1) The Nippon Dental University, School of Life Dentistry, Department of Periodontology
2) Sugita Dental Clinica
3) Wada Dental Clinic
4) Meikai University School of Dentistry, Division of Dental Biomaterials Science, Department of Restorative and Biomaterials Sciences
5) Heartful Dental Clinic
6) Aoba Dental Clinic
7) Matsumoto dental university department of Dental science and material
8) Mieji Dental Clinic
9) Iryo Hojin Shikyoukai, Yabuki Dental Clinic
10) Fukuda Dental Clinic
COI: There are no conflicts of interest to disclose regarding this paper.
All subjects have given their consent for the publication of this paper.
Abstract
This study investigated the risk associated with residual angular bony defects following active periodontal therapy, specifically their impact on the progression of periodontitis and tooth loss. The study analyzed data from 24 patients diagnosed with generalized or localized periodontitis (Stage III or higher) across 64 sites, with an average maintenance period of 116.6 months. A comparative analysis between sites with angular bony defects (experimental group) and those with horizontal bone resorption (control group) revealed no statistically significant differences in the progression of bone resorption or disease exacerbation. Radiographic assessments also demonstrated no significant differences in bone resorption volume between the two groups.
Among the factors influencing disease progression, plaque accumulation was identified as a statistically significant risk factor. In contrast, bone defect morphology, probing pocket depth (PPD ≥5 mm), and the presence or absence of the lamina dura were not significantly correlated with disease progression.
These findings suggest that, even in the presence of angular bony defects, long-term periodontal maintenance can effectively mitigate disease progression to a level comparable to that of horizontal bone resorption sites. This underscores the critical role of plaque control in post-periodontal treatment management, rather than bone defect morphology itself.
This study provides a re-evaluation of the clinical implications of angular bony defects in long-term periodontal care and offers new insights for periodontal maintenance strategies.
Key words:Wedge-shaped bone defect, periodontal maintenance, prognosis, bone resorption, tooth loss
I. Introduction
Periodontitis is a chronic, progressive disease primarily caused by biofilm, leading to attachment loss and alveolar bone resorption as it progresses. While the pattern of bone resorption varies depending on individual conditions, in many cases, the location of plaque is believed to be closely related to alveolar bone loss.1 Bone resorption is generally classified into angular (vertical) and horizontal types, with angular bony defects often being a significant clinical concern.2,3
The fundamental approach to treating periodontitis with wedge-shaped bone defects is biofilm removal, and improvement through non-surgical periodontal therapy has been reported.4,5 Additionally, periodontal surgical procedures have been shown to induce an average bone gain of 1.5 mm.6 Furthermore, regenerative periodontal therapy has been found to be particularly effective in cases where bone defects exceed 3 mm in depth, with reports of long-term favorable outcomes.7 However, even after periodontal treatment, bone defects do not always become completely flattened, and residual wedge-shaped defects are frequently observed post-treatment.8
Radiographic studies conducted during maintenance therapy following active periodontal treatment have suggested that angular bony defects do not act as a significant risk factor.8,9 On the other hand, clinical studies incorporating both radiographic and clinical evaluations have reported that angular bony defects show greater progression of bone resorption compared to horizontal bone loss, particularly when the lamina dura is absent, indicating a higher risk.3
Since previous studies have yielded inconsistent results, further long-term, high-quality studies are necessary to clarify the impact of residual angular boney defects on periodontal disease progression. Therefore, this study aims to analyze the risk posed by residual angular bony defects after active periodontal therapy in relation to progression of periodontitis and tooth loss.
II. Subjects and Methods
This retrospective study was conducted with the approval of the Ethics Committee of The Academy of Clinical Dentistry. The study included patients diagnosed with generalized or localized periodontitis at Stage 3 or higher, who had completed active periodontal therapy and continued supportive periodontal therapy (SPT) for at least five years at eight dental institutions between January 2010 and December 2023.
From the medical records of these patients, clinical parameters, patient information, and radiographic images were collected for analysis. The eligibility and exclusion criteria for this study were as follows.
Eligibility Criteria:
Age between 25 and 75 years at the start of supportive periodontal therapy (SPT).
Presence of at least 20 remaining teeth after active periodontal therapy.
Availability of periodontal examination results and radiographic images (intraoral or panoramic) at the time of SPT following active treatment.
Presence of angular bony defects identified during reevaluation after active treatment.
Eligibility Criteria:
Presence of restorations or orthodontic appliances that may affect treatment outcomes or radiographic analysis.
Persistent or progressively enlarging periapical lesions by the final examination.
Lack of available periodontal examination results and radiographic images.
Unavailability of periodontal examination results after initial treatment.
Lesions influenced by impacted third molars.
Teeth extracted before reevaluation after active treatment.
Tooth surfaces with furcation involvement.
All periodontal examinations were conducted using a full-mouth and six-sites per tooth, recording probing pocket depth (PPD) and the presence or absence of bleeding on probing (BOP). The presence of plaque was recorded on four surfaces per tooth.
Data Recorded from Medical Records:
The following information was extracted from the medical records:
Age
Sex
Number of remaining teeth at baseline (BL, after completion of active treatment) and at final examination (FE, during maintenance/SPT)
Full-mouth plaque score from BL to FE
Bleeding on probing (BOP%) from BL to FE
Percentage of sites with probing pocket depth (PPD) ≥ 4 mm from BL to FE
Smoking status
Medical history (systemic conditions)
Annual frequency of SPT visits
Other notable findings
From this dataset, patients and sites that met the eligibility criteria were selected. Based on periodontal examination and radiographic findings at reevaluation after active treatment, they were categorized into the following groups.
Experimental Group
Sites where a angular bony (vertical) defect of 2 mm or more was observed on the interproximal surfaces in radiographic images.
Control Group
Sites with horizontal bone loss observed on the smooth surface of the contralateral, adjacent, or similar tooth in the same patient.
Radiographic Image Analysis
Dental radiographs (periapical or panoramic) taken at baseline (BL) and final examination (FE) using the apical projection technique were used for measurements. All radiographic images were digitized, imported into a computer, and analyzed at maximum magnification on the screen.
In the experimental group, the root length was measured as the distance from the cementoenamel junction (CEJ) to the root apex. Bone loss was quantified by measuring the distance from the CEJ to the bottom of the bone defect. The depth of the bone defect was measured from the alveolar crest to the bottom of the defect. Similarly, in the control group, root length and bone loss were measured using the same methodology. To standardize the data, all measurements were adjusted based on the average root length of 10 mm for Japanese individuals.10
The presence of the lamina dura (LD) at the interdental alveolar crest were assessed. The LD was considered intact if it appeared as a continuous radiopaque white line without interruptions along the superior and inferior margins.
Data Analysis
The mean values or frequencies of each clinical parameter from baseline (BL) to final examination (FE) were calculated.
Probing pocket depth (PPD):
Differences between the experimental and control groups, as well as changes from BL to FE within each group, were analyzed using a paired t-test.
The difference in the mean change from BL to FE between groups was also analyzed using a paired t-test.
Bleeding on probing (BOP) and plaque presence:
Differences between and within groups were analyzed using a chi-square test.
Radiographic analysis:
In the experimental group, changes in bone loss (mm) and bone defect depth (mm) from BL to FE were analyzed using a paired t-test.
In the control group, changes in bone defect depth from BL to FE were also analyzed using a paired t-test.
Additionally, bone loss at BL and FE, as well as the difference in bone loss progression between the experimental and control groups, was analyzed using a paired t-test.
The presence or absence of the lamina dura was analyzed using a chi-square test for both within-group and between-group differences.
Assessment of periodontal disease progression:
The number of lost teeth and the progression of bone resorption (categorized as ≥0.5 mm, ≥1.0 mm, and ≥1.5 mm) were analyzed using a chi-square test to assess differences between groups. To identify factors associated with progression of bone loss, a multivariable logistic regression analysis was performed, using risk factors as explanatory variables and periodontal disease progression as the dependent variable.
III. Results
A total of 64 sites from 24 patients who met the inclusion criteria were analyzed in this study. The duration of supportive periodontal therapy (SPT) from baseline (BL) to final examination (FE) ranged from 60 to 215 months (mean 116.6 months). One tooth loss was observed in the experimental group, and this tooth was excluded from the calculation of mean clinical parameters and radiographic measurements but was included in the analysis of periodontal disease progression.
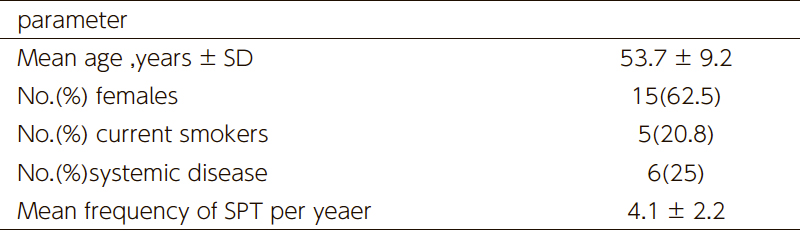
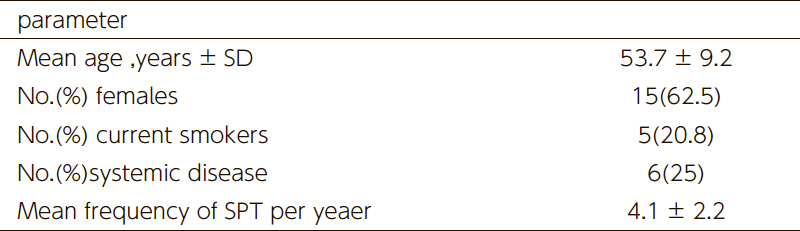
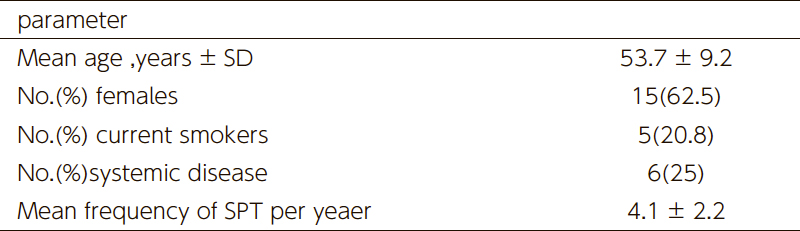
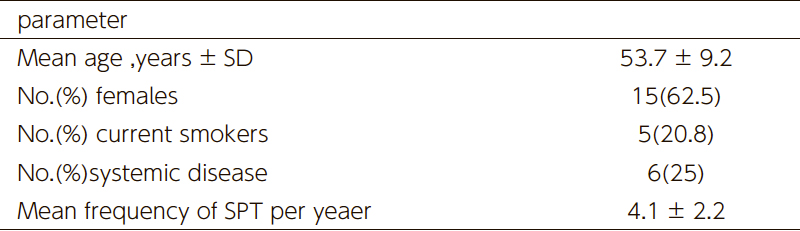
As shown in Table 1, the patient characteristics at BL (completion of active periodontal therapy) were summarized. The longitudinal changes in full-mouth clinical parameters are presented in Table 2. No significant changes were observed in the mean plaque score, bleeding on probing (BOP), or the proportion of sites with probing pocket depth (PPD) ≥4 mm. However, the number of lost teeth showed a statistically significant reduction.
