontaminate during maintenance. Careful consideration should be given to surface characteristics, especially in patients with a history of periodontitis or other risk profiles.
Additionally, implants with prosthetic angulation ≥30° showed increased prevalence of both mucositis and peri-implantitis, consistent with findings from the European Association for Osseointegration (EAO) consensus meetings.10 Such configurations may predispose to mechanical stress concentration and suboptimal plaque control, promoting inflammatory responses.
These results reinforce the importance of meticulous preoperative planning, including implant selection, prosthetic design, and surface characteristics—particularly for high-risk patients.
V. Conclusion
This implant-level analysis of peri-implant health and associated risk factors revealed the following key findings:
1. The prevalence of peri-implant mucositis and peri-implantitis varies substantially depending on diagnostic criteria, emphasizing the need for standardized definitions and normative clinical thresholds in clinical practice.
2. Implants with rough surface topography at the coronal portion are associated with a significantly higher risk of peri-implantitis, highlighting the importance of careful surface selection.
3. Prosthetic angulation and structural design features may influence peri-implant tissue health, underscoring the necessity of comprehensive prosthetic and surgical planning.
These findings suggest that peri-implant disease prevention strategies should extend beyond implant selection to include optimized prosthetic design and consistent maintenance protocols. Re-evaluation of current clinical approaches is warranted to enhance long-term implant outcomes.
References
Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis and peri-implant diseases and conditions — 2018 classification of periodontal and peri-implant diseases and conditions. J Periodontol. 2018;89(Suppl 1):S159–S172.
Cui Z, Wang P, Gao W. Microbial dysbiosis in periodontitis and peri-implantitis: pathogenesis, immune responses, and therapeutic. Front Cell Infect Microbiol. 2025 Feb 11;15:1517154. doi:10.3389/fcimb.2025.1517154. eCollection 2025.
Sekino S. Effectiveness of oral hygiene-focused maintenance in preventing peri-implantitis. J Jpn Soc Oral Implantol. 2022;35(1):Review article. (Originally in Japanese)
Kameda Y, Kobayashi T, Morokuma M, Kobayashi H, Ohhira A, Kubodera R, Sekino S. Prevalence and factors related to peri-implant diseases in general practitioners: Part I: Patient level analysis. JICD. 2023;4(2):e002.
Wada M, Mameno T, Onodera Y, Matsuda H, Daimon K, Ikebe K. Prevalence of peri-implant disease and risk indicators in a Japanese population with at least 3 years in function: A multicentre retrospective study. Clin Oral Implants Res. 2019 Feb;30(2):111–120. doi:10.1111/clr.13397. Epub 2019 Jan 18.
Mameno T, Wada M, Onodera Y, Fujita D, Sato H, Ikebe K. Longitudinal study on risk indicators for peri-implantitis using survival-time analysis. J Prosthodont Res. 2019 Apr;63(2):216–220. doi:10.1016/j.jpor.2018.12.002. Epub 2018 Dec 30.
Lee CT, Huang YW, Zhu L, Weltman R. Prevalences of peri-implantitis and peri-implant mucositis: systematic review and meta-analysis. J Dent. 2017 Jul;62:1–12. doi:10.1016/j.jdent.2017.04.011
Costa FO, Costa AM, Ferreira SD, et al. Long-term impact of patients' compliance to peri-implant maintenance therapy on the incidence of peri-implant diseases: An 11-year prospective follow-up clinical study. Clin Implant Dent Relat Res. 2023 Apr;25(2):303–312. doi:10.1111/cid.13169.
Schwarz F, Alcoforado G, Guerrero A, et al. Peri-implantitis: Summary and consensus statements of group 3. The 6th EAO Consensus Conference 2021. Clin Oral Implants Res. 2021 Oct;32 Suppl 21:245–253. doi:10.1111/clr.13827
1) Kameda Dental Clinic
2) The Academy of Clinical Dentistry
3) Department of Periodontology, School of Life Dentistry, Nippon Dental University
4) Department of Comprehensive Dentistry, Nippon Dental University Hospital
(表1)Patients characteristics(表2)Total Number (Frequency %) of Implant Sites with Healthy Peri-implant Tissues, Peri-implant Mucositis, and Peri-implantitis(表3)Peri-implant tissue conditions according to factors at the implant level(表4)Results of moltivatiable logistic regression analysis for risk factors of Peri-implant mucositis and Peri-implantitis(表5)Results of multivariable logistic regression analysis for risk factors of peri-implantitis (Criterion 1)
Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis and peri-implant diseases and conditions — 2018 classification of periodontal and peri-implant diseases and conditions. J Periodontol. 2018;89(Suppl 1):S159–S172.
