1) Section of Oral Implantology, Department of Oral Rehabilitation, Fukuoka Dental College
2) Educational Support and Institutional Research Office, Fukuoka Dental College
Direct correspondence and requests for reprints to Dr. Kae Kakura, Section of Oral Implantology, Department of Oral Rehabilitation. Fukuoka Dental College, 2-15-1 Tamura, Sawara-ku, Fukuoka, 814-0193, Japan; 81-92-801-0425 phone; +81-92-801-0513 fax; [email protected].
Abstract
Objectives: The integration of implantology into dental education is essential to prepare predoctoral students for modern clinical practice. This study aimed to evaluate the impact of a hands-on implant training program on students’ perceptions of implant treatment and to compare the results with a similar survey conducted 15 years ago. Methods: Dental students participated in a comprehensive hands-on implant training session during their fifth-year clinical rotation. The training involved techniques such as gingival incision, flap reflection, implant placement, suturing, and impression-taking, using both conventional and digital methods. Students' perceptions of implant treatment were assessed through a pre- and post-training questionnaire, focusing on topics such as the necessity of implant education and its potential difficulty. Results: In 2024, 84 students participated in the hands-on training and completed the questionnaire. The results revealed a significant increase in the number of students who preferred implants over other treatment options for restoring a missing mandibular first molar. Although no significant differences were observed in students’ views on the difficulty of implant treatment, a positive shift in attitudes toward incorporating implant treatment into future practice was noted. Conclusions: The findings suggest that advancements in implant training, particularly the inclusion of digital technologies, have contributed to more comprehensive and effective education. This study also demonstrates that hands-on training plays a key role in motivating students to adopt implantology in their clinical practice. The results underline the importance of incorporating cutting-edge technology and comprehensive training in implant education to foster confidence and competence in future practitioners.
Since the early 1990s, the necessity of incorporating implantology into dental education has been recognized and the methods for doing so have been widely reported.1–7 A report from approximately 20 years ago noted that while many dental universities had included implantology in their curricula, there was significant variation in the use of lectures, model-based training, and the extent of clinical experience provided.8–15 In a 2005 survey of implant education at 56 European dental universities, Afsharzand et al. reported that although an implant course was required as part of predoctoral training at most universities, the content of predoctoral implantology education programs varied widely between institutions.13 Additionally, Maalhagh-Fard et al. conducted a survey of graduates after initiating a predoctoral elective program on implantology at the University of Detroit Mercy School of Dentistry. They reported a strong positive correlation between participation in the program and the introduction of implant treatment in postgraduate clinical practice.16
When implant treatment first began to gain popularity, dentists often learned implant-related knowledge and techniques through vendor-led workshops and lectures, with limited opportunities to acquire foundational knowledge. A systematic curriculum that develops foundational knowledge of implantology from the predoctoral to postgraduate levels is essential to prepare students to comprehensively understand implant treatment. Accordingly, Fukuoka Dental College began offering implantology training to predoctoral students, using models, in 2003. The initial training involved placing a single type of implant body into a simple polyurethane model. Starting in 2004, the curriculum was enhanced to include several types of distinctive implant bodies and a hands-on training model that was developed in-house. All predoctoral students are required to undergo this training. Additionally, students attend 13 lectures on the fundamental principles of implant treatment and participate in two treatment planning exercises using implant simulations alongside the hands-on training. To evaluate the educational impact of implantology at that time, we reported a comparison of students' perceptions before and after the hands-on training in 2009.17
Fifteen years have passed since that report, and implant treatment is now recognized as a high-priority treatment option for the prosthetic rehabilitation of missing teeth.18 Furthermore, implantology education is now offered at most dental universities in Japan. Amid these changing circumstances, the content of implantology education at our university has also evolved. Therefore, we conducted a similar survey to the one conducted 15 years ago to examine changes in students' perceptions of implant treatment before and after the hands-on training.
2. Methods
2.1 Ethics approval
This study was conducted with the approval of the Ethics Review Committee of Fukuoka Dental College (approval number 612).
2.2 Implantology education and hands-on training
A hands-on implant placement training session was conducted during the clinical training period for fifth-year students in the Fukuoka Dental College Hospital. The clinical training for undergraduate students comprised 60 days in the first term and 87 days in the second term. During this period, students rotated through the Departments of Implants and Prosthodontics, Conservative Dentistry and Periodontics, Oral Surgery, Pediatric and Orthodontic Dentistry, General Dentistry, Dentistry for Patients with Disabilities, Home Dental Care, and Medical, gaining practical experience by participating in clinical activities.
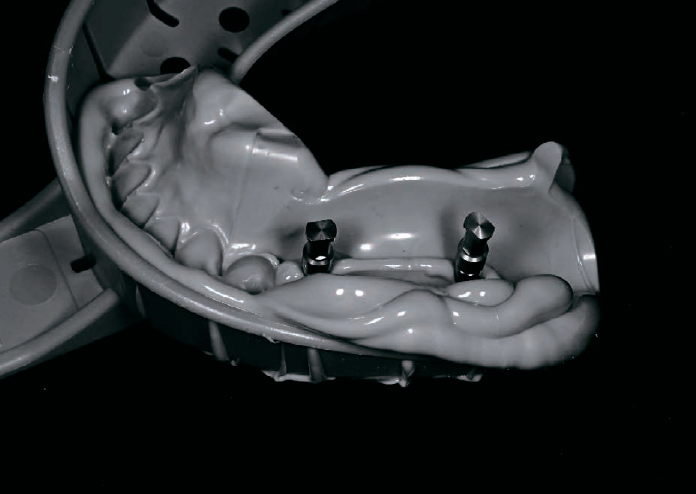
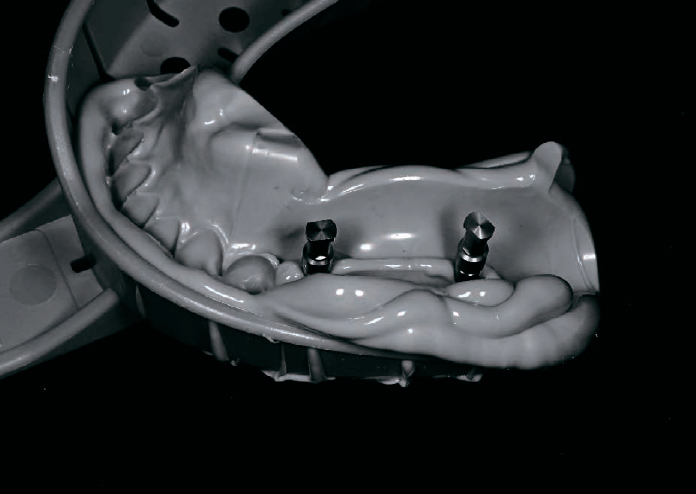
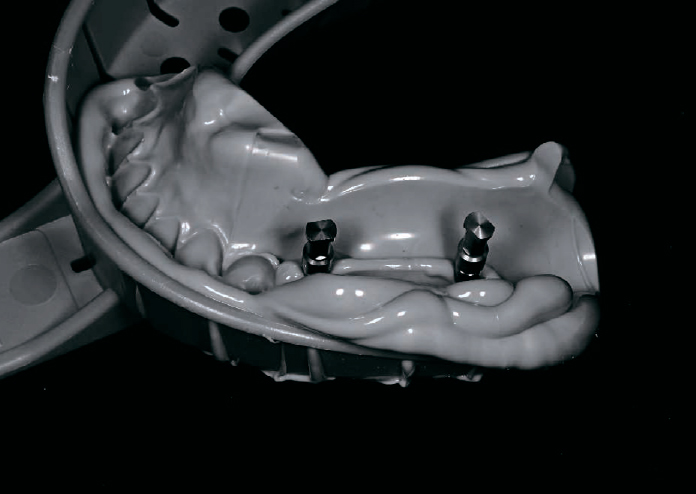
The clinical training in implantology was conducted over a period of one day as part of the restorative dentistry training, which comprised 15 days in the first term and 16 days in the second term. This training included chairside observation and assisting the instructor. Approximately 10 students participated in each hands-on training session, with one instructor assigned to guide two to three students. Using dedicated models, students practiced a series of procedures, including gingival incision, reflection of the gingival flap, preparation of the implant site, implant placement, suturing, and secondary surgery (Figs.1,2). Additionally, they practiced impression-taking techniques using both open-tray silicone impressions and optical impressions with an intraoral scanner (Figs.3,4). Through this hands-on training, students acquired the knowledge and skills necessary to explain the need for prosthetic treatments to restore missing teeth and to present treatment options to patients. All students completed these processes within the one-day training period.
2.3 Implantology models
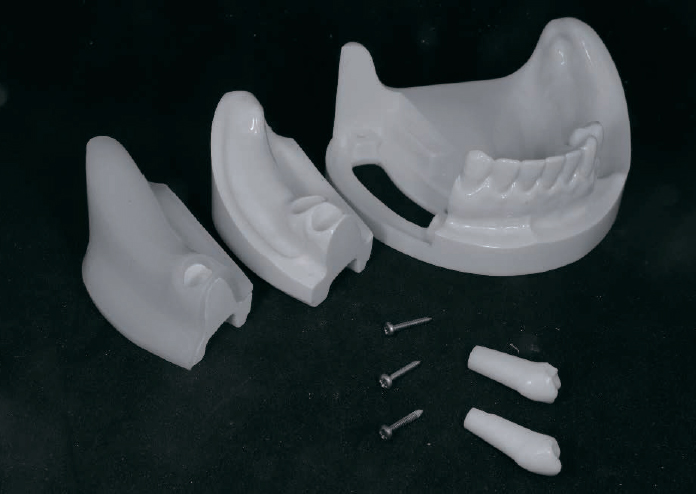
A simulation model specifically developed for this hands-on training (Nisshin Dental Products Co., Ltd., Kyoto, Japan) was employed (Fig.1). The alveolar bone region for implant training consisted of three layers: silicone rubber gingiva, cortical bone, and cancellous bone. The edentulous region could be replaced with acrylic resin, allowing it to be used for training in fabricating removable partial dentures. Thus, students could use the same model for both implant and removable denture training.
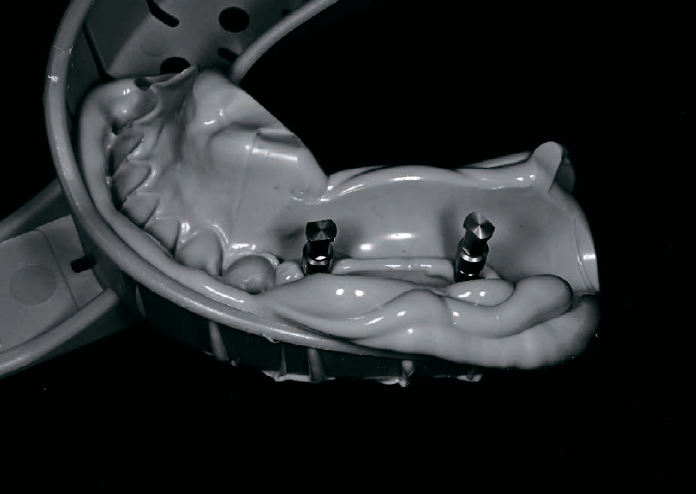
For implant training, tapered implants (Replace Select Tapered, Nobel Biocare Japan, Tokyo, Japan) and straight implants (Replace Select Straight, Nobel Biocare Japan, Tokyo, Japan) were employed (Fig.2). Students learned techniques such as gingival incision, flap reflection, determination of implant placement sites, preparation of implant sockets, placement of implants, and suturing (Fig.3). Furthermore, they were trained in implant platform exposure, abutment connection, and impression-taking methods (Fig.4a,b).
