1) Department of Operative Dentistry, Endodontology and Periodontology, School of Dentistry, Matsumoto Dental University.
2) Oral Health Science, Department of Oral Health Promotion, Oral Science Course, Matsumoto Dental University Graduate School of Oral Medicine.
3) Yamaguchi Dental Clinic,Nagano,Japan.
4) Department of Removable Partial Prosthodontics, Tokyo Dental College.
5) Asunaro Pediatric Dental Clinic, Toyama, Japan.
6) Tai Dental Clinic,Kanagawa,Japan.
7) Department of Hard Tissue Research, Graduate School of Oral Medicine, Matsumoto Dental University.
The oral function of periodontitis patients is maintainable only after inflammation is tightly regulated, and additionally, after proper vertical and horizontal jaw position is established and occlusal relationship is restored as typically found in posterior disocclusion with anterior guidance. Advanced periodontitis is however characterized by progressive periodontal tissue breakdown leading to teeth mobility and pathologic migration. As a result, once the occlusal balance is disturbed,excessive force load is applied in the form of traumatic occlusion, causing the periodontal tissue to surpass its adaptive threshold, thereby generating secondary occlusal trauma, and in turn, further periodontal tissue destruction in more than a few cases.
Treatment goals were established for a patient on the verge of experiencing occlusal collapse due to broad type periodontitis, which was to stabilize inflammation and occlusion. We would like to present a case in which positive results were achieved with interdisciplinary treatment team approach that includes specialties such as periodontal disease, orthodontics, prosthetic treatment, which led to long term stability. The patient was a 39-year-old male at the time of initial visit. He presented to the Periodontal Disease Department of the Matsumoto Dental University Hospital with a chief complaint of teeth mobility across the full jaw length. After being diagnosed with broad type periodontitis resulting in teeth separation and misaligned crowded teeth, basic periodontal treatment and periodontal surgery were performed with improvement in the periodontal tissue. With subsequent treatment for oral function improvement, teeth misalignment improved, and dentition continuity was achieved with orthodontic treatment. Ultimately, occlusion was established across the full jaw length with prosthetic treatment, whereby healthy oral environment was achieved; the patient has been on Supportive Periodontal Therapy (SPT) for 10 years.
Key words:broad type periodontitis, malalignment of teeth, prosthetic treatment, team approach, interdisciplinary treatment
Introduction
Periodontitis is a chronic inflammatory disease caused by infectious permanent bacteria in oral cavity,characterized by breakdown and resorption of gingival connective tissues and alveolar bones, which is a lifestyle disease contracted by approximately 50% of the Japanese population that are 40 years or older.1 After periodontitis has progressed, pathologic mobility and migration generally occur as the disease progresses. Reports have indicated that pathologic teeth migration was observed in 30 – 55.8% of periodontitis patients.2-4 Additionally, periodontal tissue breakdown is evident in advanced periodontitis patients. In more than a few cases of such patients, the periodontal tissue cannot bear the chewing forces and occlusal forces that were exerted when these patients were healthy. The occlusal forces exacerbate teeth mobility after exceeding the adaptive threshold of the periodontal tissue, which results in occlusal trauma breaking down the periodontal tissue, and in secondary trauma on the periodontal membrane, and thus further exacerbate the already compromised oral health of such patients. Furthermore, malalignment of teeth and malocclusion in patients with healthy periodontal tissue cause poor occlusal contact relationship with the teeth on the opposite counterpart of the jaw, leading to early occlusal contact, excessive lateral force, and traumatic occlusion, thereby causing primary occlusal trauma in healthy periodontal tissues. Therefore, inflammatory periodontal diseases and traumatic occlusion are interrelated, and mutually contribute to the exacerbation of one another, and thus, to provide long-term stability in oral health and to prevent recurrence of various challenges, occlusal treatment for periodontitis involving traumatic occlusion, in addition to controlling inflammations, is imperative for stabilizing occlusion and for dispersing occlusal force.