Cui Z, Wang P, Gao W. Microbial dysbiosis in periodontitis and peri-implantitis: pathogenesis, immune responses, and therapeutic. Front Cell Infect Microbiol. 2025 Feb 11;15:1517154. doi:10.3389/fcimb.2025.1517154. eCollection 2025.
Sekino S. Effectiveness of oral hygiene-focused maintenance in preventing peri-implantitis. J Jpn Soc Oral Implantol. 2022;35(1):Review article. (Originally in Japanese)
Kameda Y, Kobayashi T, Morokuma M, Kobayashi H, Ohhira A, Kubodera R, Sekino S. Prevalence and factors related to peri-implant diseases in general practitioners: Part I: Patient level analysis. JICD. 2023;4(2):e002.
Wada M, Mameno T, Onodera Y, Matsuda H, Daimon K, Ikebe K. Prevalence of peri-implant disease and risk indicators in a Japanese population with at least 3 years in function: A multicentre retrospective study. Clin Oral Implants Res. 2019 Feb;30(2):111–120. doi:10.1111/clr.13397. Epub 2019 Jan 18.
Mameno T, Wada M, Onodera Y, Fujita D, Sato H, Ikebe K. Longitudinal study on risk indicators for peri-implantitis using survival-time analysis. J Prosthodont Res. 2019 Apr;63(2):216–220. doi:10.1016/j.jpor.2018.12.002. Epub 2018 Dec 30.
Lee CT, Huang YW, Zhu L, Weltman R. Prevalences of peri-implantitis and peri-implant mucositis: systematic review and meta-analysis. J Dent. 2017 Jul;62:1–12. doi:10.1016/j.jdent.2017.04.011
Costa FO, Costa AM, Ferreira SD, et al. Long-term impact of patients' compliance to peri-implant maintenance therapy on the incidence of peri-implant diseases: An 11-year prospective follow-up clinical study. Clin Implant Dent Relat Res. 2023 Apr;25(2):303–312. doi:10.1111/cid.13169.
Schwarz F, Alcoforado G, Guerrero A, et al. Peri-implantitis: Summary and consensus statements of group 3. The 6th EAO Consensus Conference 2021. Clin Oral Implants Res. 2021 Oct;32 Suppl 21:245–253. doi:10.1111/clr.13827
Prevalence and factors related to peri-implant diseases in general practitioners: Part II: Implant level analysisPrognosis of Angular Bony Defects After Active Periodontal Therapy: A 5-to17- Year Long-term Retrospective Cohort Study
1) Kameda Dental Clinic
2) The Academy of Clinical Dentistry
3) Department of Periodontology, School of Life Dentistry, Nippon Dental University
4) Department of Comprehensive Dentistry, Nippon Dental University Hospital
(表2)Total Number (Frequency %) of Implant Sites with Healthy Peri-implant Tissues, Peri-implant Mucositis, and Peri-implantitis(表3)Peri-implant tissue conditions according to factors at the implant level(表4)Results of moltivatiable logistic regression analysis for risk factors of Peri-implant mucositis and Peri-implantitis(表5)Results of multivariable logistic regression analysis for risk factors of peri-implantitis (Criterion 1)
Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis and peri-implant diseases and conditions — 2018 classification of periodontal and peri-implant diseases and conditions. J Periodontol. 2018;89(Suppl 1):S159–S172.
Cui Z, Wang P, Gao W. Microbial dysbiosis in periodontitis and peri-implantitis: pathogenesis, immune responses, and therapeutic. Front Cell Infect Microbiol. 2025 Feb 11;15:1517154. doi:10.3389/fcimb.2025.1517154. eCollection 2025.