(Fig.1) A simulation model for predoctoral implant training(Fig.2) Two types of implants for predoctoral training(Fig.3) Implant placement procedure on simulation model(Fig.4a) Implant analogs connection procedure with silicone
impression(Fig.4b) Optical impression procedure using an intraoral scanner
2.4 Questionnaire
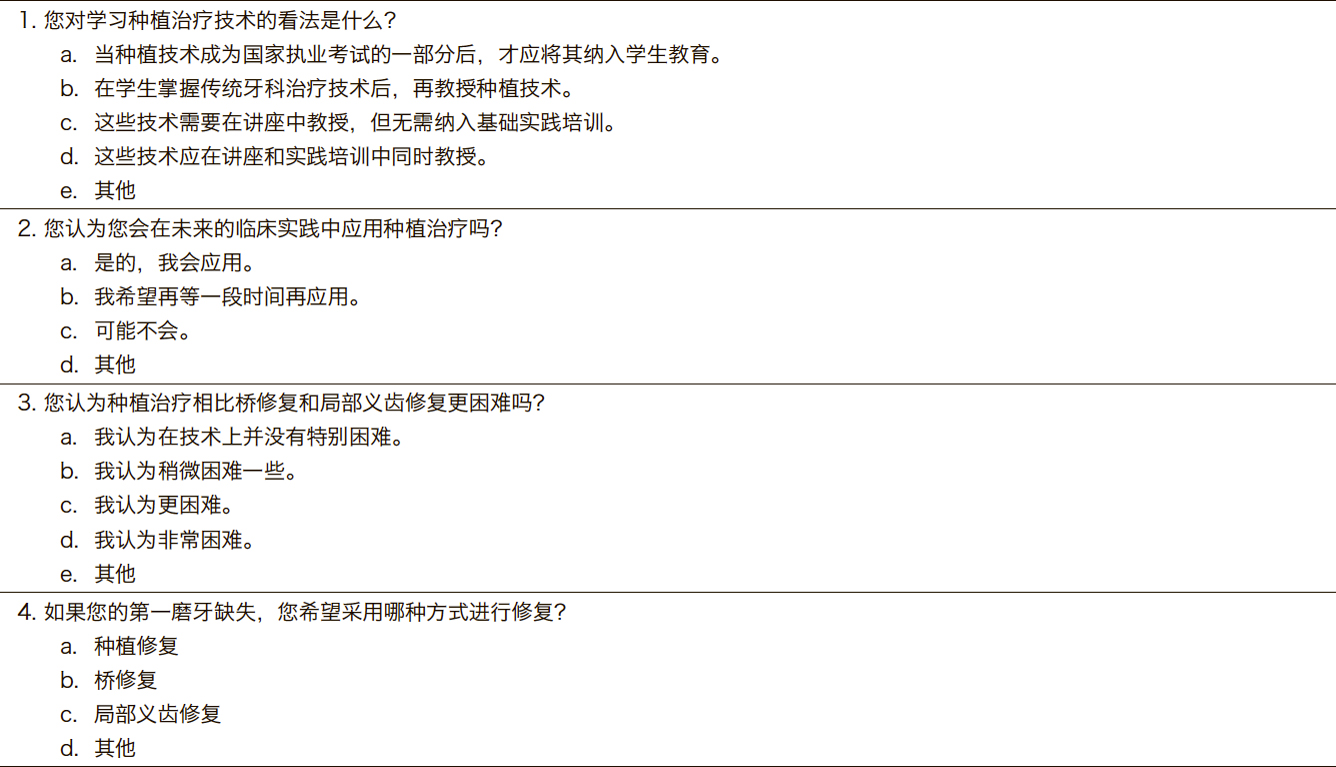
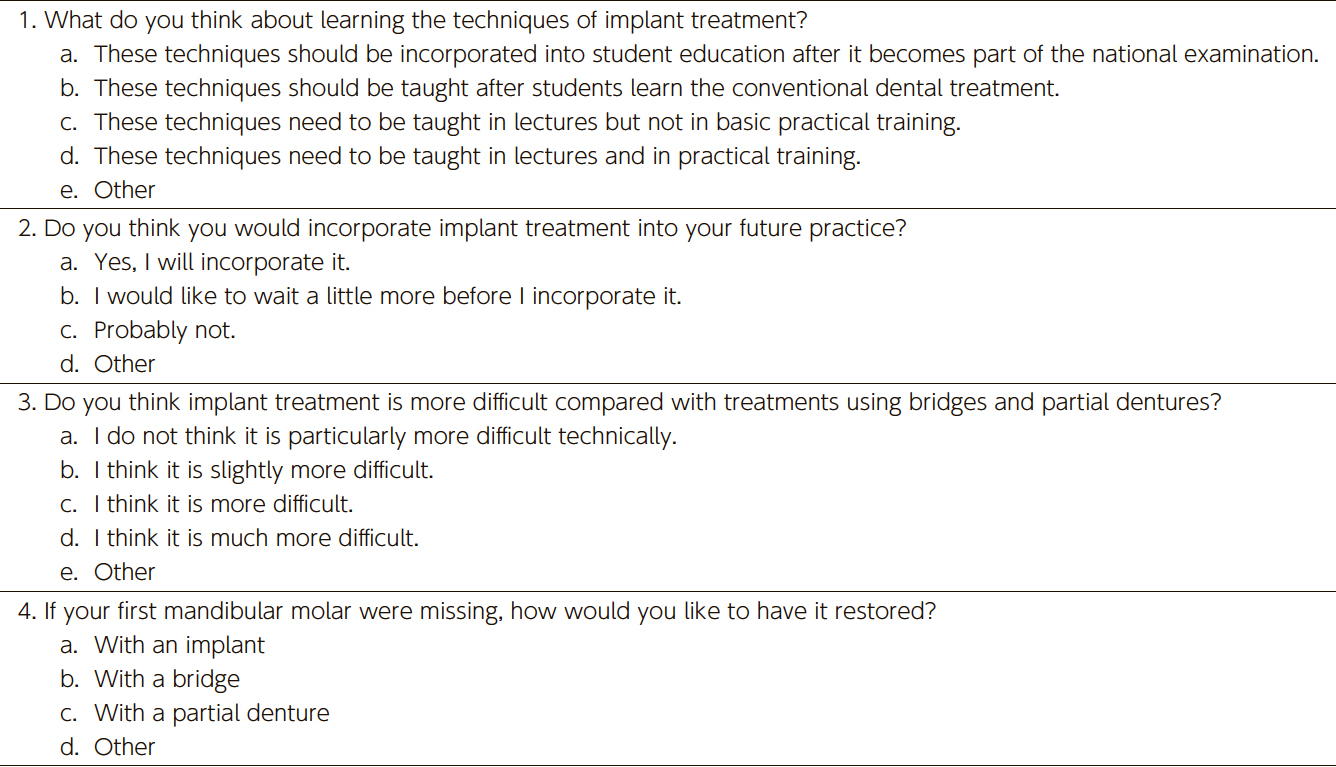
To assess students' perceptions of implant treatment, a questionnaire was administered to all students who participated in the implant training (Table 1). The questionnaire was administered immediately before and after the training. Students were asked whether they agreed or disagreed with topics such as the necessity of implant-related training and lectures and the necessity of implant treatment. Their responses were compared before and after training. Statistical analyses were performed using IBM® SPSS® Statistics Version 22 (IBM, Armonk, USA).
3. Results
In 2024, 84 students (47 males, 37 females) participated in hands-on implant training. The response rate to the questionnaire was 100%.
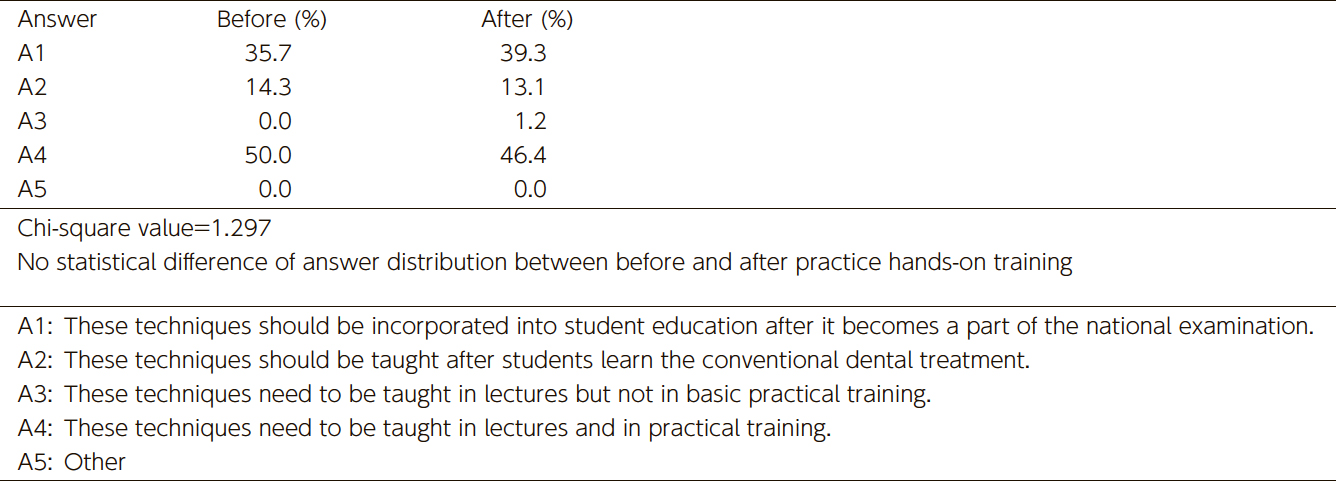
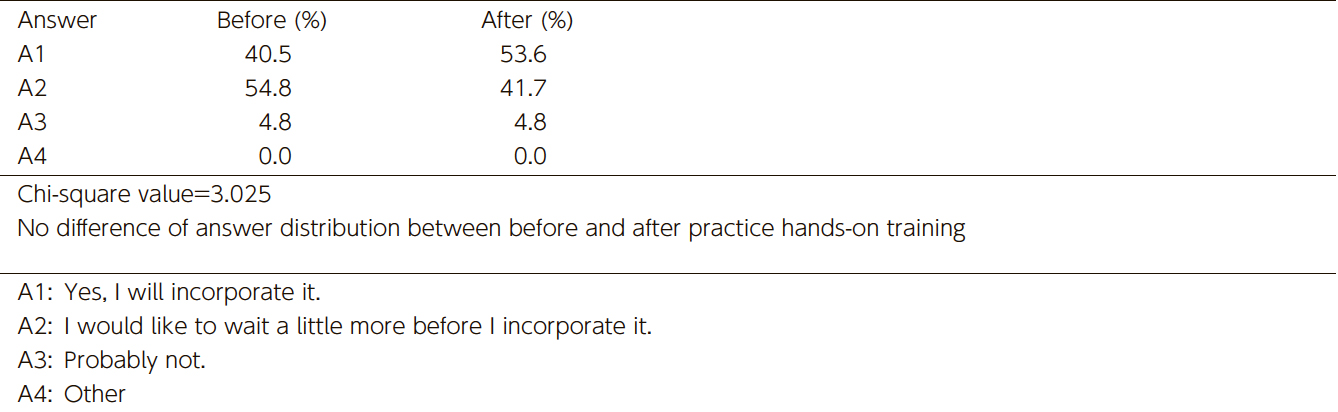
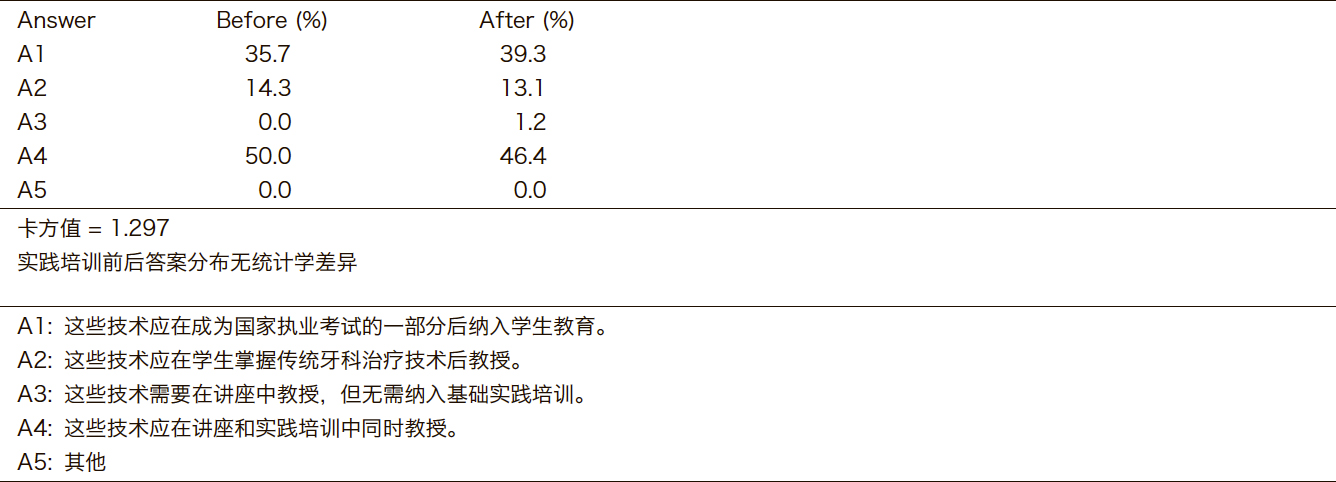
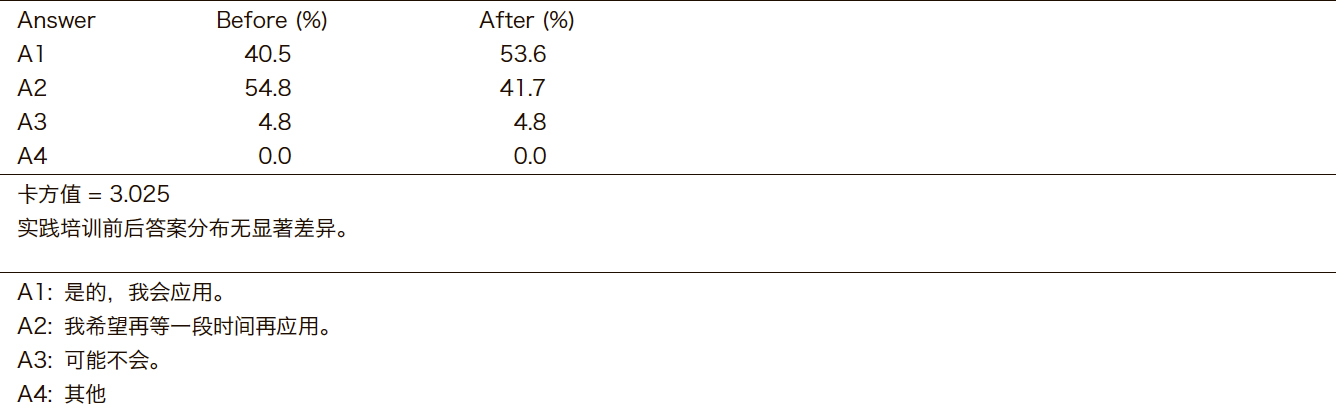
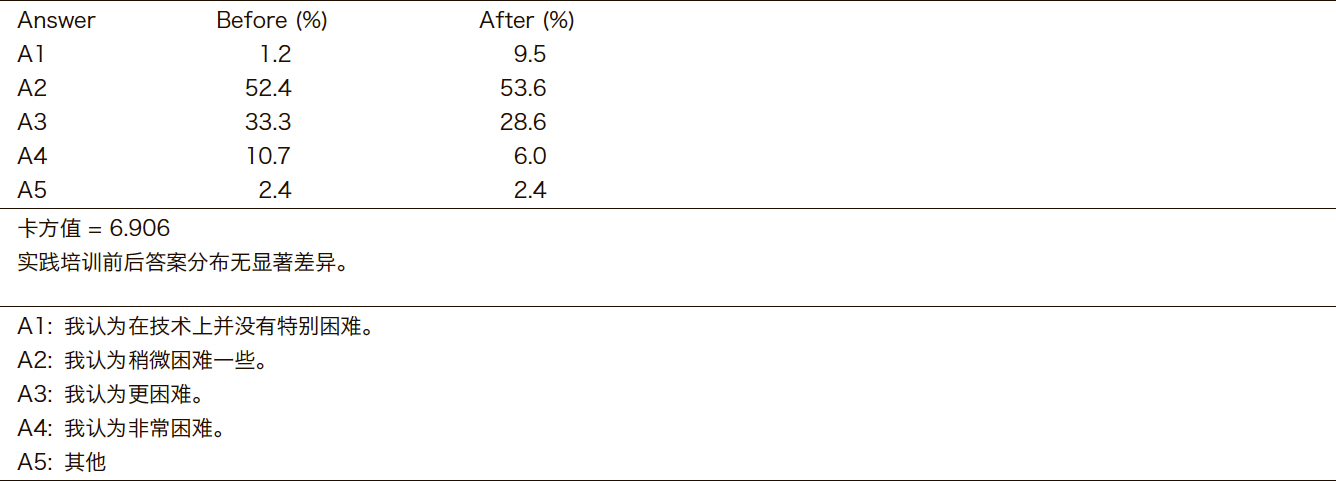
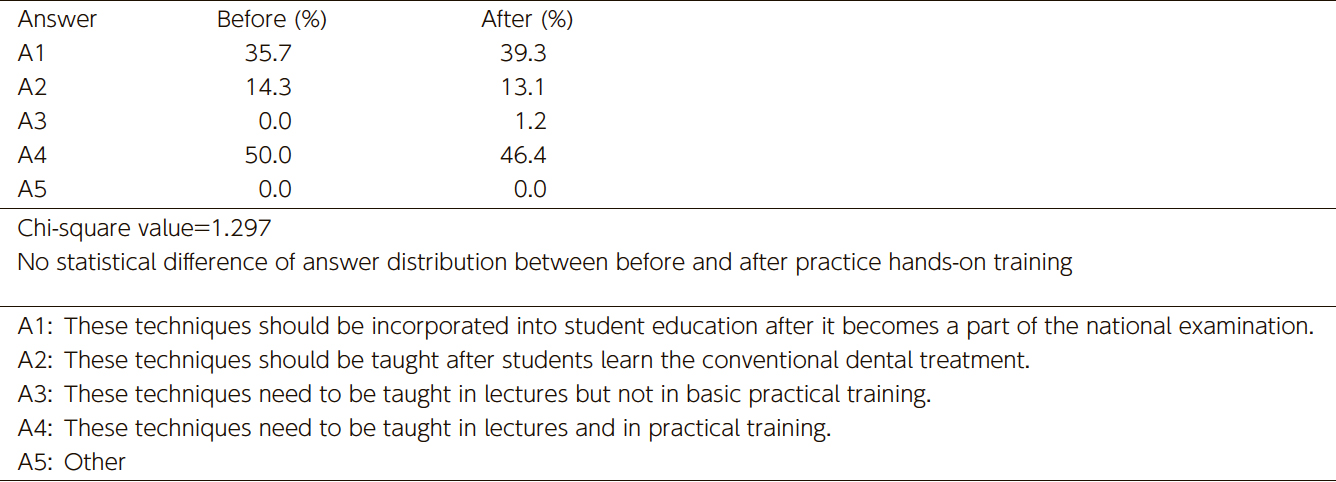
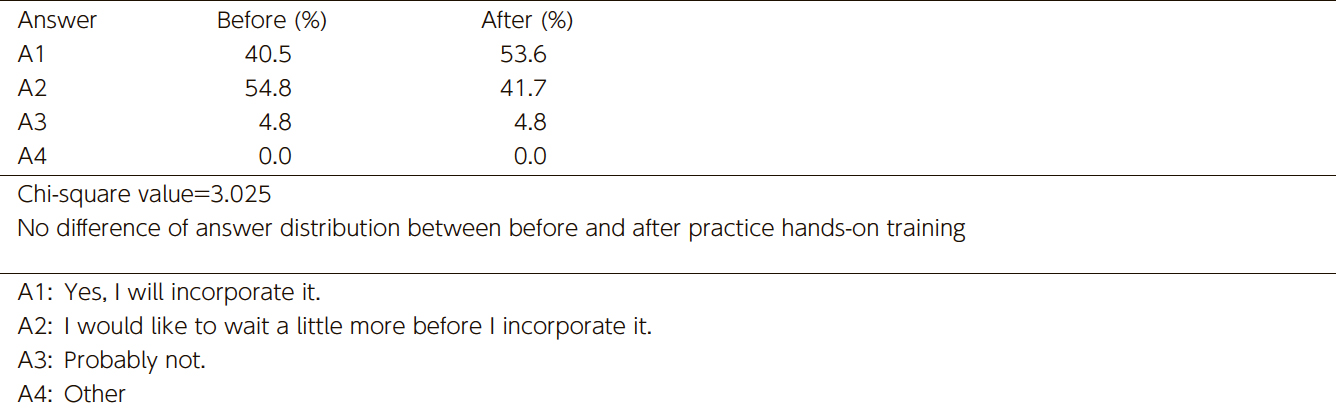
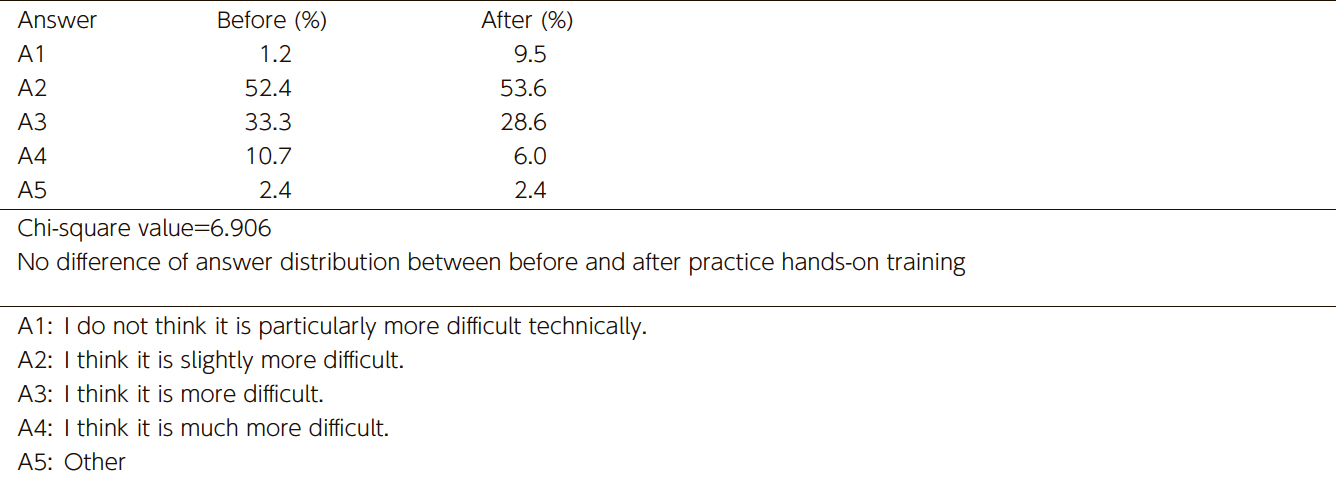
When students were asked about the appropriate timing for learning implant treatment techniques, the percentage of students who answered, "These techniques should be taught after students have mastered conventional dental treatments," decreased by 2.4% after the hands-on training. Meanwhile, the percentage of students who answered, "These techniques should be incorporated into education after they become part of the national board examination," increased by 3.6% (Table 2). There was no statistically significant difference in responses before and after the hands-on training regarding the timing of learning these implant techniques. Similarly, when asked whether they would incorporate implant treatment into their future practice, the percentage of students who answered positively ("I will incorporate it") increased by 3.1% after the hands-on training. The percentage of students who answered, "I would like to wait a little longer before incorporating it," decreased by 13.1% (Table 3). Regarding the difficulty of implant training, the number of students who responded, "I think implant treatment is technically very difficult," decreased after the training, while the number of students who responded, "I think it is not that difficult," increased (Table 4). However, these changes in the responses regarding the introduction of implant treatment and its difficulty before and after the hands-on training were not statistically significant.