Moreover, patients with advanced periodontal disease often suffer from complex disorders involving dental caries, dental pulp disease, esthetics, temporomandibular joints in addition to periodontal disease, and therefore in many cases require interdisciplinary treatment in their treatment plans consisting of a combination of multiple treatment approaches, such as coronal restoration, endodontic, orthodontic and prosthetic treatments in addition to periodontitis treatment by specialists in each area.5-7
Here we would like to present a case report on a patient whose periodontitis progressed at a young age. This patient has been maintaining well on long-term SPT after a team of specialists in each department of Matsumoto Dental University Hospital provided interdisciplinary treatment in a single mouth.
Case
Patient: 39 years old (at the time of initial visit), male
Initial visit: June 2007
Chief complaint: teeth mobility across the full jaw length
1. Systemic medical history
No systemic medical history to make note of.
2. Oral medical history
Sometime around 2004 (at age 35), the patient received treatment for caries on a few teeth at a nearby dentist. Until then, he did not have any preexisting caries or periodontal diseases. and had never seen a dentist. In the same year however, as he noticed movement in his teeth across his full jaw, he received his first diagnosis at the Matsumoto Dental University Hospital (hereinafter “this hospital”). He was busy back then, and therefore, only received treatments for carries a few times and had periodontal pockets cleaned. In 2005 (age 36), in addition to teeth movement, he began to notice gingival bleeding, foul breath, food particles between teeth. In June 2007 (age 39), he returned to this hospital for a visit and was referred to the periodontics.