(Table 1) Demographic and clinical parameters of study patiens at baseline.(Table 2) Clinical parameter at baseline(BL) and final examinations(FE)
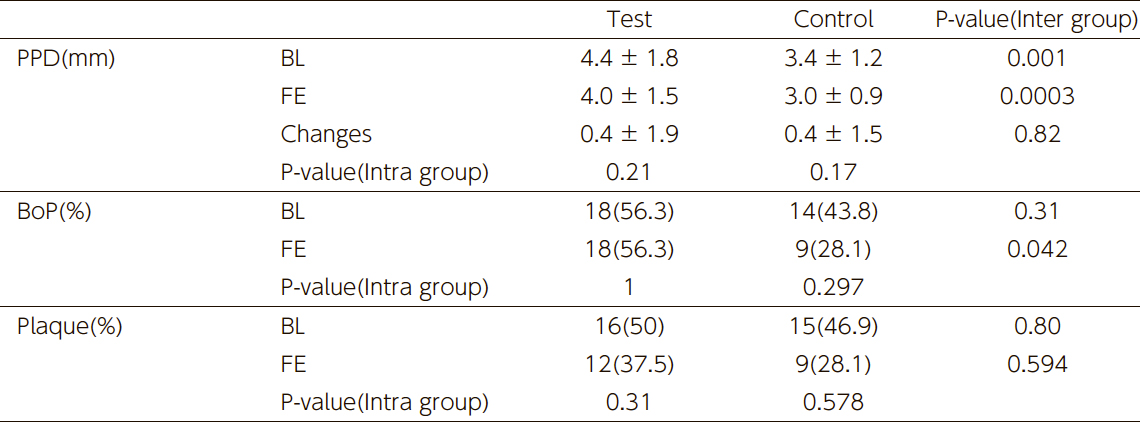
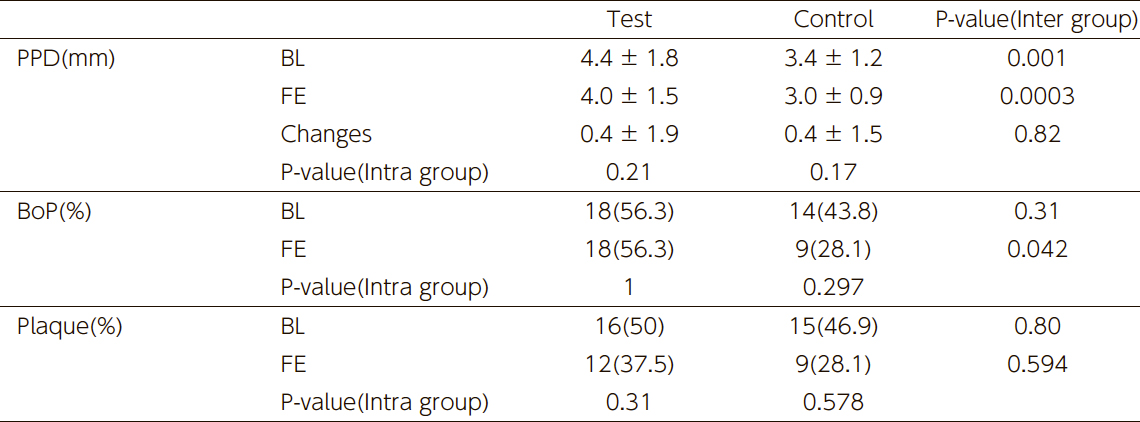
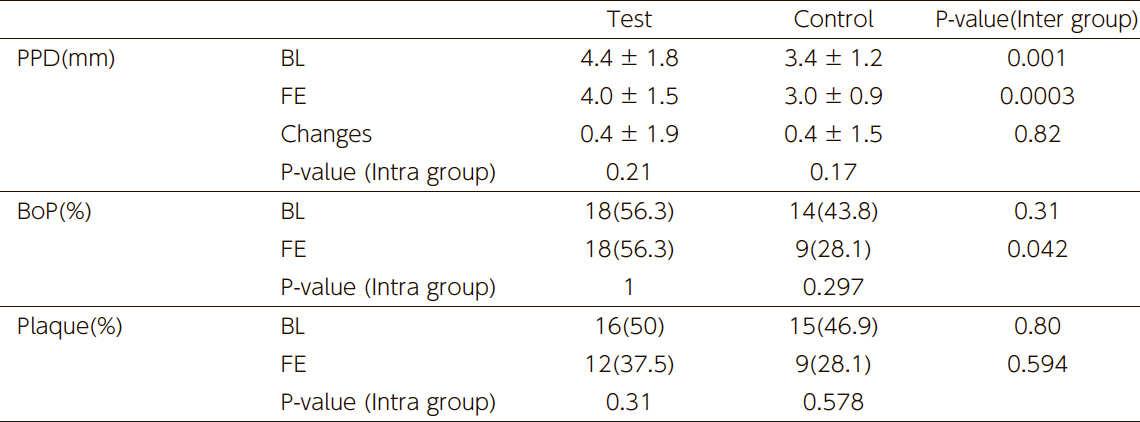
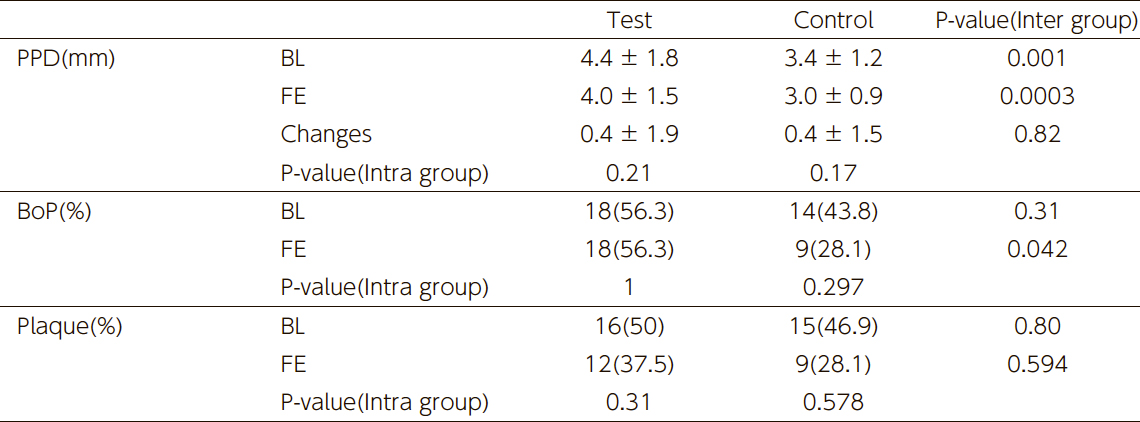
Table 3 presents the longitudinal changes in clinical parameters for the experimental and control groups. The mean PPD at both BL and FE was significantly higher in the experimental group than in the control group. However, the change in PPD from BL to FE did not show a significant difference between groups. Regarding BOP, the experimental group showed a significantly higher BOP at FE than the control group, but the within-group change from BL to FE was not statistically significant. The number of plaque-affected surfaces did not show significant differences between or within groups.