Sekino S. Effectiveness of oral hygiene-focused maintenance in preventing peri-implantitis. J Jpn Soc Oral Implantol. 2022;35(1):Review article. (Originally in Japanese)
Kameda Y, Kobayashi T, Morokuma M, Kobayashi H, Ohhira A, Kubodera R, Sekino S. Prevalence and factors related to peri-implant diseases in general practitioners: Part I: Patient level analysis. JICD. 2023;4(2):e002.
Wada M, Mameno T, Onodera Y, Matsuda H, Daimon K, Ikebe K. Prevalence of peri-implant disease and risk indicators in a Japanese population with at least 3 years in function: A multicentre retrospective study. Clin Oral Implants Res. 2019 Feb;30(2):111–120. doi:10.1111/clr.13397. Epub 2019 Jan 18.
Mameno T, Wada M, Onodera Y, Fujita D, Sato H, Ikebe K. Longitudinal study on risk indicators for peri-implantitis using survival-time analysis. J Prosthodont Res. 2019 Apr;63(2):216–220. doi:10.1016/j.jpor.2018.12.002. Epub 2018 Dec 30.
Lee CT, Huang YW, Zhu L, Weltman R. Prevalences of peri-implantitis and peri-implant mucositis: systematic review and meta-analysis. J Dent. 2017 Jul;62:1–12. doi:10.1016/j.jdent.2017.04.011
Costa FO, Costa AM, Ferreira SD, et al. Long-term impact of patients' compliance to peri-implant maintenance therapy on the incidence of peri-implant diseases: An 11-year prospective follow-up clinical study. Clin Implant Dent Relat Res. 2023 Apr;25(2):303–312. doi:10.1111/cid.13169.
Schwarz F, Alcoforado G, Guerrero A, et al. Peri-implantitis: Summary and consensus statements of group 3. The 6th EAO Consensus Conference 2021. Clin Oral Implants Res. 2021 Oct;32 Suppl 21:245–253. doi:10.1111/clr.13827
1) Kameda Dental Clinic
2) The Academy of Clinical Dentistry
3) Department of Periodontology, School of Life Dentistry, Nippon Dental University
4) Department of Comprehensive Dentistry, Nippon Dental University Hospital
Resumen
Este estudio tuvo como objetivo investigar la prevalencia de las enfermedades periimplantarias y los factores de riesgo asociados en pacientes tratados en consultorios dentales generales en Japón. Se incluyeron un total de 514 implantes dentales en 163 pacientes (94 mujeres), con una edad media de 63,6 años, que asistieron a citas de mantenimiento en cinco clínicas dentales generales. Las características generales de los pacientes y los posibles factores de riesgo se registraron mediante historias clínicas y entrevistas durante las visitas de mantenimiento. Además, se realizaron exámenes clínicos periodontales y periimplantarios, así como evaluaciones radiográficas. La prevalencia de mucositis periimplantaria y periimplantitis se calculó a nivel de implante. Se realizó un análisis de regresión logística multivariado para evaluar la asociación entre las características generales de los pacientes, los indicadores de riesgo y la periimplantitis.
La prevalencia de mucositis periimplantaria osciló entre el 9,53% y el 17,51%, mientras que la de periimplantitis varió entre el 3,11% y el 11,89%, dependiendo de los criterios diagnósticos utilizados. El análisis de regresión logística multivariado reveló que una topografía de superficie rugosa en el cuerpo del implante se asoció significativamente con periimplantitis, con una razón de momios (odds ratio) de 4,85. En conclusión, entre los pacientes con implantes que reciben mantenimiento regular en consultorios dentales generales, la prevalencia de enfermedades periimplantarias a nivel de implante fue relativamente baja, y una superficie rugosa del implante mostró una correlación significativa con la periimplantitis.