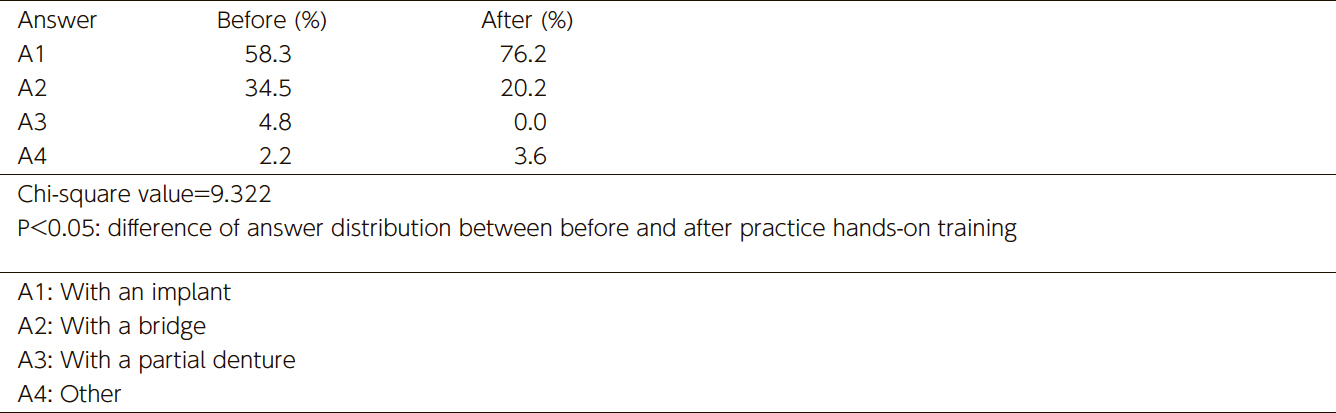
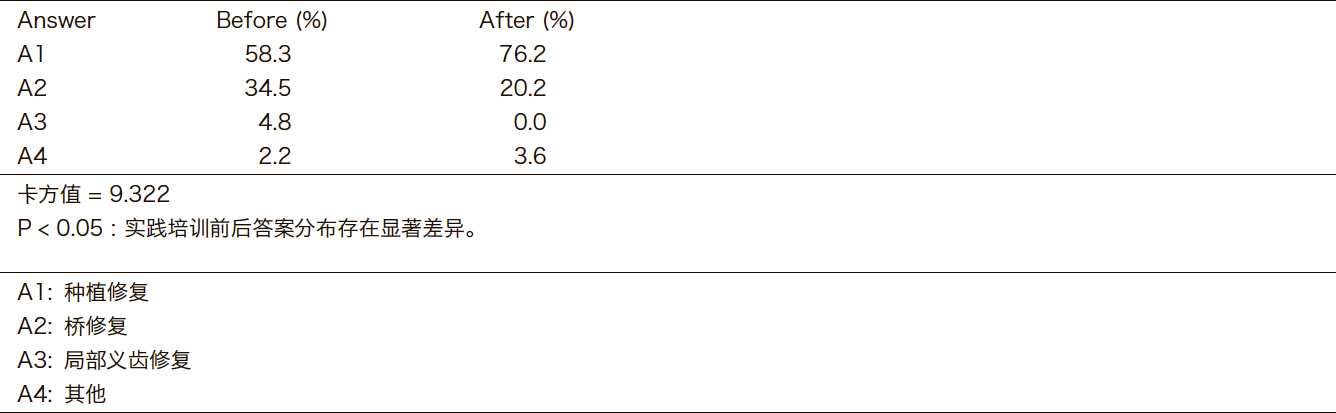
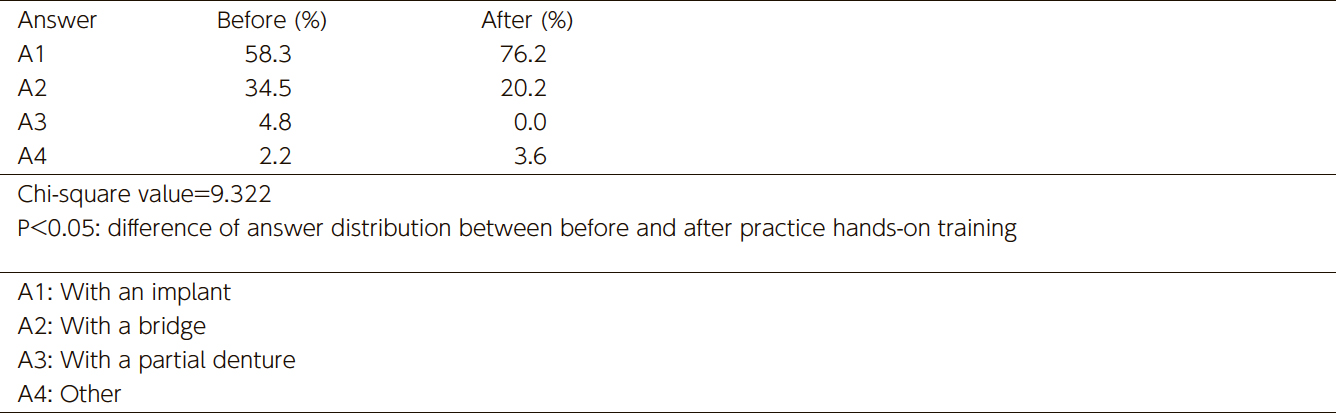
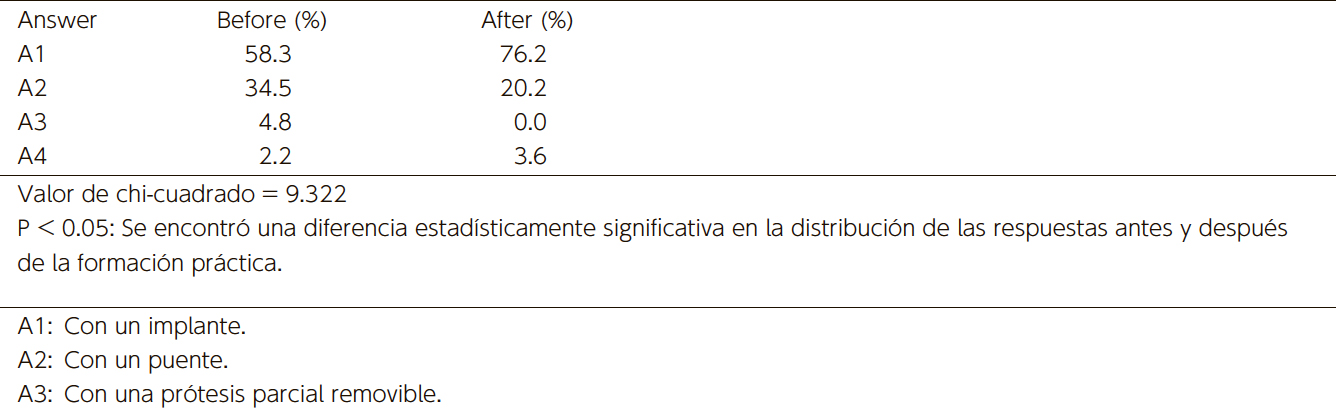
In contrast, when students were asked, "How would you restore a missing mandibular first molar?" the percentage of students who responded that they would use a bridge decreased by 14.3% after the hands-on training, whereas the percentage of students who responded that they would use an implant increased by 17.9% (Table 5). This change in the responses regarding students’ choices of prosthetic treatment for missing teeth was statistically significant.
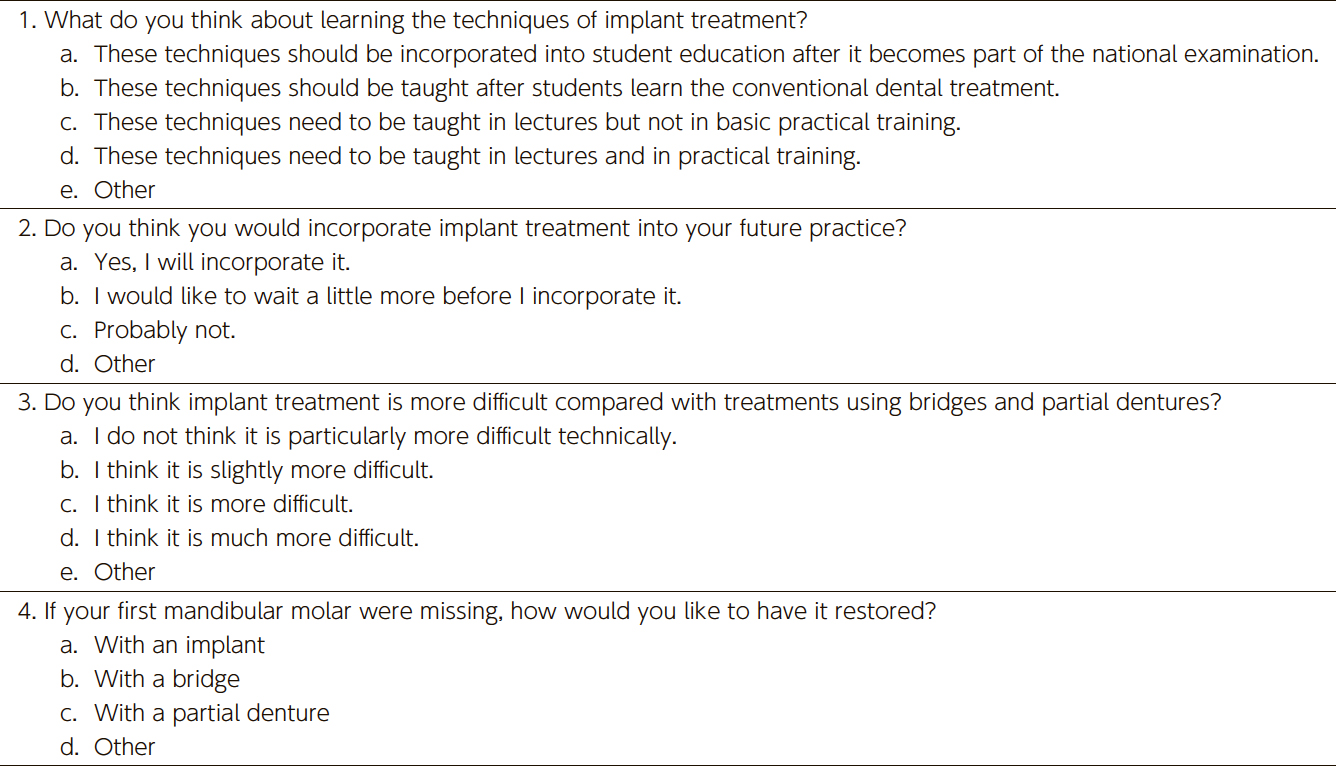
(Table 1) Survey questions asked of predoctoral dental students regarding implant training
(Table 2) Responses to the survey question "What do you think about learning the techniques of implant treatment?"
by percentage of total respondents (n=84)(Table 3) Responses to the survey question "Do you think you would incorporate implant treatment into your future practice?"
by percentage of total respondents (n=84)
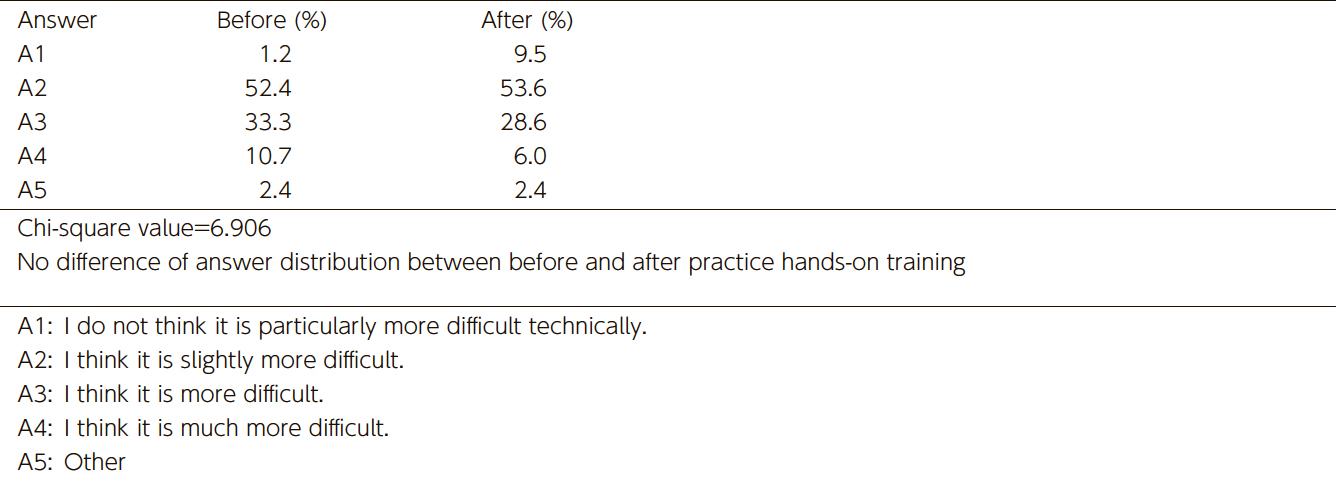
(Table 4) Responses to the survey question "Do you think implant treatment is more difficult compared with treatments
using bridges and partial dentures?" by percentage of total respondents (n=84)(Table 5) Responses to the survey question "If your first mandibular molar were missing, how would you like to have it restored?"
by percentage of total respondents (n=84)
4. Discussion
Compared to 15 years ago, while undergraduate education in implantology has become more comprehensive, there are still differences in educational approaches across institutions.19–23 Students who have received a thorough undergraduate education in implantology tend to be more proactive about implant treatments and are more likely to incorporate them into their practice after graduation.24
At our institution, implant training is mandatory for all undergraduate students. In the fourth year, students are required to attend 13 lectures and 2 computer simulation exercises, and they are tasked with developing an implant treatment plan for a case presented as a problem-solving exercise. In the fifth year, students are required to participate in hands-on practice using resin models with artificial gingiva. This hands-on training includes gingival incision, flap inversion, preparation of implant placement sites, implant placement, suturing, secondary surgery, abutment connection, and impression taking (both silicone and optical impressions). Students are trained to place 2 types of implant fixtures.
In 2009, a survey was conducted before and after hands-on training to investigate the awareness of undergraduate students regarding implant treatments.17 The results showed that significantly more students responded positively to the question, “Do you think you will incorporate implant treatment into your future practice?” after completing the hands-on training. Additionally, when asked whether they thought implant treatment was more difficult than treatments using bridges or partial dentures, significantly more students answered “not difficult” after the hands-on training, while the proportion of students who answered “difficult” significantly decreased. When asked how they would restore a missing mandibular first molar, significantly more students chose implants over bridges after the training.17
In the current survey, there was a significant increase in students choosing implants to restore a missing mandibular first molar after completing the hands-on training. This result is similar to the results obtained in 2009. However, no significant differences were found in the responses to the other survey questions before and after the hands-on training. These differences may reflect the influence of more advanced and comprehensive implant education at our institution since 2009, which has been driven by advancements in digital technology. For instance, the enhancement of computer simulations for treatment planning, the introduction of problem-solving exercises, and the addition of hands-on optical impression techniques using intraoral scanners could be contributing factors. On the other hand, a 2012 NHK television program, “Dental Implant Problems: Reasons for the Sharp Increase,” may have created a negative impression of implant treatments, potentially affecting some students’ attitudes.
Nevertheless, the significant increase in the percentage of students choosing implant treatment over alternatives after the hands-on training suggests that this training is effective in motivating students to engage with implant treatments.