(Table 3) Clinical parameters at baseline and final examination on the study tooth site
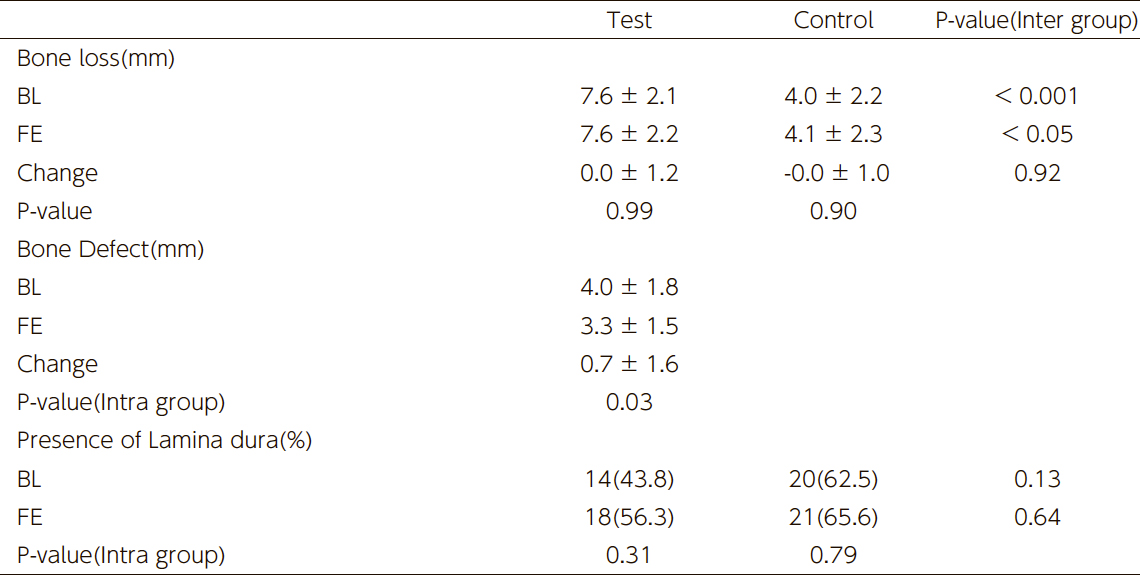
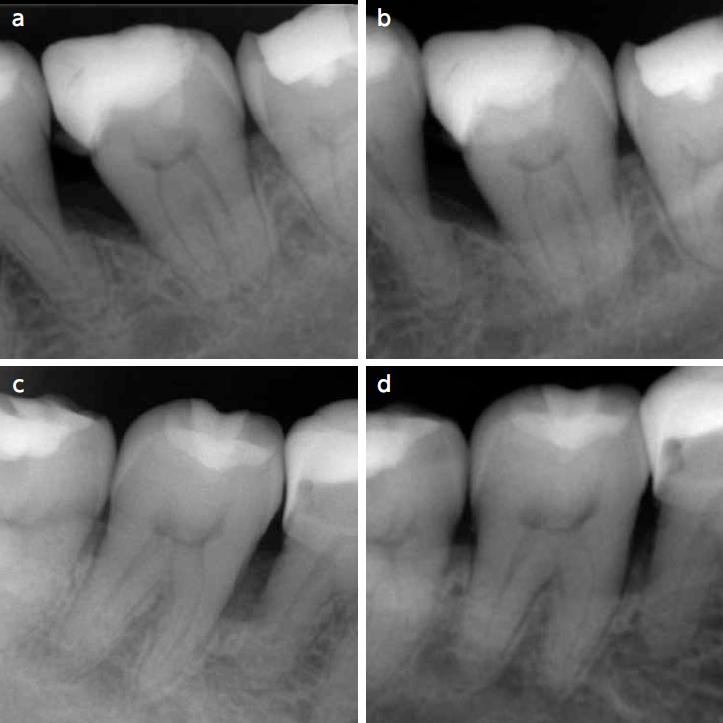
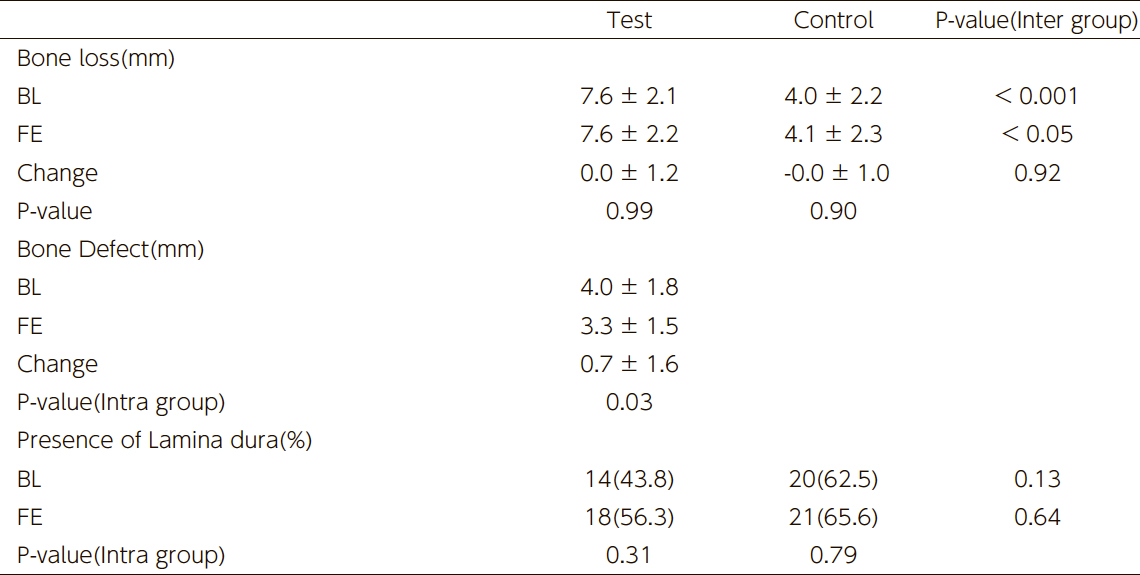
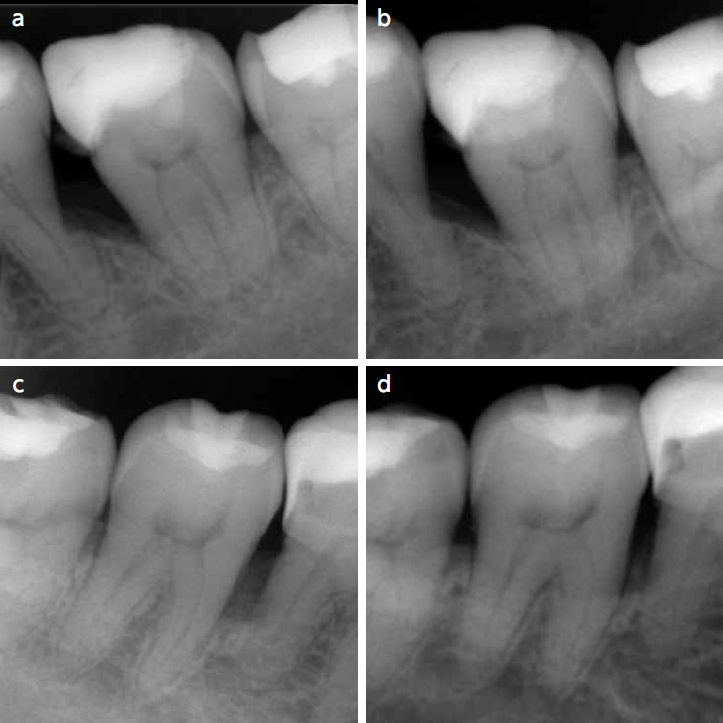
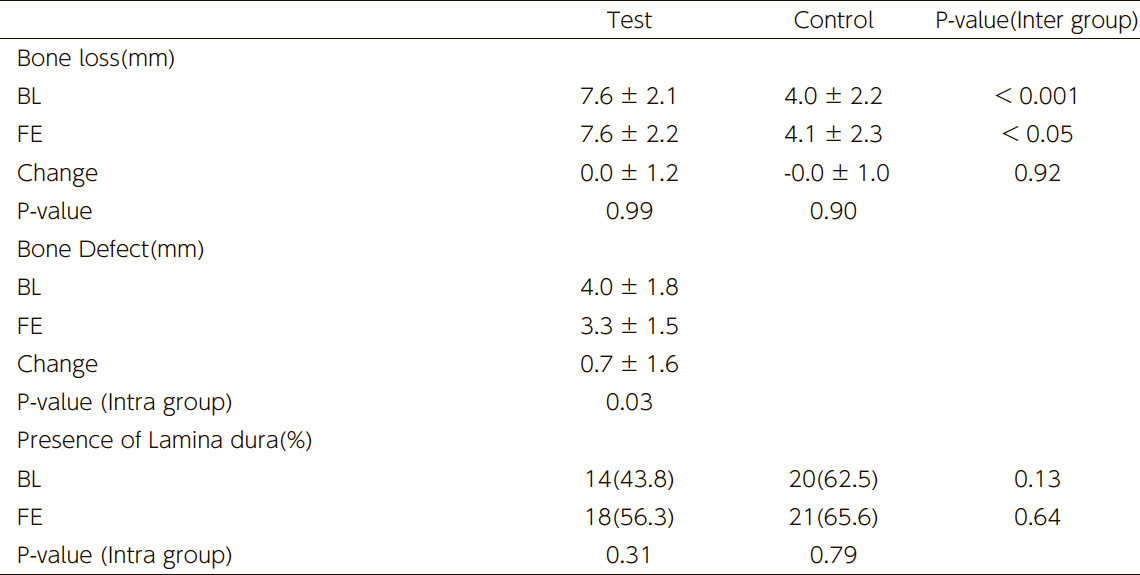
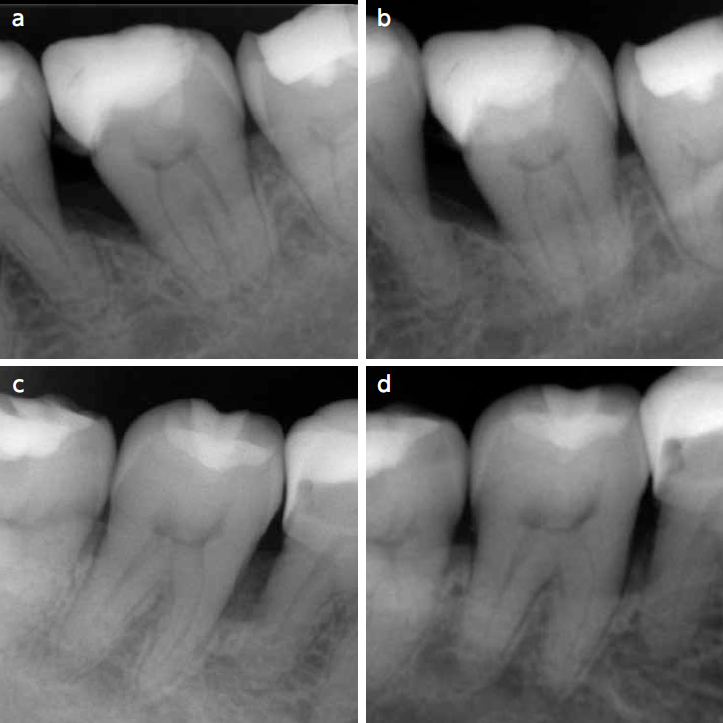
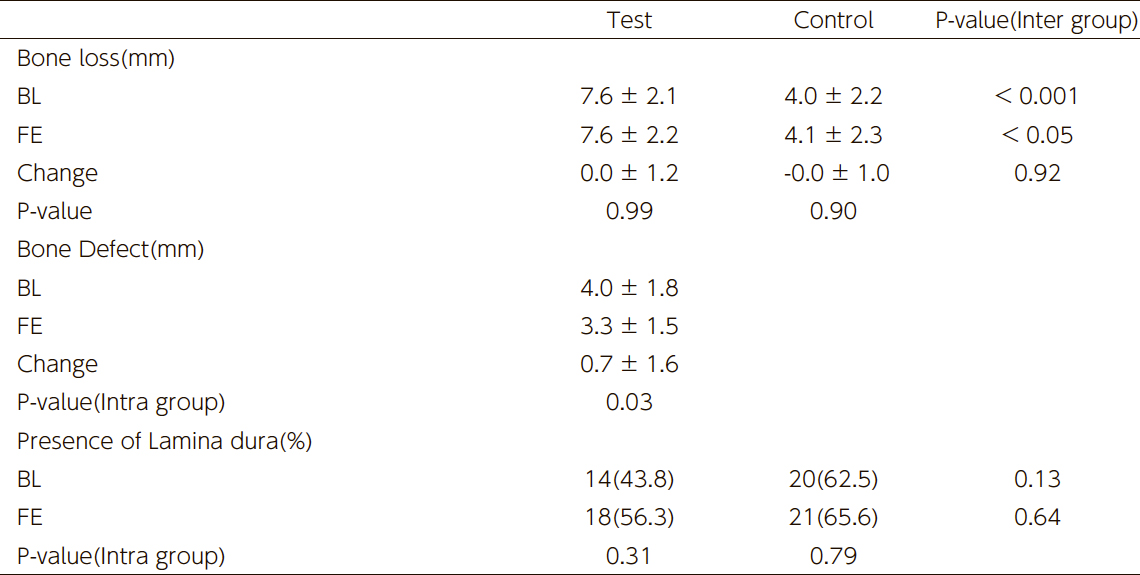
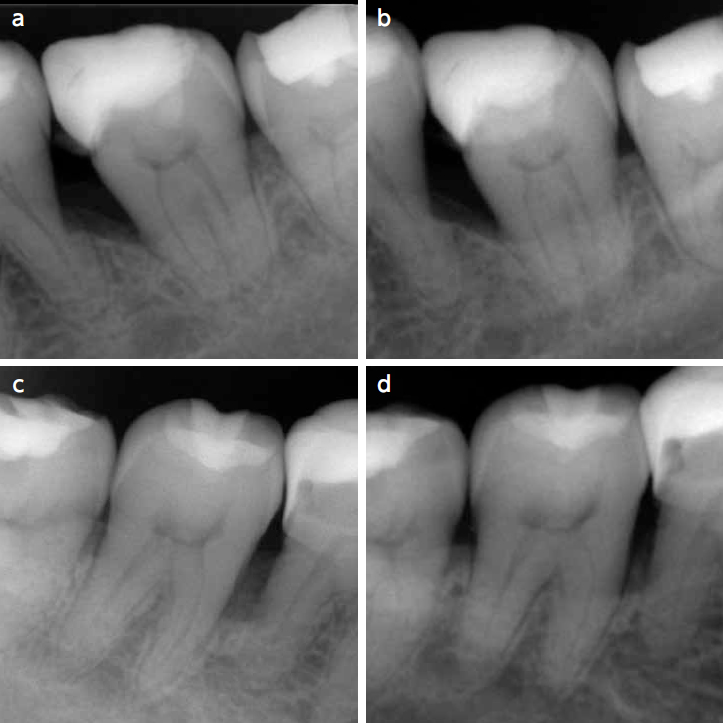
The radiographic analysis results are presented in Table 4. The amount of bone loss at both BL and FE was significantly greater in the experimental group compared to the control group. However, the change in bone loss from BL to FE did not show a significant difference between groups. On the other hand, the depth of bone defects in the experimental group significantly decreased from BL to FE. No statistically significant differences were observed in the presence of the lamina dura either within or between groups. Fig.1 illustrates a representative case.