Palabras clave: Periimplantitis, mucositis periimplantaria, implantes dentales, prevalencia, factores de riesgo, mantenimiento, superficie del implante, práctica dental general
I. Introducción
Las condiciones inflamatorias que afectan los tejidos que rodean los implantes dentales pueden clasificarse en dos categorías: mucositis periimplantaria y periimplantitis.1 La mucositis periimplantaria se caracteriza por una inflamación limitada a la mucosa periimplantaria sin evidencia radiográfica de pérdida ósea marginal, mientras que la periimplantitis implica una destrucción inflamatoria que se extiende al hueso de soporte, provocando una resorción progresiva del hueso alveolar. El factor etiológico principal de las enfermedades periimplantarias es la acumulación de biopelícula bacteriana.1 Con frecuencia se han detectado bacterias periodontales patógenas en sitios afectados por periimplantitis.2 Sin embargo, existen diferencias estructurales y biológicas entre la dentición natural y los tejidos periimplantarios. Mientras que la inflamación en los tejidos periodontales generalmente se limita al tejido conectivo, los procesos inflamatorios alrededor de los implantes pueden extenderse rápidamente a la interfaz hueso-implante.3 A diferencia de los tejidos periodontales, los tejidos periimplantarios carecen de ligamento periodontal y tienen una vascularización relativamente pobre, lo que puede comprometer los mecanismos de defensa del huésped. Como resultado, una vez que la infección microbiana provoca una alteración en la interfaz implante-hueso, incluso una resorción ósea de progresión lenta puede volverse autosostenida. Estas diferencias fundamentales hacen necesaria una terapia de mantenimiento de por vida tras la colocación del implante.4
A pesar del mantenimiento regular, las enfermedades periimplantarias pueden desarrollarse y representan una causa importante de fracaso del implante. Un metanálisis realizado por Lee et al.5 informó una prevalencia de periimplantitis a nivel de paciente del 19,83% y una prevalencia a nivel de implante del 9,25%. Sin embargo, la mayoría de los datos incluidos en estos análisis provienen de centros especializados, reflejando resultados bajo condiciones óptimas de tratamiento. Por lo tanto, para obtener hallazgos más generalizables, son esenciales estudios epidemiológicos realizados en entornos de práctica general rutinaria. En nuestro primer informe, demostramos que, entre pacientes mantenidos en la práctica clínica general, la prevalencia a nivel de paciente de mucositis periimplantaria fue del 23,9% y la de periimplantitis del 15,8%, identificando la historia de pérdida dental por periodontitis y el tabaquismo como factores de riesgo significativos.6
El presente estudio tiene como objetivo analizar la prevalencia de enfermedades periimplantarias a nivel de implante e identificar los factores de riesgo asociados en un entorno de práctica dental general.
II. Sujetos y Métodos
Este estudio fue aprobado por el Comité de Ética de la Academia de Odontología Clínica (Número de aprobación: 22-003). Se obtuvo el consentimiento informado por escrito de todos los participantes. El diseño del estudio combinó una revisión retrospectiva de los registros de los pacientes con una evaluación transversal basada en el examen clínico, la evaluación radiográfica y los datos recopilados mediante entrevistas durante las visitas de mantenimiento.
Se incluyeron un total de 514 implantes dentales en 163 pacientes (edad media: 63,6 años, 94 mujeres) que asistieron a cinco clínicas dentales generales en Japón para mantenimiento entre julio de 2021 y julio de 2022. Todos los implantes habían estado funcionales durante al menos un año antes del examen. Se excluyeron los pacientes que hubieran tomado antibióticos sistémicos en los tres meses previos al examen.
Examen clínico
En el momento de la visita de mantenimiento, se registraron los siguientes parámetros para cada implante:
Profundidad de sondaje (PPD)
Sangrado al sondaje (BOP) o supuración (S)
Índice de placa
Nivel radiográfico del hueso marginal (MBL)
Las mediciones clínicas se realizaron con una sonda periodontal de plástico. La PPD y el BOP se evaluaron en seis sitios por implante: mesiobucal, mediobucal, distobucal, distolingual, mediolingual y mesiolingual, registrándose las lecturas en milímetros. Los puntajes de placa se registraron tras la aplicación de un agente revelador en cuatro aspectos: mesial, bucal, distal y lingual.