In recent years, the adoption of digital technology in dental practice has advanced, especially in the field of implantology, where digital technology has been integrated relatively early. In dental education, the use of CAD/CAM for prosthetic fabrication, virtual simulation equipment, and even the application of artificial intelligence (AI) are being explored, with the expectation of developing highly effective educational systems.25–28
5. Conclusions
This study highlights the positive impact of hands-on implant training on predoctoral dental students' perceptions of implant treatment. Comparing the results with our previous survey from 2009, we observed that the training not only increased students' willingness to incorporate implant treatment into their future practice but also improved their confidence in performing implant-related procedures. Despite the advancements in implant education, the findings suggest that continuous improvements in training methods, particularly with the integration of digital technology, will further enhance students' readiness to provide implant-based care. Our results also underscore the importance of early exposure to implantology in dental curricula, as it fosters greater engagement and interest in implant treatment among future practitioners. Moving forward, further studies will be necessary to explore how these educational improvements influence students' long-term clinical practices and patient outcomes.
6. Disclosure
All authors have no conflicts of interest related to this research that need to be disclosed.
This work was supported by a Grant-in Aid for Scientific Research (JP24K12976 )
7. Refences
Weintraub AM, Seckinger R, Berthold P, Weintraub GS. Predoctoral Implant dentistry programs in U.S. dental schools. J Prosthodont 1995; 4(2): 116-21.
Seckinger R J, Weintraub A M, Berthold P, Weintraub G S. The status of undergraduate implant education in dental schools outside the United States. Implant Dent 1995; 4(2):105-9.
Bell F A, Hendricson W D. A problem-based course in dental implantology. J Dent Educ 1993; 57(9): 687-95.
Schnitman P A. Education in implant dentistry. J Am Dent Assoc 1990; 121(3): 330-2.
Simons A M, Bell F A, Beirne O R, McGlumphy E A. Undergraduate education in implant dentistry. Implant Dent 1995; 4(1): 40-3.
Ismail J Y. Predoctoral curriculum guidelines in implant dentistry. Int J Oral Implantol. 1990; 7(1): 67-9.
Seckinger R J, Weintraub A M, Berthold P, Weintraub G S. The status of undergraduate implant education in dental schools outside the United States. Implant Dent 1995; 4(2): 105-9.
Addy LD, Lynch CD, Locke M, Watts A, Gilmour AS. The teaching of implant dentistry in undergraduate dental schools in the United Kingdom and Ireland. Br Dent J. 2008 13; 205(11): 609-14.
Blum IR, O'Sullivan DJ, Jagger DC. A survey of undergraduate education in dental implantology in UK dental schools. Eur J Dent Educ. 2008; 12(4): 204-7.
Kronstrom M, McGrath L, Chaytor D. Implant dentistry in the undergraduate dental education program at Dalhousie University. Part 1: clinical outcomes. Int J Prosthodont 2008; 21(2): 124-8.
Petropoulos VC, Arbree NS, Tarnow D, Rethman M, Malmquist J, Valachovic R, Brunson WD, Alfano MC. Teaching implant dentistry in the predoctoral curriculum: a report from the ADEA Implant Workshop's survey of deans. J Dent Educ. 2006; 70(5): 580-8.
Lim MV, Afsharzand Z, Rashedi B, Petropoulos VC. Predoctoral implant education in U.S. dental schools. J Prosthodont. 2005; 14(1): 46-56.
Klokkevold PR. Implant education in the dental curriculum. J Calif Dent Assoc. 2001; 29(11): 747-55.
Wilcox C W, Huebner G R, Mattson J S, Nilsson D E, Blankenau R J. Placement and restoration of implants by predoctoral students: the Creighton experience. J Prosthodont 1997; 6(1): 61-5.
Maalhagh-Fard A, Nimmo A, Lepczyk JW, Pink FE. Implant dentistry in predoctoral education: the elective approach. J Prosthodont. 2002; 11(3): 202-7.
Kido H, Yamamoto K, Kakura K, Morinaga K, Matsuura T, Matsunaga T, Shimizu H, Takahashi Y, Sato H, Matsuura M. Students' opinion of a predoctoral implant training program. J Dent Educ. 2009; 73(11): 1279-85.
Muddugangadhar BC, Amarnath GS, Sonika R, Chheda PS, Garg A. Meta-analysis of Failure and Survival Rate of Implant-supported Single Crowns, Fixed Partial Denture, and Implant Tooth-supported Prostheses. J Int Oral Health. 2015 ; 7(9): 11-7.
Hare A, Bird S, Wright S, Ucer C, Khan RS. Current Undergraduate Dental Implantology Teaching in UK. Dent J (Basel). 2022; 10(7): 127. doi: 10.3390/dj10070127.
Seitz SD, Zimmermann RL, Hendricson WD. Expansion of a Predoctoral Surgical Implant Selective for Dental Students. J Dent Educ. 2016; 80(3): 328-33.
Prasad S, Bansal N. Predoctoral Dental Students' Perceptions of Dental Implant Training: Effect of Preclinical Simulation and Clinical Experience. J Dent Educ. 2017; 81(4): 395-403.
Missinne K, Duyck J, Naert I, Quirynen M, Bertrand S, Vandamme K. Oral Implant Restorations By Undergraduate Students: An Up To 5-Years Clinical Outcome. Int J Prosthodont. 2021; 34(4): 433–440.
Schweyen R, Al-Nawas B, Arnold C, Hey J. A cross-sectional survey of attitudes towards education in implant dentistry in the undergraduate dental curriculum. Int J Implant Dent. 2020 8; 6(1): 26.
Kattadiyil MT, Jekki R, Goodacre CJ, Baba NZ. Comparison of treatment outcomes in digital and conventional complete removable dental prosthesis fabrications in a predoctoral setting. J Prosthet Dent. 2015; 114(6): 818-25.
Huang Y, Hu Y, Chan U, Lai P, Sun Y, Dai J, Cheng X, Yang X. Student perceptions toward virtual reality training in dental implant education. PeerJ. 2023;11:e14857. doi: 10.7717/peerj.14857. eCollection 2023.
Fang Q, Reynaldi R, Araminta AS, Kamal I, Saini P, Afshari FS, Tan SC, Yuan JC, Qomariyah NN, Sukotjo C. Artificial Intelligence (AI)-driven dental education: Exploring the role of chatbots in a clinical learning environment. J Prosthet Dent. 2024: S0022-3913(24)00231-2. doi: 10.1016/j.prosdent.2024.03.038. Online ahead of print.
Surlari Z, Budală DG, Lupu CI, Stelea CG, Butnaru OM, Luchian I. Current Progress and Challenges of Using Artificial Intelligence in Clinical Dentistry-A Narrative Review. J Clin Med 2023; 12(23): 7378. doi: 10.3390/jcm12237378.
1) Section of Oral Implantology, Department of Oral Rehabilitation, Fukuoka Dental College
2) Educational Support and Institutional Research Office, Fukuoka Dental College
Direct correspondence and requests for reprints to Dr. Kae Kakura, Section of Oral Implantology, Department of Oral Rehabilitation. Fukuoka Dental College, 2-15-1 Tamura, Sawara-ku, Fukuoka, 814-0193, Japan; 81-92-801-0425 phone; +81-92-801-0513 fax; [email protected].
Weintraub AM, Seckinger R, Berthold P, Weintraub GS. Predoctoral Implant dentistry programs in U.S. dental schools. J Prosthodont 1995; 4(2): 116-21.
Seckinger R J, Weintraub A M, Berthold P, Weintraub G S. The status of undergraduate implant education in dental schools outside the United States. Implant Dent 1995; 4(2):105-9.
Bell F A, Hendricson W D. A problem-based course in dental implantology. J Dent Educ 1993; 57(9): 687-95.
Schnitman P A. Education in implant dentistry. J Am Dent Assoc 1990; 121(3): 330-2.
Simons A M, Bell F A, Beirne O R, McGlumphy E A. Undergraduate education in implant dentistry. Implant Dent 1995; 4(1): 40-3.
Ismail J Y. Predoctoral curriculum guidelines in implant dentistry. Int J Oral Implantol. 1990; 7(1): 67-9.
Seckinger R J, Weintraub A M, Berthold P, Weintraub G S. The status of undergraduate implant education in dental schools outside the United States. Implant Dent 1995; 4(2): 105-9.
Addy LD, Lynch CD, Locke M, Watts A, Gilmour AS. The teaching of implant dentistry in undergraduate dental schools in the United Kingdom and Ireland. Br Dent J. 2008 13; 205(11): 609-14.
Blum IR, O'Sullivan DJ, Jagger DC. A survey of undergraduate education in dental implantology in UK dental schools. Eur J Dent Educ. 2008; 12(4): 204-7.
Kronstrom M, McGrath L, Chaytor D. Implant dentistry in the undergraduate dental education program at Dalhousie University. Part 1: clinical outcomes. Int J Prosthodont 2008; 21(2): 124-8.
Petropoulos VC, Arbree NS, Tarnow D, Rethman M, Malmquist J, Valachovic R, Brunson WD, Alfano MC. Teaching implant dentistry in the predoctoral curriculum: a report from the ADEA Implant Workshop's survey of deans. J Dent Educ. 2006; 70(5): 580-8.
Lim MV, Afsharzand Z, Rashedi B, Petropoulos VC. Predoctoral implant education in U.S. dental schools. J Prosthodont. 2005; 14(1): 46-56.
Klokkevold PR. Implant education in the dental curriculum. J Calif Dent Assoc. 2001; 29(11): 747-55.
Wilcox C W, Huebner G R, Mattson J S, Nilsson D E, Blankenau R J. Placement and restoration of implants by predoctoral students: the Creighton experience. J Prosthodont 1997; 6(1): 61-5.
Maalhagh-Fard A, Nimmo A, Lepczyk JW, Pink FE. Implant dentistry in predoctoral education: the elective approach. J Prosthodont. 2002; 11(3): 202-7.
Kido H, Yamamoto K, Kakura K, Morinaga K, Matsuura T, Matsunaga T, Shimizu H, Takahashi Y, Sato H, Matsuura M. Students' opinion of a predoctoral implant training program. J Dent Educ. 2009; 73(11): 1279-85.
Muddugangadhar BC, Amarnath GS, Sonika R, Chheda PS, Garg A. Meta-analysis of Failure and Survival Rate of Implant-supported Single Crowns, Fixed Partial Denture, and Implant Tooth-supported Prostheses. J Int Oral Health. 2015 ; 7(9): 11-7.
Hare A, Bird S, Wright S, Ucer C, Khan RS. Current Undergraduate Dental Implantology Teaching in UK. Dent J (Basel). 2022; 10(7): 127. doi: 10.3390/dj10070127.
Seitz SD, Zimmermann RL, Hendricson WD. Expansion of a Predoctoral Surgical Implant Selective for Dental Students. J Dent Educ. 2016; 80(3): 328-33.
Prasad S, Bansal N. Predoctoral Dental Students' Perceptions of Dental Implant Training: Effect of Preclinical Simulation and Clinical Experience. J Dent Educ. 2017; 81(4): 395-403.
Missinne K, Duyck J, Naert I, Quirynen M, Bertrand S, Vandamme K. Oral Implant Restorations By Undergraduate Students: An Up To 5-Years Clinical Outcome. Int J Prosthodont. 2021; 34(4): 433–440.
Schweyen R, Al-Nawas B, Arnold C, Hey J. A cross-sectional survey of attitudes towards education in implant dentistry in the undergraduate dental curriculum. Int J Implant Dent. 2020 8; 6(1): 26.
Kattadiyil MT, Jekki R, Goodacre CJ, Baba NZ. Comparison of treatment outcomes in digital and conventional complete removable dental prosthesis fabrications in a predoctoral setting. J Prosthet Dent. 2015; 114(6): 818-25.
Huang Y, Hu Y, Chan U, Lai P, Sun Y, Dai J, Cheng X, Yang X. Student perceptions toward virtual reality training in dental implant education. PeerJ. 2023;11:e14857. doi: 10.7717/peerj.14857. eCollection 2023.
Fang Q, Reynaldi R, Araminta AS, Kamal I, Saini P, Afshari FS, Tan SC, Yuan JC, Qomariyah NN, Sukotjo C. Artificial Intelligence (AI)-driven dental education: Exploring the role of chatbots in a clinical learning environment. J Prosthet Dent. 2024: S0022-3913(24)00231-2. doi: 10.1016/j.prosdent.2024.03.038. Online ahead of print.
Surlari Z, Budală DG, Lupu CI, Stelea CG, Butnaru OM, Luchian I. Current Progress and Challenges of Using Artificial Intelligence in Clinical Dentistry-A Narrative Review. J Clin Med 2023; 12(23): 7378. doi: 10.3390/jcm12237378.
1) Section of Oral Implantology, Department of Oral Rehabilitation, Fukuoka Dental College
2) Educational Support and Institutional Research Office, Fukuoka Dental College
Direct correspondence and requests for reprints to Dr. Kae Kakura, Section of Oral Implantology, Department
of Oral Rehabilitation. Fukuoka Dental College, 2-15-1 Tamura, Sawara-ku, Fukuoka, 814-0193, Japan;
81-92-801-0425 phone; +81-92-801-0513 fax; [email protected].