(Table 4) Radiographic measurements at baseline and final examination(Fig.1)
a) Mesial surface of first molar with an angular bony defect present after active therapy
b) The same sites 9 years later
c) mesial site site second moler with an even outline of the alveolar bone after active therapy
d) The same sites 9 years later
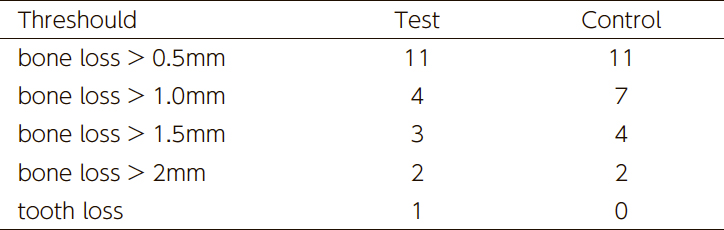
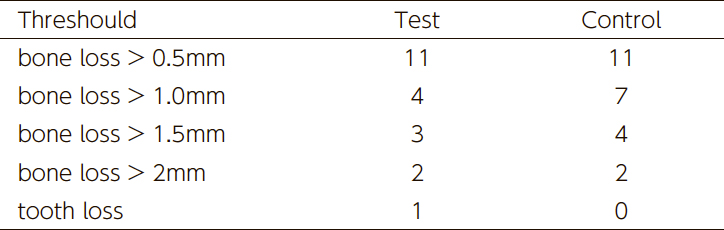
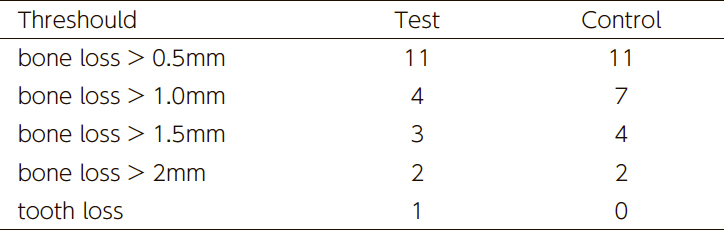
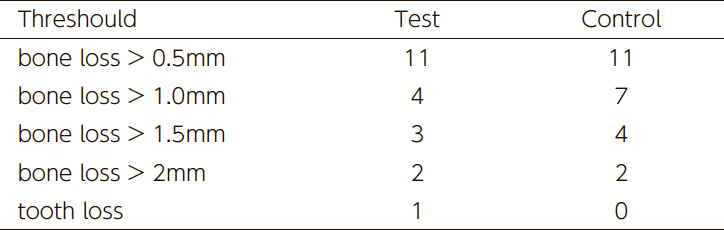
The number of "disease progression sites" is presented in Table 5. When including the single case of tooth loss in the experimental group, the progression of bone loss was analyzed at three thresholds (>0.5 mm, >1.0 mm, >1.5 mm). No significant differences in disease progression were observed between groups at any threshold.
(Table 5) Number of disease progression at each threshold level
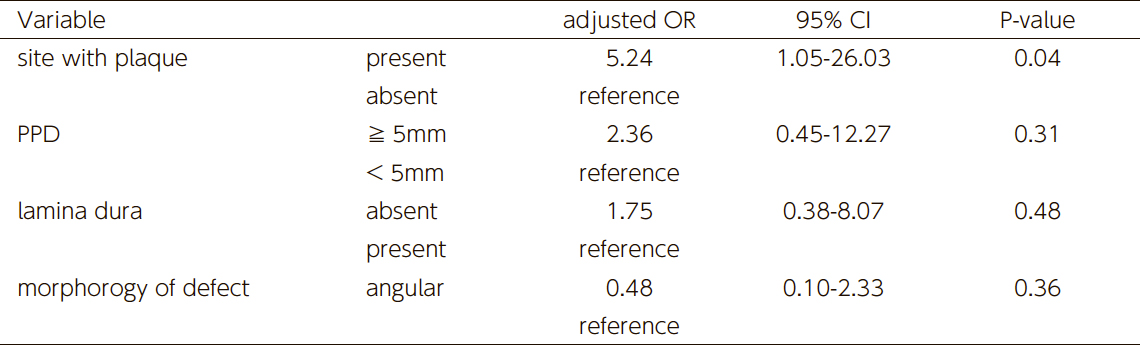
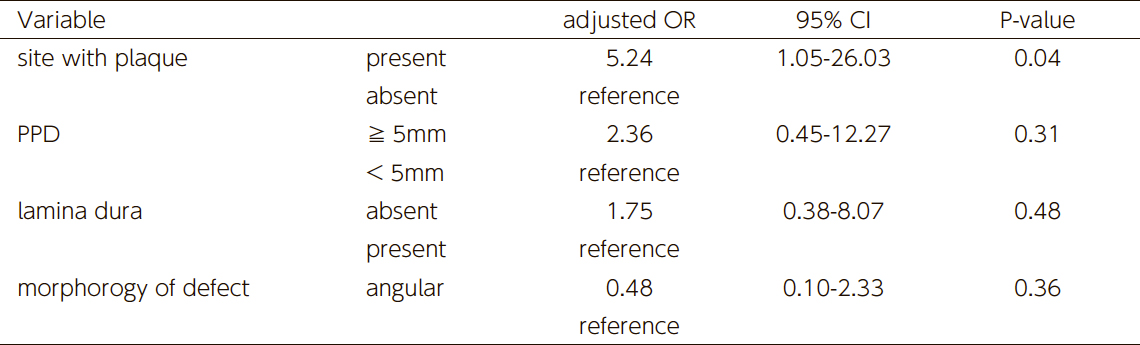
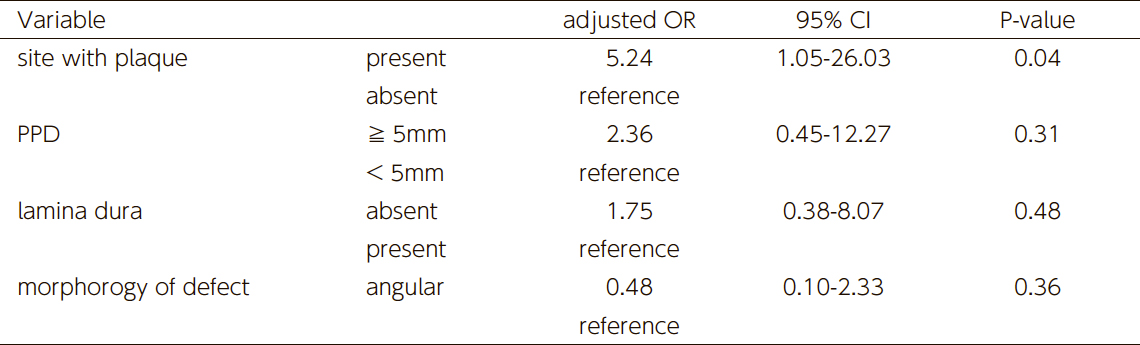
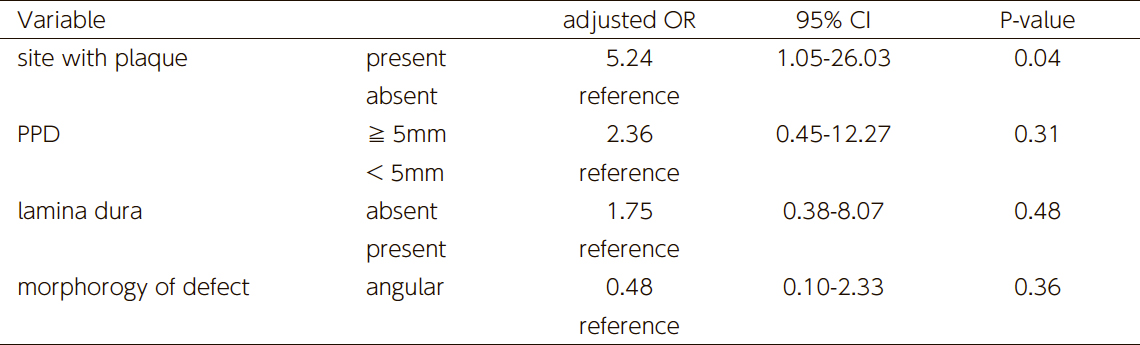
The results of the multivariable logistic regression analysis are shown in Table 6. When disease progression was defined as bone loss exceeding 1 mm or tooth loss, plaque accumulation was identified as a significant independent risk factor (adjusted odds ratio: 2.36, p < 0.05). In contrast, PPD ≥5 mm, bone morphology (angular vs. horizontal), and the presence or absence of the lamina dura did not show statistical significance.
(Table 6) The resut of multivariate logistic regression analysis for disease progression (adjusted by years of SPT and smoking status)
IV. Discussion
The results of this study indicate that angular boney defects identified at reevaluation after active periodontal therapy did not exhibit a significantly greater progression of bone resorption compared to sites with horizontal bone loss, provided that patients continued maintenance therapy at an annual average frequency of 4.1 ± 2.2 times per year. Specifically, no significant differences were observed in the amount of bone loss measured on radiographs or in the proportion of sites that worsened during the observation period between angular boney defects and horizontal bone loss sites.