3. Family history
Both parents have been wearing complete upper and lower dentures from age 65. The brother, who is 5 years older than him, has been receiving treatments at a nearby dentist after being diagnosed with periodontitis.
4. Lifestyle and habits
The patient has a history of smoking 20 cigarettes a day for 5 years in his 20s. He did not drink regularly but occasionally drank 180ml of alcoholic beverages with his work peers.
5. Present condition
1) Systemic findings
166cm tall,weighs 64.0kg,with BMI(Body Mass Index) of 23.2 , medium build medium height.
2) Intraoral findings
(1) Macroscopic findings
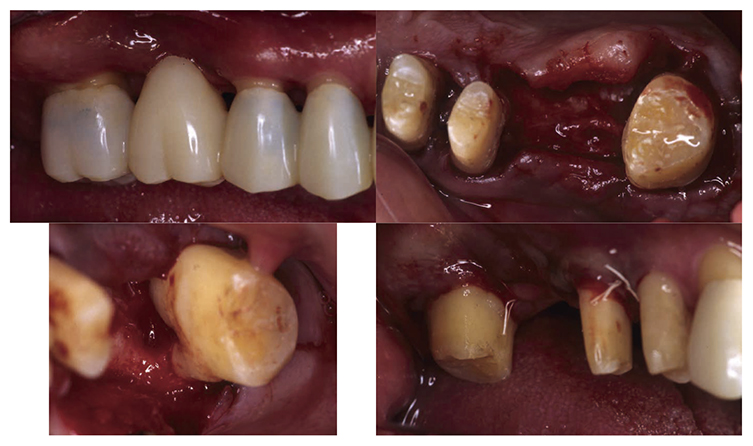
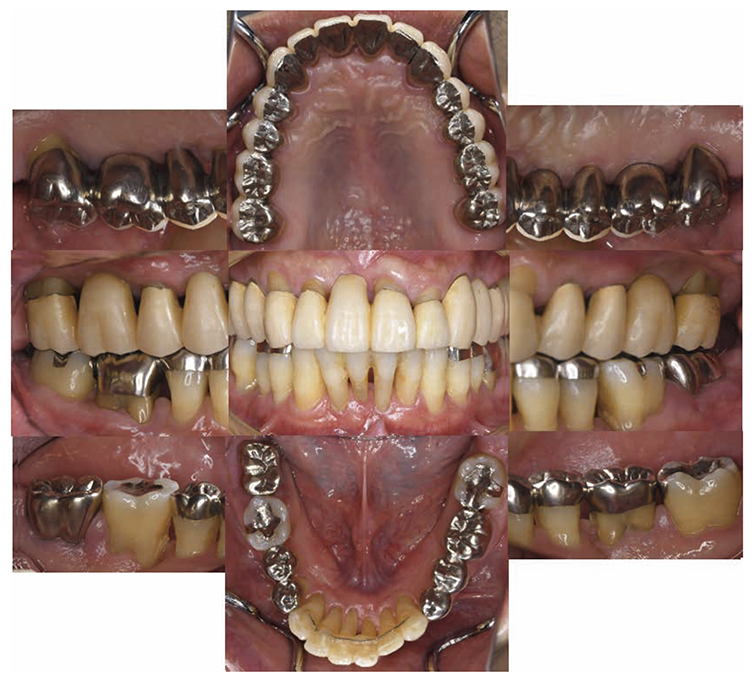
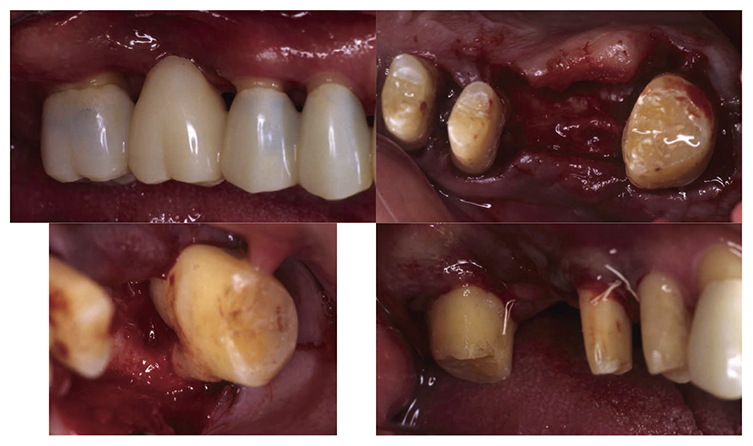
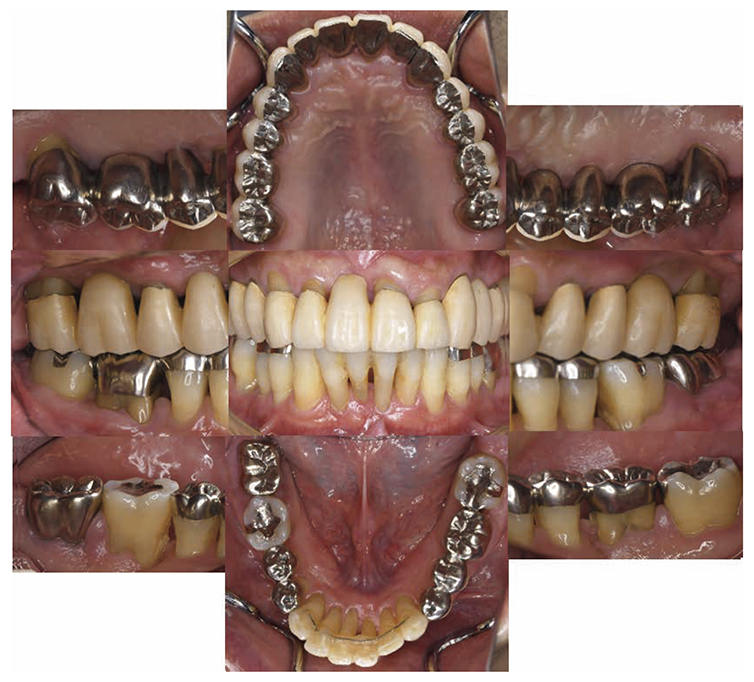
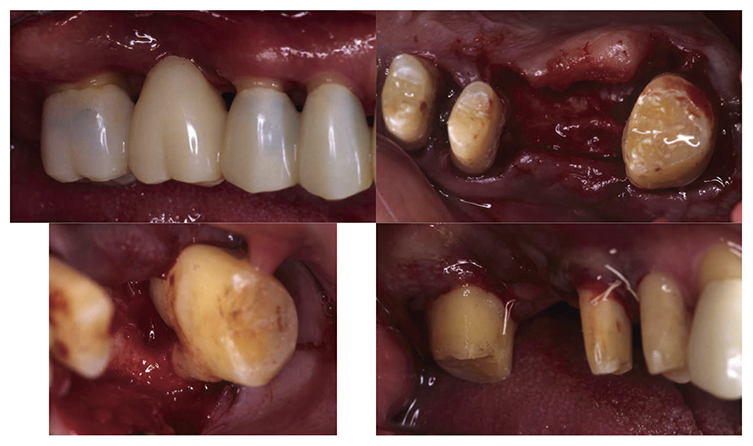
No obvious redness and swelling were present in the marginal gingiva across the full jaw; some blood congestion was however observed. The gingival shape of the anterior teeth in the mandible and maxilla was that of a thick shelf. Significant gingival recession was observed on the mandibular anterior teeth and the buckle side of the left and right maxillary first molar. The dental arch on the maxilla and mandible had a parabolic shape. Teeth separation was however observed between the maxillary central incisors, maxillary right central incisor and lateral incisor, maxillary right canine and first premolar, maxillary left canine and first premolar, and crowding was observed in the mandibular central incisors (Fig.1a).