インプラント実習では,テーパー型インプラント(Replace Select Tapered, Nobel Biocare Japan, 東京,日本)およびストレート型インプラント(Replace Select
Straight, Nobel Biocare Japan,
東京,日本)を使用した(図2).学生は,歯肉切開,歯肉弁剥離,インプラント埋入部位の決定,埋入窩の形成,インプラント埋入,および縫合の手技を習得した(図3).さらに,インプラントプラットフォームの開窓,アバットメントの装着,および印象採得の方法についても実践的に学習した(図4a,b).
(図1) A simulation model for predoctoral implant training(図2) Two types of implants for predoctoral training(図3) Implant placement procedure on simulation model(図4a) Implant analogs connection procedure with silicone
impression(図4b) Optical impression procedure using an intraoral scanner
(表1) Survey questions asked of predoctoral dental students regarding implant training
(表2) Responses to the survey question "What do you think about learning the techniques of implant treatment?"
by percentage of total respondents (n=84)(表3) Responses to the survey question "Do you think you would incorporate implant treatment into your future practice?"
by percentage of total respondents (n=84)
(表4) Responses to the survey question "Do you think implant treatment is more difficult compared with treatments
using bridges and partial dentures?" by percentage of total respondents (n=84)(表5) Responses to the survey question "If your first mandibular molar were missing, how would you like to have it restored?"
by percentage of total respondents (n=84)
Weintraub AM, Seckinger R, Berthold P, Weintraub GS. Predoctoral Implant dentistry programs in U.S. dental schools. J Prosthodont 1995; 4(2): 116-21.
Seckinger R J, Weintraub A M, Berthold P, Weintraub G S. The status of undergraduate implant education in dental schools outside the United States. Implant Dent 1995; 4(2):105-9.
Bell F A, Hendricson W D. A problem-based course in dental implantology. J Dent Educ 1993; 57(9): 687-95.
Schnitman P A. Education in implant dentistry. J Am Dent Assoc 1990; 121(3): 330-2.
Simons A M, Bell F A, Beirne O R, McGlumphy E A. Undergraduate education in implant dentistry. Implant Dent 1995; 4(1): 40-3.
Ismail J Y. Predoctoral curriculum guidelines in implant dentistry. Int J Oral Implantol. 1990; 7(1): 67-9.
Seckinger R J, Weintraub A M, Berthold P, Weintraub G S. The status of undergraduate implant education in dental schools outside the United States. Implant Dent 1995; 4(2): 105-9.
Addy LD, Lynch CD, Locke M, Watts A, Gilmour AS. The teaching of implant dentistry in undergraduate dental schools in the United Kingdom and Ireland. Br Dent J. 2008 13; 205(11): 609-14.
Blum IR, O'Sullivan DJ, Jagger DC. A survey of undergraduate education in dental implantology in UK dental schools. Eur J Dent Educ. 2008; 12(4): 204-7.
Kronstrom M, McGrath L, Chaytor D. Implant dentistry in the undergraduate dental education program at Dalhousie University. Part 1: clinical outcomes. Int J Prosthodont 2008; 21(2): 124-8.
Petropoulos VC, Arbree NS, Tarnow D, Rethman M, Malmquist J, Valachovic R, Brunson WD, Alfano MC. Teaching implant dentistry in the predoctoral curriculum: a report from the ADEA Implant Workshop's survey of deans. J Dent Educ. 2006; 70(5): 580-8.
Lim MV, Afsharzand Z, Rashedi B, Petropoulos VC. Predoctoral implant education in U.S. dental schools. J Prosthodont. 2005; 14(1): 46-56.
Klokkevold PR. Implant education in the dental curriculum. J Calif Dent Assoc. 2001; 29(11): 747-55.
Wilcox C W, Huebner G R, Mattson J S, Nilsson D E, Blankenau R J. Placement and restoration of implants by predoctoral students: the Creighton experience. J Prosthodont 1997; 6(1): 61-5.
Maalhagh-Fard A, Nimmo A, Lepczyk JW, Pink FE. Implant dentistry in predoctoral education: the elective approach. J Prosthodont. 2002; 11(3): 202-7.
Kido H, Yamamoto K, Kakura K, Morinaga K, Matsuura T, Matsunaga T, Shimizu H, Takahashi Y, Sato H, Matsuura M. Students' opinion of a predoctoral implant training program. J Dent Educ. 2009; 73(11): 1279-85.
Muddugangadhar BC, Amarnath GS, Sonika R, Chheda PS, Garg A. Meta-analysis of Failure and Survival Rate of Implant-supported Single Crowns, Fixed Partial Denture, and Implant Tooth-supported Prostheses. J Int Oral Health. 2015 ; 7(9): 11-7.
Hare A, Bird S, Wright S, Ucer C, Khan RS. Current Undergraduate Dental Implantology Teaching in UK. Dent J (Basel). 2022; 10(7): 127. doi: 10.3390/dj10070127.
Seitz SD, Zimmermann RL, Hendricson WD. Expansion of a Predoctoral Surgical Implant Selective for Dental Students. J Dent Educ. 2016; 80(3): 328-33.
Prasad S, Bansal N. Predoctoral Dental Students' Perceptions of Dental Implant Training: Effect of Preclinical Simulation and Clinical Experience. J Dent Educ. 2017; 81(4): 395-403.
Missinne K, Duyck J, Naert I, Quirynen M, Bertrand S, Vandamme K. Oral Implant Restorations By Undergraduate Students: An Up To 5-Years Clinical Outcome. Int J Prosthodont. 2021; 34(4): 433–440.
Schweyen R, Al-Nawas B, Arnold C, Hey J. A cross-sectional survey of attitudes towards education in implant dentistry in the undergraduate dental curriculum. Int J Implant Dent. 2020 8; 6(1): 26.
Kattadiyil MT, Jekki R, Goodacre CJ, Baba NZ. Comparison of treatment outcomes in digital and conventional complete removable dental prosthesis fabrications in a predoctoral setting. J Prosthet Dent. 2015; 114(6): 818-25.
Huang Y, Hu Y, Chan U, Lai P, Sun Y, Dai J, Cheng X, Yang X. Student perceptions toward virtual reality training in dental implant education. PeerJ. 2023;11:e14857. doi: 10.7717/peerj.14857. eCollection 2023.
Fang Q, Reynaldi R, Araminta AS, Kamal I, Saini P, Afshari FS, Tan SC, Yuan JC, Qomariyah NN, Sukotjo C. Artificial Intelligence (AI)-driven dental education: Exploring the role of chatbots in a clinical learning environment. J Prosthet Dent. 2024: S0022-3913(24)00231-2. doi: 10.1016/j.prosdent.2024.03.038. Online ahead of print.
Surlari Z, Budală DG, Lupu CI, Stelea CG, Butnaru OM, Luchian I. Current Progress and Challenges of Using Artificial Intelligence in Clinical Dentistry-A Narrative Review. J Clin Med 2023; 12(23): 7378. doi: 10.3390/jcm12237378.
1) Section of Oral Implantology, Department of Oral Rehabilitation, Fukuoka Dental College
2) Educational Support and Institutional Research Office, Fukuoka Dental College
Las correspondencias directas y las solicitudes de reimpresiones deben dirigirse a la Dra. Kae Kakura, Sección de Implantología Oral, Departamento de Rehabilitación Oral, Facultad de Odontología de Fukuoka, 2-15-1 Tamura, Sawara-ku, Fukuoka, 814-0193, Japón; Teléfono: +81-92-801-0425; Fax: +81-92-801-0513; Correo electrónico: [email protected].
Resumen
Objetivos: La integración de la implantología en la educación dental es fundamental para preparar a los estudiantes predoctorales para la práctica clínica moderna. Este estudio tuvo como objetivo evaluar el impacto de un programa de formación práctica en implantología sobre la percepción de los estudiantes respecto al tratamiento con implantes y comparar los resultados con una encuesta similar realizada hace 15 años. Métodos: Los estudiantes de odontología participaron en una sesión integral de formación práctica en implantología durante su rotación clínica en el quinto año. La formación incluyó técnicas como incisión gingival, elevación de colgajo, colocación de implantes, sutura y toma de impresiones, utilizando métodos convencionales y digitales. La percepción de los estudiantes sobre el tratamiento con implantes se evaluó mediante un cuestionario aplicado antes y después de la formación, centrándose en temas como la necesidad de educación en implantología y la posible dificultad del tratamiento. Resultados: En 2024, 84 estudiantes participaron en la formación práctica y completaron el cuestionario. Los resultados revelaron un aumento significativo en el número de estudiantes que prefirieron los implantes sobre otras opciones de tratamiento para restaurar un primer molar inferior ausente. Aunque no se observaron diferencias significativas en la percepción de la dificultad del tratamiento con implantes, sí se evidenció un cambio positivo en la actitud de los estudiantes hacia la incorporación de la implantología en su futura práctica clínica. Conclusiones: Los hallazgos sugieren que los avances en la formación en implantología, especialmente la inclusión de tecnologías digitales, han contribuido a una educación más completa y efectiva. Este estudio también demuestra que la formación práctica desempeña un papel clave en la motivación de los estudiantes para adoptar la implantología en su ejercicio clínico. Los resultados subrayan la importancia de integrar tecnologías de vanguardia y una formación integral en la enseñanza de la implantología para fomentar la confianza y la competencia en los futuros profesionales.
Desde principios de la década de 1990, se ha reconocido la necesidad de integrar la implantología en la educación odontológica, y se han reportado ampliamente diversos métodos para lograrlo.1–7 Un informe de hace aproximadamente 20 años señaló que, aunque muchas universidades de odontología habían incorporado la implantología en sus planes de estudio, existían diferencias significativas en el uso de conferencias, entrenamiento con modelos y el nivel de experiencia clínica proporcionada.8–15 En una encuesta realizada en 2005 sobre la educación en implantología en 56 universidades odontológicas europeas, Afsharzand et al. informaron que, aunque la mayoría de las universidades exigían un curso de implantología como parte de la formación predoctoral, el contenido de los programas educativos en implantología variaba ampliamente entre las instituciones.13 Además, Maalhagh-Fard et al. realizaron una encuesta entre los graduados tras la implementación de un programa electivo predoctoral en implantología en la Facultad de Odontología de la Universidad de Detroit Mercy. Los resultados indicaron una fuerte correlación positiva entre la participación en el programa y la introducción del tratamiento con implantes en la práctica clínica de posgrado.16
Cuando el tratamiento con implantes comenzó a ganar popularidad, los odontólogos solían adquirir conocimientos y técnicas relacionadas con los implantes a través de talleres y conferencias dirigidas por fabricantes, con oportunidades limitadas para obtener una base de conocimientos sólida. Un currículo sistemático que desarrolle conocimientos fundamentales sobre implantología desde la formación predoctoral hasta el nivel de posgrado es esencial para preparar a los estudiantes en la comprensión integral del tratamiento con implantes.
En este contexto, en 2003, la Facultad de Odontología de Fukuoka comenzó a ofrecer formación en implantología a estudiantes predoctorales, utilizando modelos. La formación inicial consistía en colocar un solo tipo de implante en un modelo de poliuretano simple. A partir de 2004, el currículo se mejoró para incluir varios tipos de implantes y un modelo de entrenamiento práctico desarrollado internamente. Todos los estudiantes predoctorales deben completar esta formación obligatoriamente. Además, los estudiantes asisten a 13 conferencias sobre los principios fundamentales del tratamiento con implantes y participan en dos ejercicios de planificación de tratamientos utilizando simulaciones de implantes junto con la formación práctica. Para evaluar el impacto educativo de la implantología en ese momento, en 2009 realizamos un estudio comparativo sobre la percepción de los estudiantes antes y después del entrenamiento práctico.17
Han pasado 15 años desde aquel informe, y el tratamiento con implantes es ahora reconocido como una opción prioritaria para la rehabilitación protésica de dientes ausentes.18 Además, la enseñanza de la implantología se ha implementado en la mayoría de las universidades odontológicas de Japón. En medio de estos cambios, el contenido de la educación en implantología en nuestra universidad también ha evolucionado. Por lo tanto, realizamos una encuesta similar a la de hace 15 años para analizar los cambios en la percepción de los estudiantes sobre el tratamiento con implantes antes y después del entrenamiento práctico.
2. Métodos
2.1 Aprobación ética
Este estudio se llevó a cabo con la aprobación del Comité de Revisión Ética de la Facultad de Odontología de Fukuoka (número de aprobación 612).
2.2 Educación en implantología y formación práctica
Se realizó una sesión de formación práctica en colocación de implantes durante el período de formación clínica para los estudiantes de quinto año en el Hospital de la Facultad de Odontología de Fukuoka. La formación clínica para los estudiantes de pregrado comprendió 60 días en el primer semestre y 87 días en el segundo semestre. Durante este período, los estudiantes rotaron por los departamentos de Implantología y Prótesis, Odontología Conservadora y Periodoncia, Cirugía Oral, Odontología Pediátrica y Ortodoncia, Odontología General, Odontología para Pacientes con Discapacidades, Atención Dental Domiciliaria y Medicina, adquiriendo experiencia práctica al participar en actividades clínicas.