Las imágenes radiográficas se obtuvieron mediante un equipo de rayos X dental con técnica paralela de cono largo o una radiografía panorámica. El volumen óseo se calculó midiendo la distancia desde el nivel del hueso marginal hasta el ápice del implante (a) y la longitud del implante (b). La relación (b/a) se utilizó para estimar el volumen óseo relativo. El volumen óseo basal se definió como la medición radiográfica tomada un año después de la carga protésica. La diferencia entre el volumen óseo basal y el actual se definió como pérdida ósea marginal,7,8 (Figura 1: Criterio 1). Alternativamente, como Criterio 2, se midió la distancia vertical desde la cresta ósea marginal hasta la base del defecto intrabonoso como la profundidad del defecto óseo (Figura 2: longitud de la flecha blanca).
Para los dientes naturales, se obtuvieron registros completos de PPD, BOP, supuración, índice de control de placa (PCR) y clasificación de Eichner.
(Fig.1) Criterio 1(Fig.2) Criterio 2.The white arrow indicates the amount of bone loss, defined as the distance from the bone crest to the base of the bone defect.
Criterios diagnósticos
Los diagnósticos se realizaron utilizando definiciones modificadas basadas en el informe de consenso de 2018 sobre enfermedades periimplantarias:4
Mucositis periimplantaria
Presencia de BOP o supuración, con menos de 1 mm de pérdida ósea marginal.
Periimplantitis
Se aplicaron dos criterios diagnósticos:
Criterio 1: Presencia de BOP o supuración, con ≥1 mm de pérdida ósea marginal en comparación con el valor basal (1 año tras la carga).
Criterio 2: Presencia de BOP o supuración, con PPD ≥6 mm y profundidad del defecto óseo ≥3 mm observados en radiografías actuales.
Análisis estadístico
Se calcularon estadísticas descriptivas para todas las variables, incluyendo media ± desviación estándar para variables continuas y frecuencias para variables categóricas, a nivel de implante. Los datos se estratificaron según el tiempo transcurrido desde la carga protésica (<5 años, 5–10 años, >10 años), y se realizaron comparaciones entre grupos mediante ANOVA de un factor para variables continuas y pruebas de chi-cuadrado para datos categóricos.
La prevalencia de tejidos periimplantarios sanos, mucositis periimplantaria y periimplantitis se calculó según cada criterio diagnóstico. Las características generales de los pacientes y los parámetros clínicos de la dentición natural se compararon entre los grupos diagnósticos mediante ANOVA de un factor o pruebas de chi-cuadrado, según correspondiera.
Para evaluar la asociación entre factores de riesgo potenciales y periimplantitis, se utilizaron modelos de regresión logística multivariada. Las variables resultado se categorizaron como: implante sano, mucositis periimplantaria o periimplantitis. Se construyeron dos modelos: uno con "enfermedad periimplantaria" (mucositis + periimplantitis) como resultado, y otro con "periimplantitis" como resultado principal, utilizando implantes sanos (y en algunos modelos, sanos + mucositis) como referencia. Las variables independientes incluyeron datos demográficos, factores sistémicos y parámetros clínicos que mostraron las asociaciones bivariadas más fuertes con la enfermedad. Se calcularon razones de momios ajustadas (aOR) e intervalos de confianza del 95% (IC 95%) para determinar la significancia estadística.
III. Resultados
La Tabla 1 presenta las características demográficas y clínicas de los 163 sujetos (514 implantes). La edad media fue de 63,59 ± 12,48 años, y el 57,67% eran mujeres. Se reportó antecedente de enfermedad sistémica en el 31,29%, el 10,43% eran fumadores activos y el 25,15% consumía alcohol habitualmente.
La distribución de las condiciones periimplantarias a nivel de implante se muestra en la Tabla 2. Aproximadamente el 80% de los implantes presentaron tejidos periimplantarios sanos. Según el Criterio 1, la prevalencia de mucositis periimplantaria fue del 9,53% y la de periimplantitis del 11,89%. Según el Criterio 2, la prevalencia de mucositis fue del 17,51% y la de periimplantitis del 3,11%. Por tanto, el Criterio 1 arrojó una tasa más alta de periimplantitis, mientras que el Criterio 2 resultó en una tasa más alta de mucositis.