(2) Examination of periodontal tissue
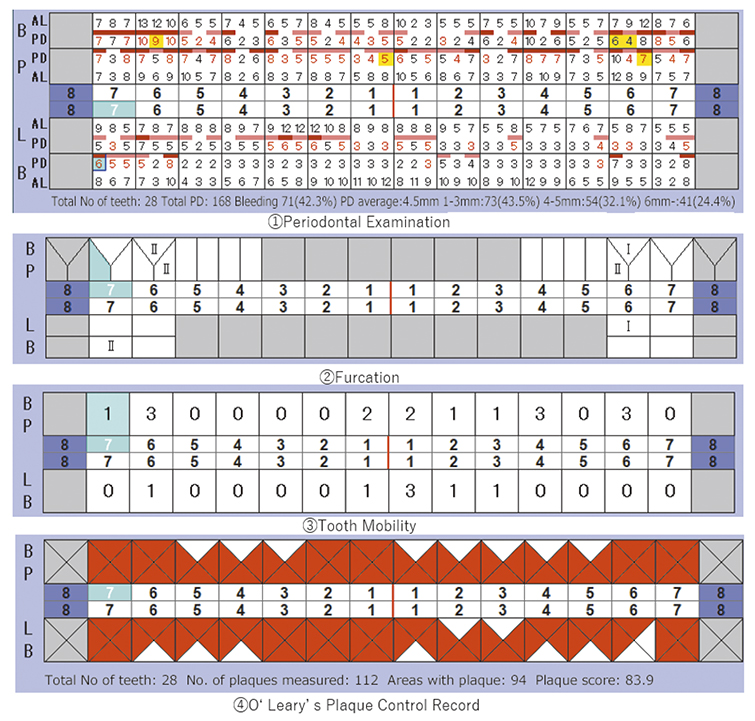
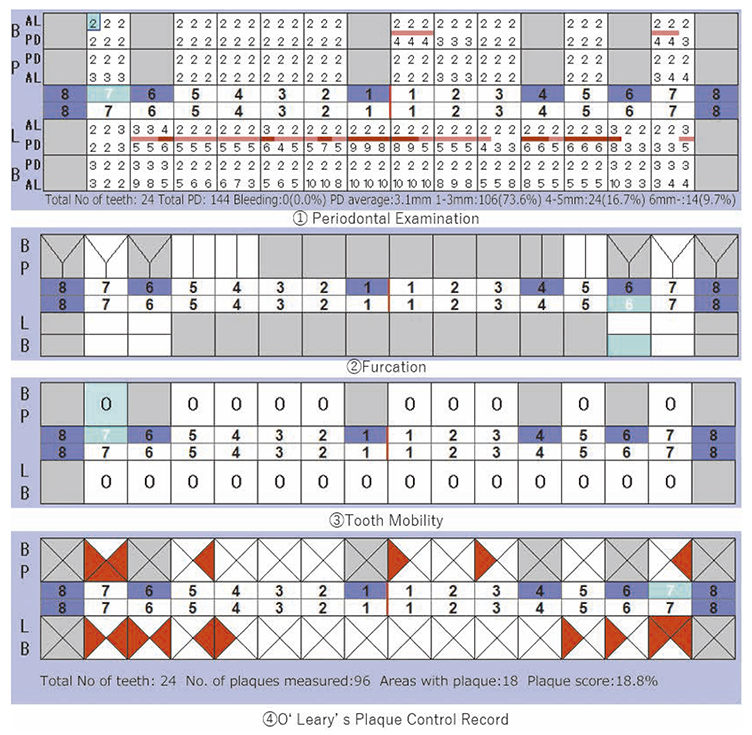