La formación clínica en implantología se llevó a cabo durante un día como parte de la formación en odontología restauradora, que constó de 15 días en el primer semestre y 16 días en el segundo semestre. Esta capacitación incluyó observación en el sillón dental y asistencia al instructor. Aproximadamente 10 estudiantes participaron en cada sesión de formación práctica, con un instructor asignado para guiar a dos o tres estudiantes.
Usando modelos especializados, los estudiantes practicaron una serie de procedimientos, incluyendo incisión gingival, elevación del colgajo, preparación del sitio para el implante, colocación del implante, sutura y cirugía secundaria (Figs.1,2). Además, practicaron técnicas de toma de impresiones utilizando tanto impresiones de silicona con cubeta abierta como impresiones ópticas con un escáner intraoral (Figs.3,4). A través de esta formación práctica, los estudiantes adquirieron los conocimientos y habilidades necesarios para explicar la necesidad de tratamientos protésicos para restaurar dientes ausentes y presentar opciones de tratamiento a los pacientes. Todos los estudiantes completaron estos procedimientos dentro del período de entrenamiento de un día.
2.3 Modelos de implantología
Se utilizó un modelo de simulación desarrollado específicamente para esta formación práctica (Nisshin Dental Products Co., Ltd., Kioto, Japón) (Fig.1). La región del hueso alveolar para el entrenamiento en implantes consistía en tres capas: encía de silicona, hueso cortical y hueso esponjoso. La zona edéntula podía ser reemplazada con resina acrílica, permitiendo su uso en la capacitación para la fabricación de prótesis parciales removibles. De este modo, los estudiantes podían utilizar el mismo modelo tanto para el entrenamiento en implantes como en prótesis removibles.
Para la formación en implantología, se utilizaron implantes cónicos (Replace Select Tapered, Nobel Biocare Japan, Tokio, Japón) e implantes rectos (Replace Select Straight, Nobel Biocare Japan, Tokio, Japón) (Fig.2). Los estudiantes aprendieron técnicas como incisión gingival, elevación del colgajo, determinación del sitio de colocación del implante, preparación del alvéolo para el implante, inserción del implante y sutura (Fig.3). Además, fueron entrenados en la exposición de la plataforma del implante, conexión del pilar protésico y métodos de toma de impresiones (Fig.4a,b).
(Fig.1) A simulation model for predoctoral implant training(Fig.2) Two types of implants for predoctoral training(Fig.3) Implant placement procedure on simulation model(Fig.4a) Implant analogs connection procedure with silicone
impression(Fig.4b) Optical impression procedure using an intraoral scanner
2.4 Cuestionario
Para evaluar la percepción de los estudiantes sobre el tratamiento con implantes, se administró un cuestionario a todos los participantes del programa de formación en implantología (Tabla 1). El cuestionario se aplicó inmediatamente antes y después del entrenamiento. A los estudiantes se les preguntó si estaban de acuerdo o en desacuerdo con temas como la necesidad de formación y conferencias sobre implantología, así como la necesidad del tratamiento con implantes. Sus respuestas fueron comparadas antes y después de la formación. Los análisis estadísticos se realizaron utilizando IBM® SPSS® Statistics Version 22 (IBM, Armonk, EE.UU.).
3. Resultados
En 2024, un total de 84 estudiantes (47 hombres y 37 mujeres) participaron en la formación práctica en implantología. La tasa de respuesta al cuestionario fue del 100%.
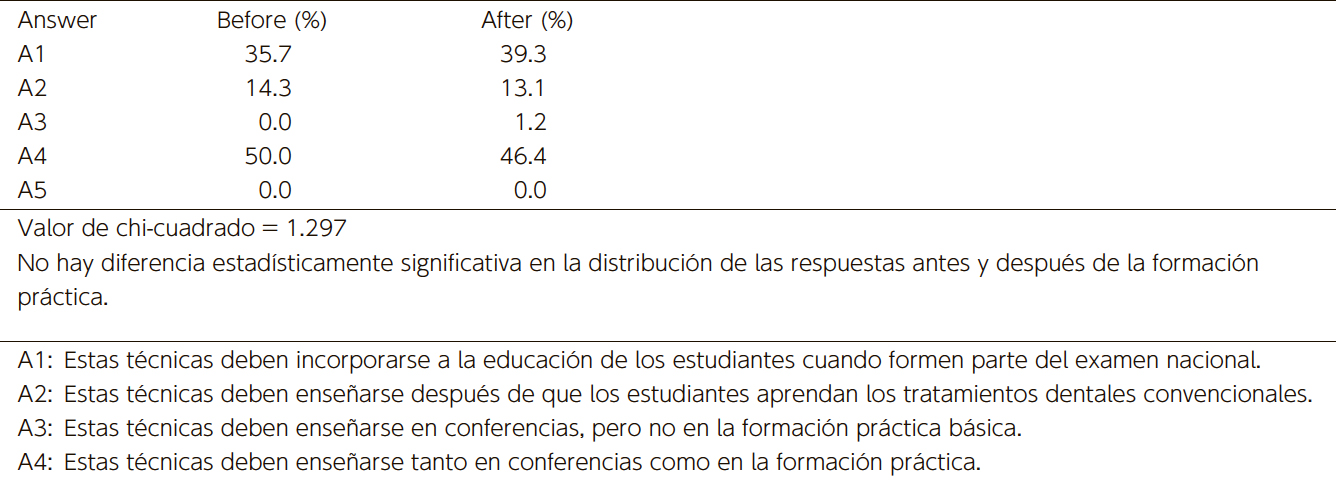
Cuando se preguntó a los estudiantes sobre el momento adecuado para aprender las técnicas de tratamiento con implantes, el porcentaje de aquellos que respondieron "Estas técnicas deben enseñarse después de que los estudiantes dominen los tratamientos dentales convencionales" disminuyó en un 2.4% después de la formación práctica. Mientras tanto, el porcentaje de estudiantes que respondieron "Estas técnicas deben incorporarse a la educación cuando formen parte del examen nacional de certificación" aumentó en un 3.6% (Tabla 2). No hubo diferencias estadísticamente significativas en las respuestas antes y después de la formación práctica con respecto al momento adecuado para aprender estas técnicas.
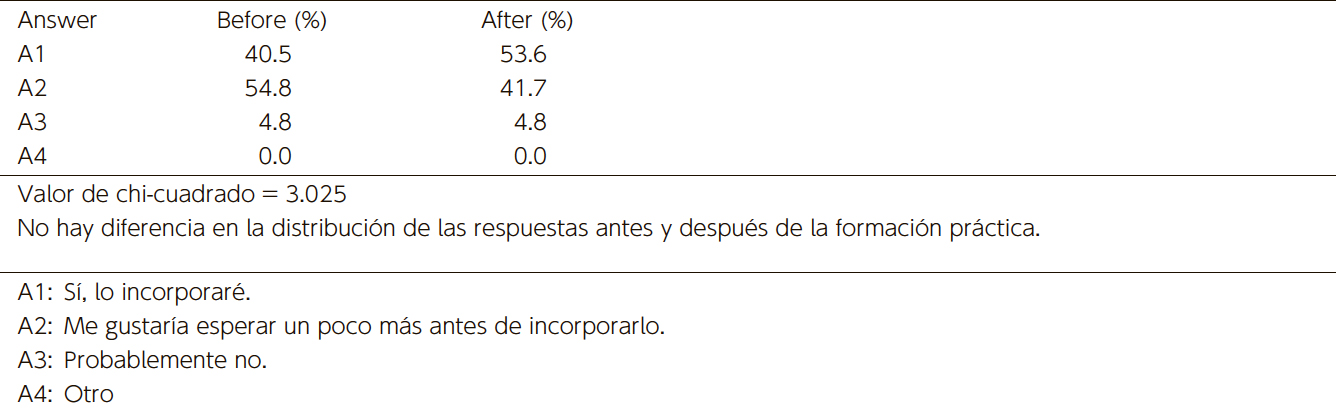
De manera similar, cuando se les preguntó si incorporarían el tratamiento con implantes en su práctica futura, el porcentaje de estudiantes que respondieron de manera positiva ("Lo incorporaré") aumentó en un 3.1% después de la formación práctica. Además, el porcentaje de estudiantes que respondieron "Me gustaría esperar un poco más antes de incorporarlo" disminuyó en un 13.1% (Tabla 3).
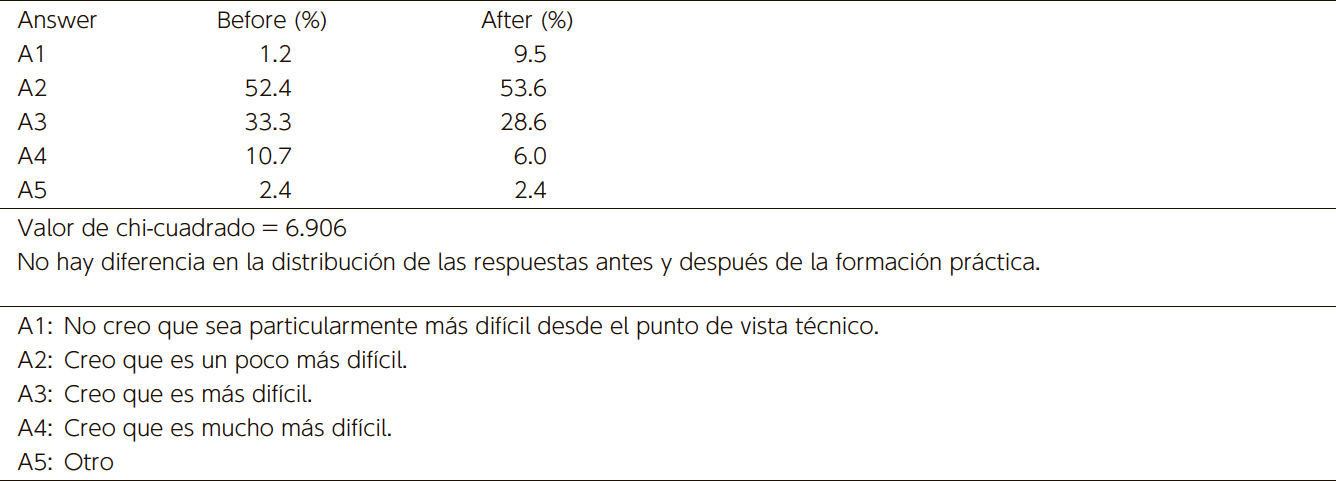
En cuanto a la dificultad de la formación en implantología, el número de estudiantes que respondieron "Creo que el tratamiento con implantes es técnicamente muy difícil" disminuyó después de la formación, mientras que el número de estudiantes que respondieron "Creo que no es tan difícil" aumentó (Tabla 4). Sin embargo, estos cambios en las respuestas sobre la introducción del tratamiento con implantes y su dificultad antes y después de la formación práctica no fueron estadísticamente significativos.
En contraste, cuando se preguntó a los estudiantes "¿Cómo restauraría un primer molar mandibular ausente?", el porcentaje de estudiantes que eligieron un puente disminuyó en un 14.3% después de la formación práctica, mientras que el porcentaje de estudiantes que eligieron un implante aumentó en un 17.9% (Tabla 5). Este cambio en la elección del tratamiento protésico para dientes ausentes fue estadísticamente significativo.