This finding is consistent with the long-term studies by Greenstein8 et al. and Pontoriero9 et al., as well as the animal study by Magnusson11 et al., which demonstrated no difference in the length of the junctional epithelium or resistance to periodontitis.
On the other hand, the results of this study differ from previous reports suggesting that angular boney defects exhibit greater progression of bone loss than horizontal bone loss sites. For instance, Papapanou2 et al. conducted a retrospective study analyzing 201 panoramic radiographs over a 10-year period, reporting that sites with angular boney defects exhibited significantly greater bone resorption (>2 mm) and had a higher incidence of tooth loss in deeper defects. However, this study did not account for post-baseline treatment, and it is likely that many patients did not receive comprehensive periodontal therapy. Thus, the study population differs from our cohort, where patients continued maintenance therapy for 5–17 years.
Similarly, Rams3 et al. conducted a prospective 36-month study and found that angular boney defects were significantly more likely to deteriorate than horizontal bone loss sites. However, their study had a shorter observation period and did not include an analysis of tooth loss, making it different from the present study. Additionally, Rams3 et al. reported that when an angular boney defect was accompanied by the presence of the lamina dura, the rate of disease progression was lower. The presence of the lamina dura is believed to be associated with the resolution of inflammation and the stabilization of periodontal tissues; however, in our study, no such correlation was observed. This discrepancy may be attributed to differences in radiographic standardization methods.
Regarding tooth loss, one case of tooth extraction was observed in the angular boney defect group, whereas no teeth were lost in the horizontal bone loss group. However, the extracted tooth exhibited a PPD of 9 mm with BOP at baseline after active periodontal therapy (data not presented), suggesting that periodontal treatment was unsuccessful in this case. Larger-scale studies analyzing tooth loss as an endpoint may yield different results.
The presence of angular boney defects is often considered a sign of occlusal trauma.12 However, in this study, none of the evaluated teeth exhibited mobility at BL, nor did they show progressive mobility during the observation period. Recent consensus reports state that pathological conditions related to secondary occlusal trauma are characterized by progressive tooth mobility. Therefore, in this study, no association between angular boney defects and occlusal trauma was observed.
In this study, the plaque adherence frequency at BL was approximately 50% in both groups. While there was a trend toward improvement by the final examination (FE), no statistically significant difference was observed. As a result, the control group showed a tendency for reduced BOP frequency, whereas the experimental group remained unchanged. At FE, the BOP frequency was significantly lower in the control group compared to the experimental group, which is likely attributable to morphological differences.
Despite the completion of active treatment, the mean PPD at BL was larger in the experimental group than in the control group. Similarly, the mean bone loss in the experimental group was significantly greater than in the control group at BL, aligning with the PPD findings. However, despite these differences, no significant intergroup differences were observed in longitudinal bone resorption progression or worsening of clinical parameters, indicating stable outcomes in both groups. Therefore, the higher PPD and BOP observed in the experimental group during the study period do not necessarily indicate a pathological condition, though longer-term observation is warranted.
This study calculated bone loss based on root length measurements from radiographic images, adjusted to the average root length of Japanese individuals. When measurements are conducted on non-standardized radiographs, as in this study, bone loss is often evaluated using proportional methods such as grids. However, proportional measurements may underestimate bone resorption in teeth with relatively longer roots, such as canines. Expressing bone loss in absolute values rather than proportions provides a more clinically relevant assessment. However, adjusting measurements to the Japanese average root length does not account for individual variations, which is a limitation of retrospective studies. Future prospective studies using standardized radiographic imaging are necessary to improve accuracy.
In this study, disease progression was defined as "tooth loss + progression of bone loss," and multivariable logistic regression analysis was performed. The results showed no correlation between alveolar bone resorption patterns and disease progression; however, plaque accumulation was significantly associated with disease progression. Additionally, while the presence of pockets >5 mm did not reach statistical significance, the odds ratio was 2.3. This suggests that in patients undergoing long-term maintenance therapy, oral hygiene status and periodontal clinical parameters may contribute more significantly to periodontitis progression than bone defect morphology.
V. Conclusion
This study demonstrated that even in cases where angular boney defects persist after active periodontal therapy, long-term maintenance therapy can prevent significant differences in the risk of periodontitis progression compared to sites with horizontal bone loss. Furthermore, multivariable analysis identified plaque accumulation as the most significant risk factor for periodontitis progression, whereas bone defect morphology, probing pocket depth (PPD ≥5 mm), and the presence or absence of the lamina dura did not reach statistical significance.
These findings suggest that in post-periodontal therapy maintenance, effective plaque control is more critical for preventing periodontitis progression than the presence of wedge-shaped bone defects. This study provides a reassessment of the clinical implications of angular boney defects and offers guidance for long-term periodontal management after treatment.
References:
Waerhaug, J. The angular bone defect and its relationship to trauma from occlusion and downgrowth of subgingival plaque. J Clin Periodontol. April 1979; 6(2):61-82. doi:10.1111/j.1600-051x.1979.tb02185.x.
Papapanou, P.N., & Wennström, J.L. The angular bony defect as indicator of further alveolar bone loss. J Clin Periodontol. May 1991; 18(5):317-22. doi:10.1111/j.1600-051x.1991.tb00435.x.
Rams, T.E., Listgarten, M.A., & Slots, J. Radiographic alveolar bone morphology and progressive periodontitis. J Periodontol. April 2018; 89(4):424-430. doi:10.1002/JPER.17-0279.
Ehnevid, H., Jansson, L., Lindskog, S., & Blomlöf, L. Periodontal healing in horizontal and vertical defects following surgical or non-surgical therapy. Swed Dent J. 1997; 21(4):137-47.
Nibali, L., Pometti, D., Tu, Y.K., & Donos, N. Clinical and radiographic outcomes following non-surgical therapy of periodontal infrabony defects: A retrospective study. J Clin Periodontol. 2011; 38:50–57. doi:10.1111/j.1600-051X.2010.01648.x.
Lang, N.P. Focus on intrabony defects—conservative therapy. Periodontol 2000. February 2000; 22:51-8. doi:10.1034/j.1600-0757.2000.2220105.x.
Cortellini, P., Buti, J., Pini Prato, G., & Tonetti, M.S. Periodontal regeneration compared with access flap surgery in human intra-bony defects 20-year follow-up of a randomized clinical trial: Tooth retention, periodontitis recurrence and costs. J Clin Periodontol. January 2017; 44(1):58-66. doi:10.1111/jcpe.12638.
Greenstein, B., Frantz, B., Desai, R., Proskin, H., Campbell, J., & Caton, J. Stability of treated angular and horizontal bony defects: A retrospective radiographic evaluation in private periodontal practice. J Periodontol. 2009 Feb;80(2):228-33.doi: 10.1902/jop.2009.080158
Pontoriero, R., Nyman, S., & Lindhe, J. The angular bony defect in the maintenance of the periodontal patient. J Clin Periodontol. March 1988; 15(3):200-4. doi:10.1111/j.1600-051x.1988.tb01570.x.
Magnusson, I., Runstad, L., Nyman, S., & Lindhe, J. J Clin Periodontol. May 1983; 10(3):333-40. doi:10.1111/j.1600-051x.1983.tb01282.x.
Glickman, I. Clinical significance of trauma from occlusion. J Am Dent Assoc. March 1965; 70:607-18. doi:10.14219/jada.archive.1965.0261.
Fan, J., & Caton, J.G. Occlusal trauma and excessive occlusal forces: Narrative review, case definitions, and diagnostic considerations. J Clin Periodontol. June 2018; 45(Suppl 20):S199-S206. doi:10.1111/jcpe.12949.
Jepsen, S., Caton, J.G., Albandar, J.M., et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. June 2018; 45(Suppl 20):S219-S229. doi:10.1111/jcpe.12951.
1) The Nippon Dental University, School of Life Dentistry, Department of Periodontology
2) Sugita Dental Clinica
3) Wada Dental Clinic
4) Meikai University School of Dentistry, Division of Dental Biomaterials Science, Department of Restorative and Biomaterials Sciences
5) Heartful Dental Clinic
6) Aoba Dental Clinic
7) Matsumoto dental university department of Dental science and material
8) Mieji Dental Clinic
9) Iryo Hojin Shikyoukai, Yabuki Dental Clinic
10) Fukuda Dental Clinic
COI: There are no conflicts of interest to disclose regarding this paper.
All subjects have given their consent for the publication of this paper.
本回顾性研究已获得日本顎咬合学会(The Academy of Clinical Dentistry)伦理委员会的批准。研究对象为诊断为广泛性或局限性牙周炎(第3期或以上)的患者,这些患者在2010年1月至2023年12月期间,于8家牙科医疗机构接受了活动性牙周治疗,并持续进行至少5年的支持性牙周治疗(SPT)。
(表4)Radiographic measurements at baseline and final examination(图1)
a) Mesial surface of first molar with an angular bony defect present after active therapy
b) The same sites 9 years later
c) mesial site site second moler with an even outline of the alveolar bone after active therapy
d) The same sites 9 years later
该结果与Greenstein et al.8 和Pontoriero et al.9 的长期研究一致,同时也与Magnusson et al.11 的动物实验结果相符,后者表明接合上皮的长度及对牙周炎的抵抗力无显著差异。
另一方面,本研究的结果与先前研究所报道的“楔形骨缺损较水平性骨吸收部位具有更大骨吸收进展”的观点不一致。例如,Papapanou et al.2 进行了一项回顾性研究,分析了201例全景X线片,观察期长达10年,结果显示楔形骨缺损部位的骨吸收显著增加(>2mm),且深度较大的缺损更易发生牙齿丧失。然而,该研究未考虑基线后的治疗情况,且许多患者可能未接受全面的牙周治疗。因此,与本研究相比,该研究的患者群体存在差异,而本研究的患者均持续接受5–17年的牙周维护治疗。
同样,Rams et al.3 进行了一项为期36个月的前瞻性研究,发现楔形骨缺损的病变恶化风险显著高于水平性骨吸收部位。然而,该研究的观察期较短,且未纳入牙齿丧失的分析,因此与本研究存在差异。此外,Rams et al.3 e指出,当楔形骨缺损伴随牙槽硬线(lamina dura)存在时,其疾病进展速率较低。牙槽硬线的存在被认为与炎症的消退及牙周组织的稳定相关,但在本研究中,未观察到这种相关性。这种差异可能与影像学标准化方法的不同有关。
Waerhaug, J. The angular bone defect and its relationship to trauma from occlusion and downgrowth of subgingival plaque. J Clin Periodontol. April 1979; 6(2):61-82. doi:10.1111/j.1600-051x.1979.tb02185.x.