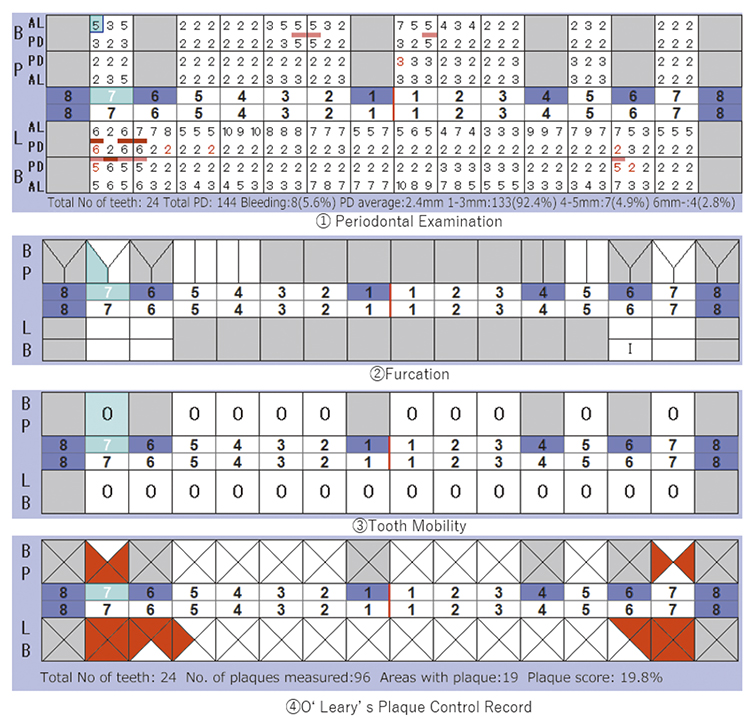
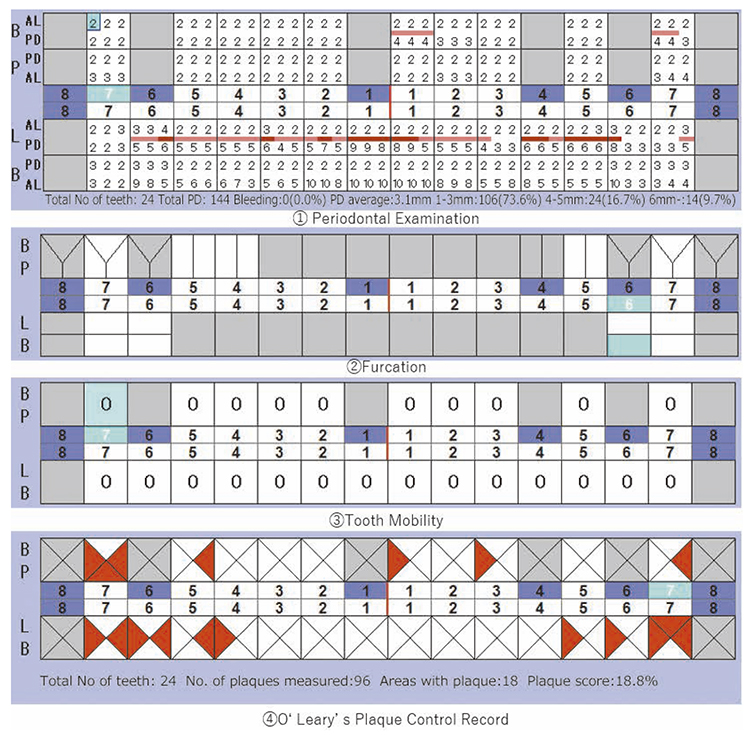
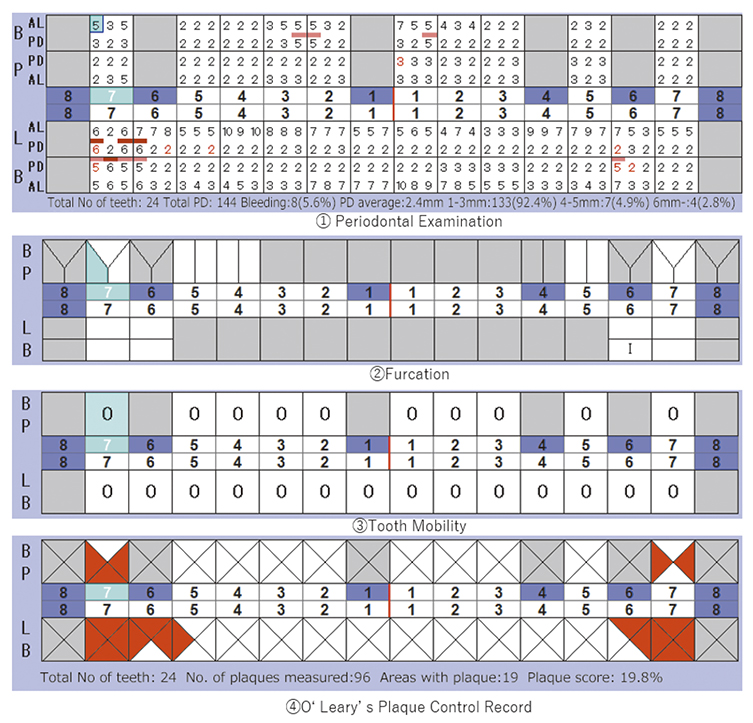
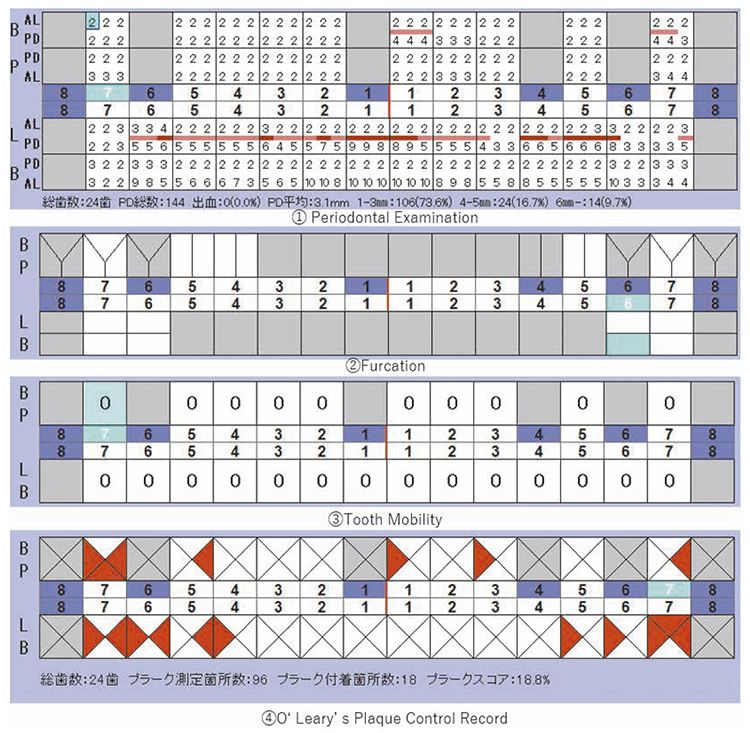