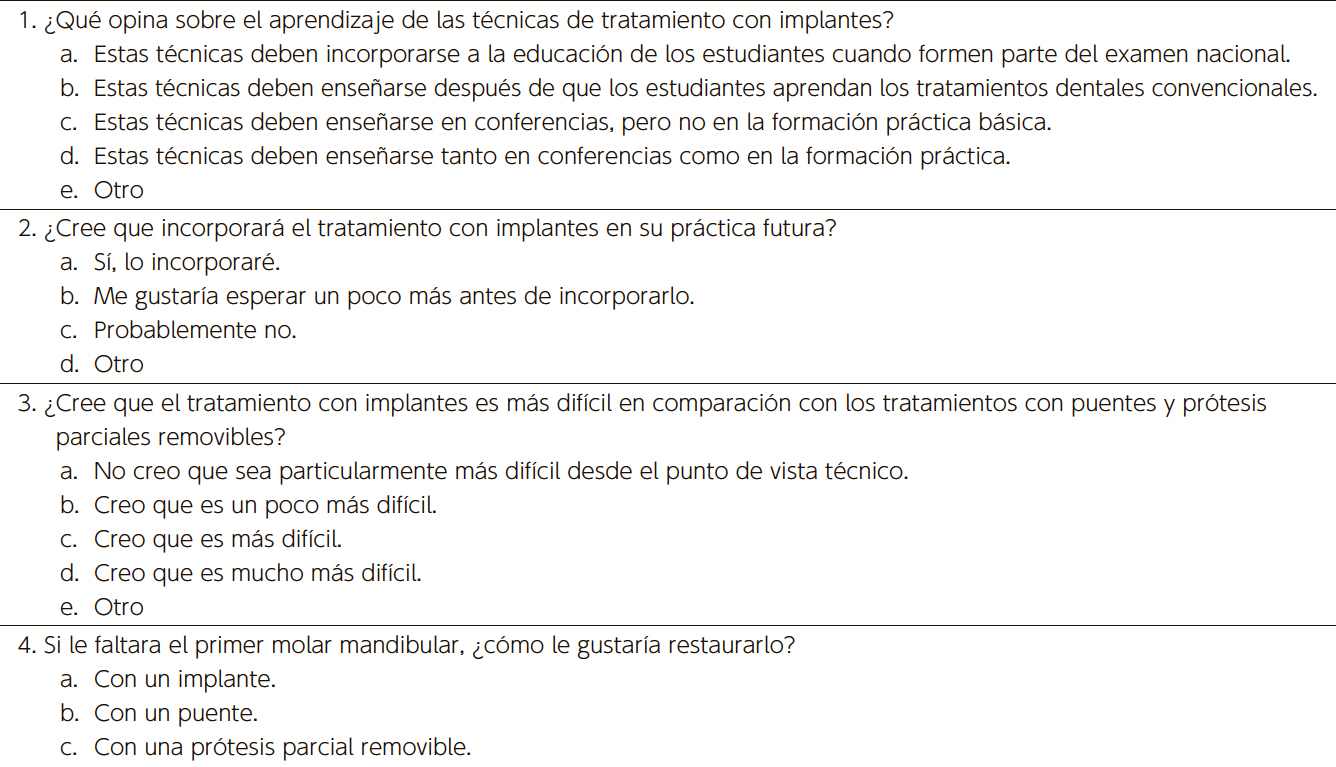
(Tabla 1) Preguntas de la encuesta realizadas a estudiantes de odontología predoctoral sobre
la formación en implantología(Tabla 2) Respuestas a la pregunta de la encuesta "¿Qué opina sobre el aprendizaje de
las técnicas de tratamiento con implantes?" por porcentaje del total de encuestados (n=84)
(Tabla 3) Respuestas a la pregunta de la encuesta "¿Cree que incorporará el tratamiento con implantes en su práctica futura?"
por porcentaje del total de encuestados (n=84)
(Tabla 4) Respuestas a la pregunta de la encuesta "¿Cree que el tratamiento con implantes es más difícil en comparación con los tratamientos con puentes y prótesis parciales removibles?" por porcentaje del total de encuestados (n=84)(Tabla 5) Respuestas a la pregunta de la encuesta "Si le faltara el primer molar mandibular, ¿cómo le gustaría restaurarlo?"
por porcentaje del total de encuestados (n=84)
4. Discusión
En comparación con hace 15 años, aunque la educación universitaria en implantología se ha vuelto más completa, todavía existen diferencias en los enfoques educativos entre las distintas instituciones.19–23 Los estudiantes que han recibido una educación predoctoral sólida en implantología tienden a ser más proactivos en el tratamiento con implantes y tienen una mayor probabilidad de incorporarlo en su práctica profesional después de graduarse.24
En nuestra institución, la formación en implantología es obligatoria para todos los estudiantes de pregrado. En el cuarto año, los estudiantes deben asistir a 13 conferencias y 2 ejercicios de simulación computarizada, además de desarrollar un plan de tratamiento con implantes para un caso presentado como un ejercicio de resolución de problemas. En el quinto año, los estudiantes deben participar en prácticas clínicas utilizando modelos de resina con encía artificial. Esta formación práctica incluye incisión gingival, elevación del colgajo, preparación del sitio de colocación del implante, colocación del implante, sutura, cirugía secundaria, conexión del pilar protésico y toma de impresiones (tanto de silicona como ópticas). Los estudiantes reciben capacitación para colocar dos tipos de implantes.
En 2009, se realizó una encuesta antes y después de la formación práctica para investigar la percepción de los estudiantes sobre el tratamiento con implantes.17 Los resultados mostraron que, después de la formación, un número significativamente mayor de estudiantes respondió afirmativamente a la pregunta: "¿Cree que incorporará el tratamiento con implantes en su práctica futura?". Además, cuando se les preguntó si el tratamiento con implantes era más difícil que los tratamientos con puentes o prótesis parciales removibles, un número significativamente mayor de estudiantes respondió "no es difícil" después de la formación, mientras que la proporción de estudiantes que lo consideraban difícil disminuyó significativamente. También, cuando se les preguntó cómo restaurarían un primer molar mandibular ausente, un número significativamente mayor de estudiantes eligió implantes en lugar de puentes después del entrenamiento.17
En la encuesta actual, se observó un aumento significativo en la elección de implantes para la restauración de un primer molar mandibular ausente después de la formación práctica, un hallazgo similar al de 2009. Sin embargo, no se encontraron diferencias significativas en las respuestas a otras preguntas antes y después del entrenamiento. Estas diferencias pueden reflejar el impacto de una educación en implantología más avanzada y completa en nuestra institución desde 2009, impulsada por los avances en tecnología digital. Factores como la mejora de las simulaciones computarizadas en la planificación del tratamiento, la introducción de ejercicios de resolución de problemas y la incorporación de técnicas de impresión óptica con escáneres intraorales podrían haber influido en estos resultados.
Por otro lado, un programa televisivo de NHK en 2012 titulado "Problemas con los implantes dentales: Razones del fuerte aumento", pudo haber generado una impresión negativa sobre los tratamientos con implantes, lo que podría haber afectado la actitud de algunos estudiantes.
A pesar de esto, el aumento significativo en el porcentaje de estudiantes que eligieron el tratamiento con implantes sobre otras alternativas después de la formación práctica sugiere que esta capacitación es efectiva para motivar a los estudiantes a involucrarse en el tratamiento con implantes.
En los últimos años, la adopción de tecnología digital en la práctica odontológica ha avanzado considerablemente, especialmente en el campo de la implantología, donde la tecnología digital se ha integrado relativamente temprano. En la educación odontológica, se están explorando el uso de CAD/CAM para la fabricación de prótesis, simuladores virtuales e incluso la aplicación de inteligencia artificial (IA), con el objetivo de desarrollar sistemas educativos altamente eficaces.25–28
5. Conclusiones
Este estudio resalta el impacto positivo de la formación práctica en implantología sobre la percepción de los estudiantes predoctorales respecto al tratamiento con implantes. Al comparar los resultados con nuestra encuesta previa de 2009, observamos que la formación no solo aumentó la disposición de los estudiantes a incorporar el tratamiento con implantes en su práctica futura, sino que también mejoró su confianza en la realización de procedimientos relacionados con implantes.
A pesar de los avances en la educación en implantología, los hallazgos sugieren que las mejoras continuas en los métodos de formación, especialmente con la integración de tecnología digital, seguirán fortaleciendo la preparación de los estudiantes para brindar atención basada en implantes. Nuestros resultados también subrayan la importancia de la exposición temprana a la implantología en los planes de estudio de odontología, ya que fomenta un mayor compromiso e interés en el tratamiento con implantes entre los futuros profesionales.
De cara al futuro, serán necesarias más investigaciones para analizar cómo estas mejoras educativas influyen en la práctica clínica a largo plazo de los estudiantes y en los resultados de los tratamientos en los pacientes.
6. Declaración de transparencia
Todos los autores declaran no tener conflictos de interés relacionados con esta investigación.
Este trabajo ha contado con el apoyo de una beca de ayuda a la investigación científica (JP24K12976).
Refences
Weintraub AM, Seckinger R, Berthold P, Weintraub GS. Predoctoral Implant dentistry programs in U.S. dental schools. J Prosthodont 1995; 4(2): 116-21.
Seckinger R J, Weintraub A M, Berthold P, Weintraub G S. The status of undergraduate implant education in dental schools outside the United States. Implant Dent 1995; 4(2):105-9.
Bell F A, Hendricson W D. A problem-based course in dental implantology. J Dent Educ 1993; 57(9): 687-95.
Schnitman P A. Education in implant dentistry. J Am Dent Assoc 1990; 121(3): 330-2.
Simons A M, Bell F A, Beirne O R, McGlumphy E A. Undergraduate education in implant dentistry. Implant Dent 1995; 4(1): 40-3.
Ismail J Y. Predoctoral curriculum guidelines in implant dentistry. Int J Oral Implantol. 1990; 7(1): 67-9.
Seckinger R J, Weintraub A M, Berthold P, Weintraub G S. The status of undergraduate implant education in dental schools outside the United States. Implant Dent 1995; 4(2): 105-9.
Addy LD, Lynch CD, Locke M, Watts A, Gilmour AS. The teaching of implant dentistry in undergraduate dental schools in the United Kingdom and Ireland. Br Dent J. 2008 13; 205(11): 609-14.
Blum IR, O'Sullivan DJ, Jagger DC. A survey of undergraduate education in dental implantology in UK dental schools. Eur J Dent Educ. 2008; 12(4): 204-7.
Kronstrom M, McGrath L, Chaytor D. Implant dentistry in the undergraduate dental education program at Dalhousie University. Part 1: clinical outcomes. Int J Prosthodont 2008; 21(2): 124-8.
Petropoulos VC, Arbree NS, Tarnow D, Rethman M, Malmquist J, Valachovic R, Brunson WD, Alfano MC. Teaching implant dentistry in the predoctoral curriculum: a report from the ADEA Implant Workshop's survey of deans. J Dent Educ. 2006; 70(5): 580-8.
Lim MV, Afsharzand Z, Rashedi B, Petropoulos VC. Predoctoral implant education in U.S. dental schools. J Prosthodont. 2005; 14(1): 46-56.
Klokkevold PR. Implant education in the dental curriculum. J Calif Dent Assoc. 2001; 29(11): 747-55.
Wilcox C W, Huebner G R, Mattson J S, Nilsson D E, Blankenau R J. Placement and restoration of implants by predoctoral students: the Creighton experience. J Prosthodont 1997; 6(1): 61-5.
Maalhagh-Fard A, Nimmo A, Lepczyk JW, Pink FE. Implant dentistry in predoctoral education: the elective approach. J Prosthodont. 2002; 11(3): 202-7.
Kido H, Yamamoto K, Kakura K, Morinaga K, Matsuura T, Matsunaga T, Shimizu H, Takahashi Y, Sato H, Matsuura M. Students' opinion of a predoctoral implant training program. J Dent Educ. 2009; 73(11): 1279-85.
Muddugangadhar BC, Amarnath GS, Sonika R, Chheda PS, Garg A. Meta-analysis of Failure and Survival Rate of Implant-supported Single Crowns, Fixed Partial Denture, and Implant Tooth-supported Prostheses. J Int Oral Health. 2015 ; 7(9): 11-7.
Hare A, Bird S, Wright S, Ucer C, Khan RS. Current Undergraduate Dental Implantology Teaching in UK. Dent J (Basel). 2022; 10(7): 127. doi: 10.3390/dj10070127.
Seitz SD, Zimmermann RL, Hendricson WD. Expansion of a Predoctoral Surgical Implant Selective for Dental Students. J Dent Educ. 2016; 80(3): 328-33.
Prasad S, Bansal N. Predoctoral Dental Students' Perceptions of Dental Implant Training: Effect of Preclinical Simulation and Clinical Experience. J Dent Educ. 2017; 81(4): 395-403.
Missinne K, Duyck J, Naert I, Quirynen M, Bertrand S, Vandamme K. Oral Implant Restorations By Undergraduate Students: An Up To 5-Years Clinical Outcome. Int J Prosthodont. 2021; 34(4): 433–440.
Schweyen R, Al-Nawas B, Arnold C, Hey J. A cross-sectional survey of attitudes towards education in implant dentistry in the undergraduate dental curriculum. Int J Implant Dent. 2020 8; 6(1): 26.
Kattadiyil MT, Jekki R, Goodacre CJ, Baba NZ. Comparison of treatment outcomes in digital and conventional complete removable dental prosthesis fabrications in a predoctoral setting. J Prosthet Dent. 2015; 114(6): 818-25.
Huang Y, Hu Y, Chan U, Lai P, Sun Y, Dai J, Cheng X, Yang X. Student perceptions toward virtual reality training in dental implant education. PeerJ. 2023;11:e14857. doi: 10.7717/peerj.14857. eCollection 2023.
Fang Q, Reynaldi R, Araminta AS, Kamal I, Saini P, Afshari FS, Tan SC, Yuan JC, Qomariyah NN, Sukotjo C. Artificial Intelligence (AI)-driven dental education: Exploring the role of chatbots in a clinical learning environment. J Prosthet Dent. 2024: S0022-3913(24)00231-2. doi: 10.1016/j.prosdent.2024.03.038. Online ahead of print.
Surlari Z, Budală DG, Lupu CI, Stelea CG, Butnaru OM, Luchian I. Current Progress and Challenges of Using Artificial Intelligence in Clinical Dentistry-A Narrative Review. J Clin Med 2023; 12(23): 7378. doi: 10.3390/jcm12237378.