La Tabla 3 muestra el estado de salud a nivel de implante según diversos factores. Según el Criterio 1, los implantes con conexión interna del pilar mostraron tasas de mucositis y periimplantitis del 5,37% y 11,29%, respectivamente. Los implantes con superficie de colar mecanizado presentaron tasas del 16,00% y 6,80%, respectivamente. Los implantes de nivel óseo mostraron tasas del 11,40% y 7,02%. Además, los implantes con una angulación protésica ≥30° entre el cuerpo del implante y la prótesis mostraron tasas de mucositis y periimplantitis del 14,87% y 7,43%, respectivamente, con diferencias estadísticamente significativas.
Según el Criterio 2, las conexiones internas del pilar se asociaron con una periimplantitis significativamente menor (3,23%) y una mucositis mayor (13,36%).
El análisis de regresión logística multivariado se realizó únicamente para el Criterio 1, debido a la baja prevalencia de periimplantitis bajo el Criterio 2 (Tabla 4). Las conexiones internas del pilar (aOR = 6,97) y los implantes de nivel óseo (aOR = 5,68) se asociaron significativamente con un mayor riesgo de mucositis y periimplantitis. Específicamente para la periimplantitis (Criterio 1), los implantes con una topografía de superficie rugosa en la porción coronal mostraron un riesgo significativamente mayor, con una razón de momios ajustada de 4,48 (Tabla 5).
(Tabla 1)Patients characteristics(Tabla 2)Total Number (Frequency %) of Implant Sites with Healthy Peri-implant Tissues, Peri-implant Mucositis, and Peri-implantitis(Tabla 3)Peri-implant tissue conditions according to factors at the implant level(Tabla 4)Results of moltivatiable logistic regression analysis for risk factors of Peri-implant mucositis and Peri-implantitis(Tabla 5)Results of multivariable logistic regression analysis for risk factors of peri-implantitis (Criterion 1)
IV. Discusión
En este estudio, la prevalencia a nivel de implante de mucositis y periimplantitis varió significativamente según los criterios diagnósticos: 9,53% y 11,89% bajo el Criterio 1, y 17,51% y 3,11% bajo el Criterio 2, respectivamente. Esta discrepancia resalta el impacto de la definición de caso en los resultados epidemiológicos. El Criterio 1 se basa en una comparación radiográfica longitudinal desde un valor basal (1 año tras la carga), permitiendo detectar pérdida ósea progresiva. En contraste, el Criterio 2 utiliza una evaluación transversal de la profundidad actual del defecto óseo sin referencia al valor basal, por lo que no puede distinguir entre lesiones progresivas y no progresivas. En consecuencia, algunos casos con progresión activa de la enfermedad podrían haberse pasado por alto bajo el Criterio 2. Esto subraya la necesidad de criterios diagnósticos estandarizados y del establecimiento de valores normativos para parámetros clínicos como la PPD en la salud periimplantaria.
Aproximadamente el 80% de los implantes se mantuvieron en estado saludable, lo cual es notablemente superior al ~60% de implantes sanos reportado en el metanálisis de Lee et al.5 Este resultado favorable podría atribuirse a la alta frecuencia de visitas de mantenimiento (media: 4,06 visitas por año). Estudios previos han demostrado que el mantenimiento regular se asocia con una menor incidencia de periimplantitis,9 hallazgo respaldado por los datos actuales.
Este estudio identificó varios factores relacionados con el implante significativamente asociados con enfermedad periimplantaria: diseño de conexión interna del pilar, tipo de implante de nivel óseo y, especialmente, una topografía de superficie rugosa en el cuello del implante. Sin embargo, estas características son comunes en los sistemas modernos de implantes. Dado su uso extendido, podría ser prematuro considerarlos factores de riesgo definitivos sin considerar variables de confusión como el ajuste protésico, el perfil de emergencia y la accesibilidad para la higiene bucal, que pueden variar según el fabricante o el clínico.
Destacablemente, los implantes con superficie rugosa en la porción coronal mostraron un riesgo significativamente mayor de periimplantitis (aOR = 4,48), lo que sugiere que la topografía de la superficie desempeña un papel crítico en el desarrollo de la enfermedad. Este hallazgo concuerda con evidencia previa que indica que las superficies rugosas retienen más biopelícula y son más difíciles de descontaminar durante el mantenimiento. Debe prestarse especial atención a las características de la superficie, especialmente en pacientes con antecedente de periodontitis u otros perfiles de riesgo.