Papapanou, P.N., & Wennström, J.L. The angular bony defect as indicator of further alveolar bone loss. J Clin Periodontol. May 1991; 18(5):317-22. doi:10.1111/j.1600-051x.1991.tb00435.x.
Rams, T.E., Listgarten, M.A., & Slots, J. Radiographic alveolar bone morphology and progressive periodontitis. J Periodontol. April 2018; 89(4):424-430. doi:10.1002/JPER.17-0279.
Ehnevid, H., Jansson, L., Lindskog, S., & Blomlöf, L. Periodontal healing in horizontal and vertical defects following surgical or non-surgical therapy. Swed Dent J. 1997; 21(4):137-47.
Nibali, L., Pometti, D., Tu, Y.K., & Donos, N. Clinical and radiographic outcomes following non-surgical therapy of periodontal infrabony defects: A retrospective study. J Clin Periodontol. 2011; 38:50–57. doi:10.1111/j.1600-051X.2010.01648.x.
Lang, N.P. Focus on intrabony defects—conservative therapy. Periodontol 2000. February 2000; 22:51-8. doi:10.1034/j.1600-0757.2000.2220105.x.
Cortellini, P., Buti, J., Pini Prato, G., & Tonetti, M.S. Periodontal regeneration compared with access flap surgery in human intra-bony defects 20-year follow-up of a randomized clinical trial: Tooth retention, periodontitis recurrence and costs. J Clin Periodontol. January 2017; 44(1):58-66. doi:10.1111/jcpe.12638.
Greenstein, B., Frantz, B., Desai, R., Proskin, H., Campbell, J., & Caton, J. Stability of treated angular and horizontal bony defects: A retrospective radiographic evaluation in private periodontal practice. J Periodontol. 2009 Feb;80(2):228-33.doi: 10.1902/jop.2009.080158
Pontoriero, R., Nyman, S., & Lindhe, J. The angular bony defect in the maintenance of the periodontal patient. J Clin Periodontol. March 1988; 15(3):200-4. doi:10.1111/j.1600-051x.1988.tb01570.x.
Magnusson, I., Runstad, L., Nyman, S., & Lindhe, J. J Clin Periodontol. May 1983; 10(3):333-40. doi:10.1111/j.1600-051x.1983.tb01282.x.
Glickman, I. Clinical significance of trauma from occlusion. J Am Dent Assoc. March 1965; 70:607-18. doi:10.14219/jada.archive.1965.0261.
Fan, J., & Caton, J.G. Occlusal trauma and excessive occlusal forces: Narrative review, case definitions, and diagnostic considerations. J Clin Periodontol. June 2018; 45(Suppl 20):S199-S206. doi:10.1111/jcpe.12949.
Jepsen, S., Caton, J.G., Albandar, J.M., et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. June 2018; 45(Suppl 20):S219-S229. doi:10.1111/jcpe.12951.
COI: There are no conflicts of interest to disclose regarding this paper.
All subjects have given their consent for the publication of this paper.
1) The Nippon Dental University, School of Life Dentistry, Department of Periodontology
2) Sugita Dental Clinica
3) Wada Dental Clinic
4) Meikai University School of Dentistry, Division of Dental Biomaterials Science, Department of Restorative and Biomaterials Sciences
5) Heartful Dental Clinic
6) Aoba Dental Clinic
7) Matsumoto dental university department of Dental science and material
8) Mieji Dental Clinic
9) Iryo Hojin Shikyoukai, Yabuki Dental Clinic
10) Fukuda Dental Clinic
COI: There are no conflicts of interest to disclose regarding this paper.
All subjects have given their consent for the publication of this paper.
(表4)Radiographic measurements at baseline and final examination(図1)
a) Mesial surface of first molar with an angular bony defect present after active therapy
b) The same sites 9 years later
c) mesial site site second moler with an even outline of the alveolar bone after active therapy
d) The same sites 9 years later
Waerhaug, J. The angular bone defect and its relationship to trauma from occlusion and downgrowth of subgingival plaque. J Clin Periodontol. April 1979; 6(2):61-82. doi:10.1111/j.1600-051x.1979.tb02185.x.
Papapanou, P.N., & Wennström, J.L. The angular bony defect as indicator of further alveolar bone loss. J Clin Periodontol. May 1991; 18(5):317-22. doi:10.1111/j.1600-051x.1991.tb00435.x.
Rams, T.E., Listgarten, M.A., & Slots, J. Radiographic alveolar bone morphology and progressive periodontitis. J Periodontol. April 2018; 89(4):424-430. doi:10.1002/JPER.17-0279.
Ehnevid, H., Jansson, L., Lindskog, S., & Blomlöf, L. Periodontal healing in horizontal and vertical defects following surgical or non-surgical therapy. Swed Dent J. 1997; 21(4):137-47.
Nibali, L., Pometti, D., Tu, Y.K., & Donos, N. Clinical and radiographic outcomes following non-surgical therapy of periodontal infrabony defects: A retrospective study. J Clin Periodontol. 2011; 38:50–57. doi:10.1111/j.1600-051X.2010.01648.x.
Lang, N.P. Focus on intrabony defects—conservative therapy. Periodontol 2000. February 2000; 22:51-8. doi:10.1034/j.1600-0757.2000.2220105.x.
Cortellini, P., Buti, J., Pini Prato, G., & Tonetti, M.S. Periodontal regeneration compared with access flap surgery in human intra-bony defects 20-year follow-up of a randomized clinical trial: Tooth retention, periodontitis recurrence and costs. J Clin Periodontol. January 2017; 44(1):58-66. doi:10.1111/jcpe.12638.
Greenstein, B., Frantz, B., Desai, R., Proskin, H., Campbell, J., & Caton, J. Stability of treated angular and horizontal bony defects: A retrospective radiographic evaluation in private periodontal practice. J Periodontol. 2009 Feb;80(2):228-33.doi: 10.1902/jop.2009.080158
Pontoriero, R., Nyman, S., & Lindhe, J. The angular bony defect in the maintenance of the periodontal patient. J Clin Periodontol. March 1988; 15(3):200-4. doi:10.1111/j.1600-051x.1988.tb01570.x.
Magnusson, I., Runstad, L., Nyman, S., & Lindhe, J. J Clin Periodontol. May 1983; 10(3):333-40. doi:10.1111/j.1600-051x.1983.tb01282.x.
Glickman, I. Clinical significance of trauma from occlusion. J Am Dent Assoc. March 1965; 70:607-18. doi:10.14219/jada.archive.1965.0261.
Fan, J., & Caton, J.G. Occlusal trauma and excessive occlusal forces: Narrative review, case definitions, and diagnostic considerations. J Clin Periodontol. June 2018; 45(Suppl 20):S199-S206. doi:10.1111/jcpe.12949.
Jepsen, S., Caton, J.G., Albandar, J.M., et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. June 2018; 45(Suppl 20):S219-S229. doi:10.1111/jcpe.12951.
1) The Nippon Dental University, School of Life Dentistry, Department of Periodontology
2) Sugita Dental Clinica
3) Wada Dental Clinic
4) Meikai University School of Dentistry, Division of Dental Biomaterials Science, Department of Restorative and Biomaterials Sciences
5) Heartful Dental Clinic
6) Aoba Dental Clinic
7) Matsumoto dental university department of Dental science and material
8) Mieji Dental Clinic
9) Iryo Hojin Shikyoukai, Yabuki Dental Clinic
10) Fukuda Dental Clinic
COI: There are no conflicts of interest to disclose regarding this paper.
All subjects have given their consent for the publication of this paper.
Resumen
Este estudio investigó el riesgo asociado con los defectos óseos residuales en forma de cuña después de la terapia periodontal activa, específicamente su impacto en la progresión de la periodontitis y la pérdida dental. Se analizaron datos de 24 pacientes diagnosticados con periodontitis generalizada o localizada (Estadio 3 o superior) en 64 sitios, con un período medio de mantenimiento de 116,6 meses.
El análisis comparativo entre los sitios con defectos óseos en forma de cuña (grupo experimental) y aquellos con reabsorción ósea horizontal (grupo de control) no reveló diferencias estadísticamente significativas en la progresión de la reabsorción ósea ni en la exacerbación de la enfermedad. Las evaluaciones radiográficas tampoco mostraron diferencias significativas en el volumen de reabsorción ósea entre ambos grupos.
Entre los factores que influyen en la progresión de la enfermedad, la acumulación de placa se identificó como un factor de riesgo estadísticamente significativo. En contraste, la morfología del defecto óseo, la profundidad de sondaje (PPD ≥5 mm) y la presencia o ausencia de la lámina dura no mostraron una correlación significativa con la progresión de la enfermedad.
Estos hallazgos sugieren que, incluso en presencia de defectos óseos en forma de cuña, el mantenimiento periodontal a largo plazo puede mitigar eficazmente la progresión de la enfermedad a un nivel comparable al de los sitios con reabsorción ósea horizontal. Esto resalta el papel fundamental del control de placa en la gestión posterior al tratamiento periodontal, más que la morfología del defecto óseo en sí.
Este estudio proporciona una re-evaluación de las implicaciones clínicas de los defectos óseos en forma de cuña en el cuidado periodontal a largo plazo y ofrece nuevas perspectivas para las estrategias de mantenimiento periodontal.
Palabras clave: Wedge-shaped bone defect, periodontal maintenance, prognosis, bone resorption, tooth loss
I. Introducción
La periodontitis es una enfermedad crónica y progresiva, causada principalmente por el biofilm, que conduce a la pérdida de inserción y la reabsorción del hueso alveolar a medida que avanza. El patrón de reabsorción ósea varía según las condiciones individuales; sin embargo, en muchos casos, se cree que la ubicación de la placa dental está estrechamente relacionada con la pérdida ósea alveolar.1 En general, los patrones de reabsorción ósea se clasifican en defectos óseos en forma de cuña (verticales) y reabsorción ósea horizontal, siendo los primeros una preocupación clínica significativa.2,3
El enfoque fundamental para el tratamiento de la periodontitis con defectos óseos en forma de cuña es la eliminación del biofilm, y se ha informado de mejoras mediante la terapia periodontal no quirúrgica.4,5 Además, los procedimientos quirúrgicos periodontales han demostrado inducir un aumento óseo promedio de 1.5 mm.6 Asimismo, se ha encontrado que la terapia de regeneración de los tejidos periodontales es particularmente efectiva en defectos óseos de más de 3 mm de profundidad, con reportes de resultados favorables a largo plazo.7 Sin embargo, incluso después del tratamiento periodontal, los defectos óseos no siempre se nivelan por completo, y con frecuencia se observan defectos residuales en forma de cuña.8
Los estudios radiográficos realizados durante la terapia de mantenimiento después del tratamiento periodontal activo han sugerido que los defectos óseos en forma de cuña no representan un factor de riesgo significativo.8,9 Por otro lado, estudios clínicos que incluyen evaluaciones tanto radiográficas como clínicas han reportado que los defectos óseos en forma de cuña presentan una mayor progresión de la reabsorción ósea en comparación con la reabsorción ósea horizontal, especialmente en ausencia de la lámina dura, lo que indica un mayor riesgo de progresión.3
Dado que los estudios previos han arrojado resultados inconsistentes, se requieren investigaciones a largo plazo y de alta calidad para esclarecer el impacto de los defectos óseos en forma de cuña residuales en la progresión de la periodontitis. Por lo tanto, este estudio tiene como objetivo analizar el riesgo que representan los defectos óseos en forma de cuña residuales después de la terapia periodontal activa, en relación con la progresión de la periodontitis y la pérdida dental.
II. Sujetos y Métodos
Este estudio retrospectivo fue aprobado por el Comité de Ética de la Academia de Odontología Clínica (The Academy of Clinical Dentistry). Se incluyeron pacientes diagnosticados con periodontitis generalizada o localizada en estadio 3 o superior, que habían completado terapia periodontal activa y continuado con terapia periodontal de soporte (SPT) durante al menos cinco años en ocho centros odontológicos entre enero de 2010 y diciembre de 2023.
A partir de los registros médicos de estos pacientes, se recopilaron parámetros clínicos, información del paciente e imágenes radiográficas para su análisis. Los criterios de inclusión y exclusión del estudio fueron los siguientes.
Criterios de Elegibilidad:
Edad entre 25 y 75 años al inicio de la terapia periodontal de soporte (SPT).
Presencia de al menos 20 dientes remanentes después de la terapia periodontal activa.
Disponibilidad de resultados del examen periodontal y radiografías (intraorales o panorámicas) en el momento del SPT posterior al tratamiento activo.
Presencia de defectos óseos en forma de cuña identificados durante la reevaluación después del tratamiento activo.
Criterios de Exclusión:
Presencia de restauraciones o aparatos ortodónticos que puedan afectar los resultados del tratamiento o el análisis radiográfico.
Lesiones periapicales persistentes o en progresivo agrandamiento hasta la evaluación final.
Falta de disponibilidad de los resultados del examen periodontal y de las imágenes radiográficas.
Ausencia de resultados del examen periodontal después del tratamiento inicial.
Lesiones influenciadas por terceros molares impactados.
Extracción de dientes antes de la reevaluación posterior al tratamiento activo.
Superficies dentarias con afectación de furcación.
Todos los exámenes periodontales se realizaron utilizando el método de seis sitios por diente en toda la boca, registrando la profundidad de sondaje (PPD) y la presencia o ausencia de sangrado al sondaje (BOP). La presencia de placa se registró en cuatro superficies por diente.
Datos Registrados en los Expedientes Médicos
Se extrajo la siguiente información de los expedientes médicos:
Edad
Sexo
Número de dientes remanentes en la línea base (BL, después de completar el tratamiento activo) y en la evaluación final (FE, durante el mantenimiento/SPT)
Índice de placa en toda la boca desde BL hasta FE
Porcentaje de sitios con sangrado al sondaje (BOP%) desde BL hasta FE
Porcentaje de sitios con profundidad de sondaje (PPD) ≥ 4 mm desde BL hasta FE
Estado de tabaquismo
Historia médica (condiciones sistémicas)
Frecuencia anual de visitas para SPT
Otros hallazgos relevantes
A partir de este conjunto de datos, se seleccionaron los pacientes y sitios que cumplían con los criterios de elegibilidad. Con base en los resultados del examen periodontal y los hallazgos radiográficos durante la reevaluación después del tratamiento activo, se categorizaron en los siguientes grupos.
Grupo Experimental
Sitios donde se observó un defecto óseo en forma de cuña (vertical) de 2 mm o más en las superficies interproximales en las imágenes radiográficas.
Grupo de Control
Sitios con reabsorción ósea horizontal observados en la superficie lisa del diente contralateral, adyacente o de un diente similar en el mismo paciente.
Radiographic Image Analysis
Se utilizaron radiografías dentales (periapicales o panorámicas) tomadas en la línea base (BL) y en la evaluación final (FE) mediante la técnica de proyección apical para realizar las mediciones. Todas las imágenes radiográficas fueron digitalizadas, importadas a una computadora y analizadas con el máximo nivel de ampliación en la pantalla.
En el grupo experimental, la longitud radicular se midió como la distancia desde la unión amelocementaria (CEJ) hasta el ápice radicular. La pérdida ósea se cuantificó mediante la medición de:
La distancia desde la CEJ hasta la base del defecto óseo.
La profundidad del defecto óseo, medida desde la cresta alveolar hasta la base del defecto.
De manera similar, en el grupo de control, la longitud radicular y la pérdida ósea se midieron utilizando la misma metodología. Para estandarizar los datos, todas las mediciones se ajustaron en función de la longitud radicular promedio de 10 mm para individuos japoneses.
Se evaluó la presencia de defectos intraóseos y la condición de la lámina dura (LD) en la cresta alveolar interdental. Se consideró que la LD estaba intacta si aparecía como una línea blanca radiopaca continua, sin interrupciones a lo largo de los márgenes superior e inferior.
Análisis de Datos
Se calcularon los valores medios o las frecuencias de cada parámetro clínico desde la línea base (BL) hasta la evaluación final (FE).
Profundidad de sondaje (PPD):
Se analizaron las diferencias entre los grupos experimental y de control, así como los cambios desde BL hasta FE dentro de cada grupo, utilizando una prueba t pareada.
La diferencia en el cambio medio desde BL hasta FE entre los grupos también se analizó mediante una prueba t pareada.
Sangrado al sondaje (BOP) y presencia de placa:
Se analizaron las diferencias entre los grupos y dentro de cada grupo mediante una prueba de chi-cuadrado.
Análisis radiográfico:
En el grupo experimental, los cambios en la pérdida ósea (mm) y en la profundidad del defecto óseo (mm) desde BL hasta FE se analizaron mediante una prueba t pareada.
En el grupo de control, los cambios en la profundidad del defecto óseo desde BL hasta FE también se analizaron mediante una prueba t pareada.
Además, la pérdida ósea en BL y FE, así como la diferencia en la progresión de la pérdida ósea entre los grupos experimental y de control, se analizaron mediante una prueba t pareada.
La presencia o ausencia de la lámina dura se analizó mediante una prueba de chi-cuadrado, tanto para las diferencias dentro de cada grupo como entre los grupos.
Evaluación de la Progresión de la Enfermedad Periodontal
El número de dientes perdidos y la progresión de la reabsorción ósea (categorizada como ≥0.5 mm, ≥1.0 mm y ≥1.5 mm) se analizaron mediante una prueba de chi-cuadrado para evaluar las diferencias entre los grupos.
Para identificar los factores asociados con la progresión de la reabsorción ósea, se realizó un análisis de regresión logística multivariable, utilizando los factores de riesgo como variables explicativas y la progresión de la enfermedad periodontal como variable dependiente.
III. Resultados
En este estudio, se analizaron un total de 64 sitios de 24 pacientes que cumplían con los criterios de inclusión. La duración de la terapia periodontal de soporte (SPT) desde la línea base (BL) hasta la evaluación final (FE) osciló entre 60 y 215 meses (media: 116.6 meses). Se observó la pérdida de un diente en el grupo experimental, y este diente fue excluido del cálculo de los parámetros clínicos medios y de las mediciones radiográficas, pero se incluyó en el análisis de la progresión de la enfermedad periodontal.
Como se muestra en la Tabla 1, se resumieron las características de los pacientes en BL (al completar la terapia periodontal activa). Los cambios longitudinales en los parámetros clínicos de toda la boca se presentan en la Tabla 2. No se observaron cambios significativos en el índice medio de placa, sangrado al sondaje (BOP) o en la proporción de sitios con una profundidad de sondaje (PPD) ≥4 mm. Sin embargo, el número de dientes perdidos mostró una reducción estadísticamente significativa.
(Tabla 1) Demographic and clinical parameters of study patiens at baseline.(Tabla 2) Clinical parameter at baseline(BL) and final examinations(FE)
La Tabla 3 presenta los cambios longitudinales en los parámetros clínicos para los grupos experimental y de control. La PPD media en BL y FE fue significativamente mayor en el grupo experimental en comparación con el grupo de control. No obstante, el cambio en la PPD de BL a FE no mostró una diferencia significativa entre los grupos.
(Tabla 3) Clinical parameters at baseline and final examination on the study tooth site
En cuanto al BOP, el grupo experimental presentó valores significativamente mayores en FE en comparación con el grupo de control, aunque los cambios dentro de cada grupo desde BL hasta FE no fueron estadísticamente significativos. El número de superficies afectadas por placa no mostró diferencias significativas entre ni dentro de los grupos.
Los resultados del análisis radiográfico se presentan en la Tabla 4. La cantidad de pérdida ósea en BL y FE fue significativamente mayor en el grupo experimental en comparación con el grupo de control. Sin embargo, el cambio en la pérdida ósea de BL a FE no mostró una diferencia significativa entre los grupos. Por otro lado, la profundidad de los defectos óseos en el grupo experimental disminuyó significativamente de BL a FE. No se observaron diferencias estadísticamente significativas en la presencia de la lámina dura, ni dentro ni entre los grupos. La Fig.1 muestra un caso representativo.
(Tabla 4) Radiographic measurements at baseline and final examination(Fig.1)
a) Mesial surface of first molar with an angular bony defect present after active therapy
b) The same sites 9 years later
c) mesial site site second moler with an even outline of the alveolar bone after active therapy
d) The same sites 9 years later
La frecuencia de "sitios con progresión de la enfermedad" se presenta en la Tabla 5. Al incluir el caso de pérdida dental en el grupo experimental, se analizó la progresión de la reabsorción ósea en tres umbrales (>0.5 mm, >1.0 mm, >1.5 mm). No se observaron diferencias significativas en la progresión de la enfermedad entre los grupos en ningún umbral.
(Tabla 5) Number of disease progression at each threshold level
Los resultados del análisis de regresión logística multivariable se presentan en laTabla 6. Cuando la progresión de la enfermedad se definió como reabsorción ósea superior a 1 mm o pérdida dental, se identificó que la acumulación de placa era un factor de riesgo independiente significativo (razón de momios ajustada: 2.36, p < 0.05). En contraste, la PPD ≥5 mm, la morfología ósea (defectos en forma de cuña vs. horizontales) y la presencia o ausencia de la lámina dura no mostraron significancia estadística.