Además, los implantes con angulación protésica ≥30° mostraron una mayor prevalencia de mucositis y periimplantitis, lo cual es consistente con hallazgos de las reuniones de consenso de la Asociación Europea de Oseointegración (EAO).10 Estas configuraciones pueden predisponer al estrés mecánico concentrado y a un control subóptimo de la placa, promoviendo respuestas inflamatorias.
Estos resultados refuerzan la importancia de una planificación preoperatoria minuciosa, que incluya la selección del implante, el diseño protésico y las características de la superficie, especialmente en pacientes de alto riesgo.
V. Conclusión
Este análisis a nivel de implante sobre la salud periimplantaria y los factores de riesgo asociados reveló los siguientes hallazgos clave:
La prevalencia de mucositis periimplantaria y periimplantitis varía considerablemente según los criterios diagnósticos, lo que enfatiza la necesidad de definiciones estandarizadas y umbrales clínicos normativos en la práctica clínica.
Los implantes con superficie rugosa en la porción coronal están asociados con un riesgo significativamente mayor de periimplantitis, destacando la importancia de una selección cuidadosa de la superficie.
La angulación protésica y las características de diseño estructural pueden influir en la salud de los tejidos periimplantarios, subrayando la necesidad de una planificación quirúrgica y protésica integral.
Estos hallazgos sugieren que las estrategias de prevención de enfermedades periimplantarias deben extenderse más allá de la selección del implante para incluir un diseño protésico optimizado y protocolos de mantenimiento consistentes. Es necesario reevaluar los enfoques clínicos actuales para mejorar los resultados a largo plazo de los implantes.
References
Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis and peri-implant diseases and conditions — 2018 classification of periodontal and peri-implant diseases and conditions. J Periodontol. 2018;89(Suppl 1):S159–S172.
Cui Z, Wang P, Gao W. Microbial dysbiosis in periodontitis and peri-implantitis: pathogenesis, immune responses, and therapeutic. Front Cell Infect Microbiol. 2025 Feb 11;15:1517154. doi:10.3389/fcimb.2025.1517154. eCollection 2025.
Sekino S. Effectiveness of oral hygiene-focused maintenance in preventing peri-implantitis. J Jpn Soc Oral Implantol. 2022;35(1):Review article. (Originally in Japanese)
Kameda Y, Kobayashi T, Morokuma M, Kobayashi H, Ohhira A, Kubodera R, Sekino S. Prevalence and factors related to peri-implant diseases in general practitioners: Part I: Patient level analysis. JICD. 2023;4(2):e002.
Wada M, Mameno T, Onodera Y, Matsuda H, Daimon K, Ikebe K. Prevalence of peri-implant disease and risk indicators in a Japanese population with at least 3 years in function: A multicentre retrospective study. Clin Oral Implants Res. 2019 Feb;30(2):111–120. doi:10.1111/clr.13397. Epub 2019 Jan 18.
Mameno T, Wada M, Onodera Y, Fujita D, Sato H, Ikebe K. Longitudinal study on risk indicators for peri-implantitis using survival-time analysis. J Prosthodont Res. 2019 Apr;63(2):216–220. doi:10.1016/j.jpor.2018.12.002. Epub 2018 Dec 30.
Lee CT, Huang YW, Zhu L, Weltman R. Prevalences of peri-implantitis and peri-implant mucositis: systematic review and meta-analysis. J Dent. 2017 Jul;62:1–12. doi:10.1016/j.jdent.2017.04.011
Costa FO, Costa AM, Ferreira SD, et al. Long-term impact of patients' compliance to peri-implant maintenance therapy on the incidence of peri-implant diseases: An 11-year prospective follow-up clinical study. Clin Implant Dent Relat Res. 2023 Apr;25(2):303–312. doi:10.1111/cid.13169.
Schwarz F, Alcoforado G, Guerrero A, et al. Peri-implantitis: Summary and consensus statements of group 3. The 6th EAO Consensus Conference 2021. Clin Oral Implants Res. 2021 Oct;32 Suppl 21:245–253. doi:10.1111/clr.13827