(Tabla 6) The resut of multivariate logistic regression analysis for disease progression (adjusted by years of SPT and smoking status)
IV. Discusión
Los resultados de este estudio indican que los defectos óseos en forma de cuña identificados en la reevaluación después de la terapia periodontal activa no presentaron una progresión significativamente mayor de la reabsorción ósea en comparación con los sitios con reabsorción ósea horizontal, siempre que los pacientes continuaran con la terapia de mantenimiento con una frecuencia anual promedio de 4.1 ± 2.2 veces por año. Específicamente, no se observaron diferencias significativas en la cantidad de reabsorción ósea medida en radiografías ni en la proporción de sitios que empeoraron durante el período de observación entre los defectos óseos en forma de cuña y los sitios con reabsorción ósea horizontal.
Este hallazgo es coherente con los estudios a largo plazo de Greenstein et al.8 y Pontoriero et al.,9 así como con el estudio en modelos animales de Magnusson et al.,11 los cuales demostraron que no existen diferencias en la longitud del epitelio de unión ni en la resistencia a la periodontitis.
Por otro lado, los resultados de este estudio difieren de informes previos que sugieren que los defectos óseos en forma de cuña experimentan una mayor progresión de la reabsorción ósea en comparación con los sitios con reabsorción ósea horizontal. Por ejemplo, Papapanou et al.2 realizaron un estudio retrospectivo en el que analizaron 201 radiografías panorámicas durante un período de 10 años, informando que los sitios con defectos óseos en forma de cuña presentaban una reabsorción ósea significativamente mayor (>2 mm) y tenían una mayor incidencia de pérdida dental en defectos más profundos. Sin embargo, este estudio no consideró los tratamientos posteriores a la línea base, y es probable que muchos pacientes no hayan recibido terapia periodontal integral. Por lo tanto, la población de estudio difiere de la de nuestra cohorte, en la cual los pacientes continuaron la terapia de mantenimiento durante 5 a 17 años.
De manera similar, Rams et al.3 realizaron un estudio prospectivo de 36 meses y encontraron que los defectos óseos en forma de cuña tenían una probabilidad significativamente mayor de deteriorarse en comparación con los sitios con reabsorción ósea horizontal. Sin embargo, su estudio tuvo un período de observación más corto y no incluyó un análisis de pérdida dental, lo que lo diferencia del presente estudio.
Además, Rams et al.3 informaron que cuando un defecto óseo en forma de cuña estaba acompañado por la presencia de la lámina dura, la tasa de progresión de la enfermedad era menor. Se considera que la lámina dura está asociada con la resolución de la inflamación y la estabilización de los tejidos periodontales; sin embargo, en nuestro estudio, no se encontró dicha correlación. Esta discrepancia podría deberse a diferencias en los métodos de estandarización radiográfica.
En cuanto a la pérdida dental, se registró un único caso de extracción dentaria en el grupo de defectos en forma de cuña, mientras que no se observó pérdida dental en el grupo de reabsorción ósea horizontal. No obstante, el diente extraído presentaba una PPD de 9 mm con BOP en la línea base tras la terapia periodontal activa, lo que sugiere que el tratamiento periodontal no fue exitoso en este caso. Estudios de mayor escala que analicen la pérdida dental como un criterio de valoración podrían arrojar resultados diferentes.
La presencia de defectos óseos en forma de cuña suele considerarse un signo de trauma oclusal.12 Sin embargo, en este estudio, ninguno de los dientes evaluados presentó movilidad en la línea base (BL), ni mostró movilidad progresiva durante el período de observación. Los informes de consenso recientes establecen que las condiciones patológicas relacionadas con el trauma oclusal secundario se caracterizan por una movilidad dentaria progresiva. Por lo tanto, en este estudio, no se observó ninguna relación entre los defectos óseos en forma de cuña y el trauma oclusal.
En este estudio, la frecuencia de adherencia de placa en BL fue de aproximadamente el 50% en ambos grupos. Aunque se observó una tendencia a la mejora en la evaluación final (FE), no se encontraron diferencias estadísticamente significativas. Como resultado, el grupo de control mostró una tendencia a la reducción en la frecuencia de BOP, mientras que el grupo experimental permaneció sin cambios. En FE, la frecuencia de BOP fue significativamente menor en el grupo de control en comparación con el grupo experimental, lo que probablemente se deba a diferencias morfológicas.
A pesar de la finalización del tratamiento activo, la PPD media en BL fue mayor en el grupo experimental que en el grupo de control. Del mismo modo, la pérdida ósea media en el grupo experimental fue significativamente mayor que en el grupo de control en BL, lo que concuerda con los hallazgos de la PPD. No obstante, a pesar de estas diferencias, no se observaron diferencias intergrupales significativas en la progresión longitudinal de la reabsorción ósea ni en el empeoramiento de los parámetros clínicos, lo que indica resultados estables en ambos grupos.
Por lo tanto, la PPD y BOP más elevadas observadas en el grupo experimental durante el período de estudio no indican necesariamente una condición patológica, aunque se recomienda una observación a más largo plazo.
Este estudio calculó la pérdida ósea en función de las mediciones de la longitud radicular obtenidas a partir de imágenes radiográficas, ajustadas a la longitud radicular promedio de individuos japoneses. Cuando las mediciones se realizan en radiografías no estandarizadas, como en este estudio, la pérdida ósea suele evaluarse mediante métodos proporcionales, como el uso de cuadrículas. Sin embargo, las mediciones proporcionales pueden subestimar la reabsorción ósea en dientes con raíces relativamente más largas, como los caninos. Expresar la pérdida ósea en valores absolutos en lugar de proporciones proporciona una evaluación más relevante desde el punto de vista clínico. No obstante, ajustar las mediciones a la longitud radicular promedio de la población japonesa no considera las variaciones individuales, lo que representa una limitación de los estudios retrospectivos. Para mejorar la precisión, se necesitan futuros estudios prospectivos utilizando imágenes radiográficas estandarizadas.
En este estudio, la progresión de la enfermedad se definió como "pérdida dental + progresión de la reabsorción ósea", y se realizó un análisis de regresión logística multivariable. Los resultados no mostraron correlación entre los patrones de reabsorción ósea alveolar y la progresión de la enfermedad; sin embargo, la acumulación de placa estuvo significativamente asociada con la progresión de la enfermedad.
Además, aunque la presencia de bolsas periodontales >5 mm no alcanzó significación estadística, la razón de momios (odds ratio) fue de 2.3. Esto sugiere que en pacientes que reciben terapia de mantenimiento a largo plazo, el estado de higiene oral y los parámetros clínicos periodontales pueden contribuir más significativamente a la progresión de la periodontitis que la morfología del defecto óseo.
V. Conclusión
Este estudio demostró que, incluso en los casos donde los defectos óseos en forma de cuña persisten después de la terapia periodontal activa, la terapia de mantenimiento a largo plazo puede prevenir diferencias significativas en el riesgo de progresión de la periodontitis en comparación con los sitios con reabsorción ósea horizontal.
Además, el análisis multivariable identificó que la acumulación de placa es el factor de riesgo más significativo para la progresión de la periodontitis, mientras que la morfología del defecto óseo, la profundidad de sondaje (PPD ≥5 mm) y la presencia o ausencia de la lámina dura no alcanzaron significación estadística.
Estos hallazgos sugieren que, en el mantenimiento posterior a la terapia periodontal, el control efectivo de la placa es más importante para prevenir la progresión de la periodontitis que la presencia de defectos óseos en forma de cuña. Este estudio proporciona una revisión de las implicaciones clínicas de los defectos óseos en forma de cuña y ofrece orientación para el manejo periodontal a largo plazo después del tratamiento.
References:
Waerhaug, J. The angular bone defect and its relationship to trauma from occlusion and downgrowth of subgingival plaque. J Clin Periodontol. April 1979; 6(2):61-82. doi:10.1111/j.1600-051x.1979.tb02185.x.
Papapanou, P.N., & Wennström, J.L. The angular bony defect as indicator of further alveolar bone loss. J Clin Periodontol. May 1991; 18(5):317-22. doi:10.1111/j.1600-051x.1991.tb00435.x.
Rams, T.E., Listgarten, M.A., & Slots, J. Radiographic alveolar bone morphology and progressive periodontitis. J Periodontol. April 2018; 89(4):424-430. doi:10.1002/JPER.17-0279.
Ehnevid, H., Jansson, L., Lindskog, S., & Blomlöf, L. Periodontal healing in horizontal and vertical defects following surgical or non-surgical therapy. Swed Dent J. 1997; 21(4):137-47.
Nibali, L., Pometti, D., Tu, Y.K., & Donos, N. Clinical and radiographic outcomes following non-surgical therapy of periodontal infrabony defects: A retrospective study. J Clin Periodontol. 2011; 38:50–57. doi:10.1111/j.1600-051X.2010.01648.x.
Lang, N.P. Focus on intrabony defects—conservative therapy. Periodontol 2000. February 2000; 22:51-8. doi:10.1034/j.1600-0757.2000.2220105.x.
Cortellini, P., Buti, J., Pini Prato, G., & Tonetti, M.S. Periodontal regeneration compared with access flap surgery in human intra-bony defects 20-year follow-up of a randomized clinical trial: Tooth retention, periodontitis recurrence and costs. J Clin Periodontol. January 2017; 44(1):58-66. doi:10.1111/jcpe.12638.
Greenstein, B., Frantz, B., Desai, R., Proskin, H., Campbell, J., & Caton, J. Stability of treated angular and horizontal bony defects: A retrospective radiographic evaluation in private periodontal practice. J Periodontol. 2009 Feb;80(2):228-33.doi: 10.1902/jop.2009.080158
Pontoriero, R., Nyman, S., & Lindhe, J. The angular bony defect in the maintenance of the periodontal patient. J Clin Periodontol. March 1988; 15(3):200-4. doi:10.1111/j.1600-051x.1988.tb01570.x.
Magnusson, I., Runstad, L., Nyman, S., & Lindhe, J. J Clin Periodontol. May 1983; 10(3):333-40. doi:10.1111/j.1600-051x.1983.tb01282.x.
Glickman, I. Clinical significance of trauma from occlusion. J Am Dent Assoc. March 1965; 70:607-18. doi:10.14219/jada.archive.1965.0261.
Fan, J., & Caton, J.G. Occlusal trauma and excessive occlusal forces: Narrative review, case definitions, and diagnostic considerations. J Clin Periodontol. June 2018; 45(Suppl 20):S199-S206. doi:10.1111/jcpe.12949.
Jepsen, S., Caton, J.G., Albandar, J.M., et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. June 2018; 45(Suppl 20):S219-S229. doi:10.1111/jcpe.12951.