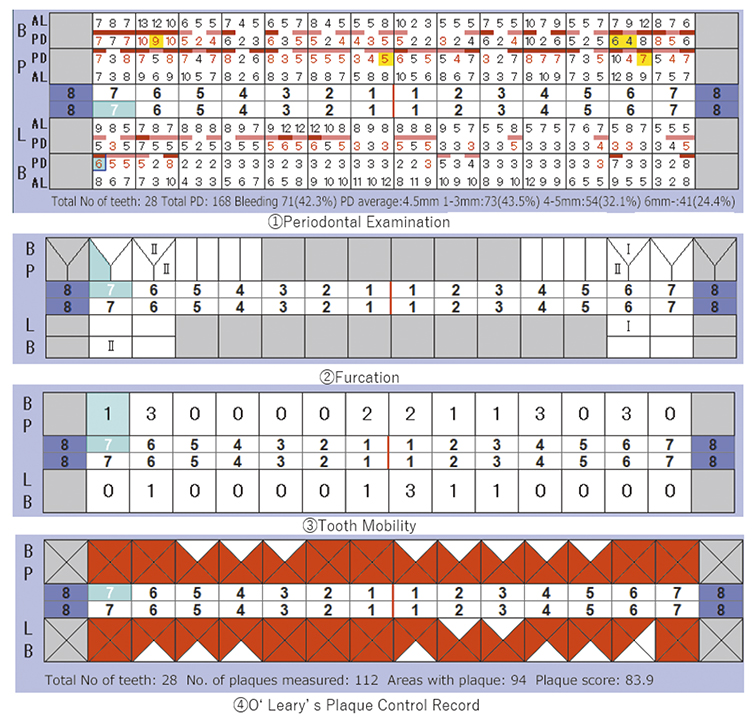
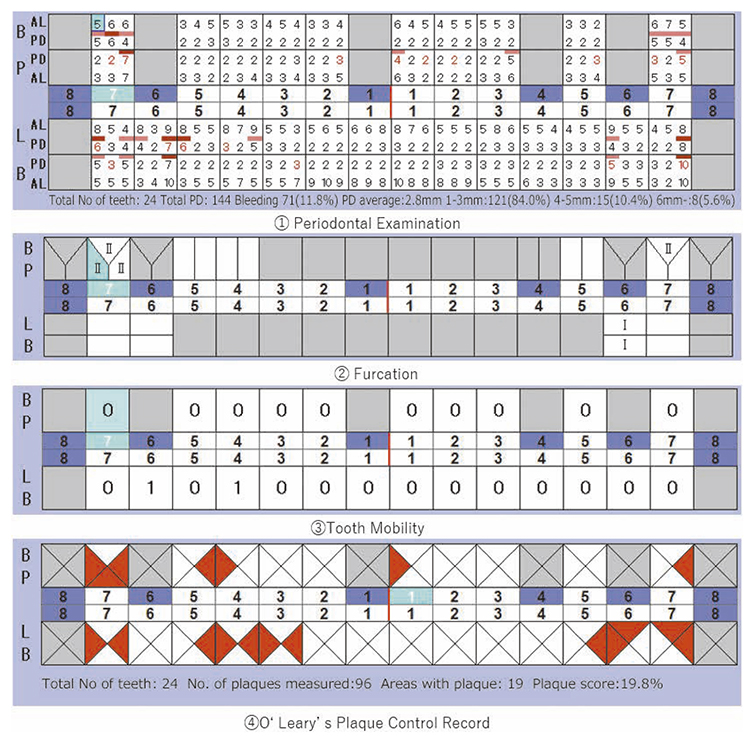
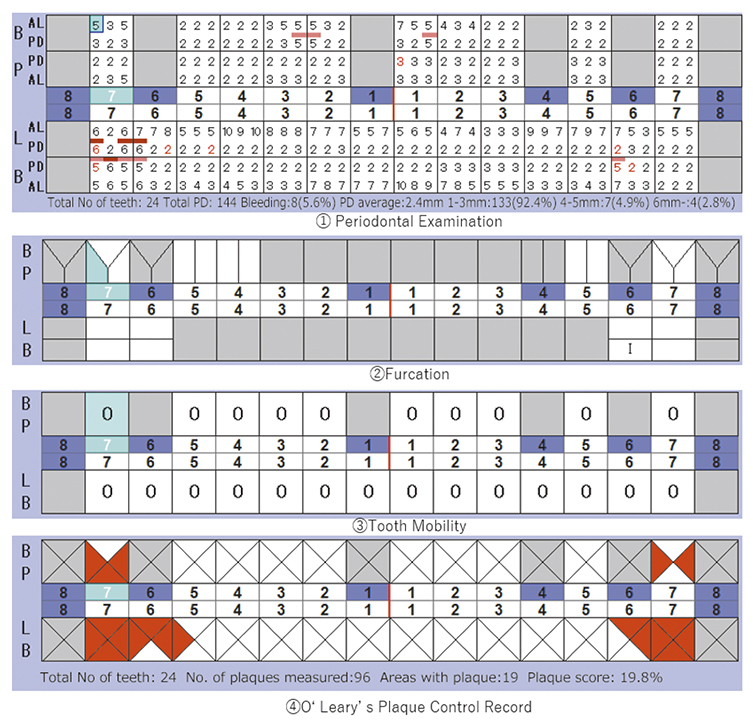
At the time of first visit, the average PD (Probing Depth) on the full jaw was 4.5mm,maximum PD was 10.0mm, 43.5% had PD of 3mm or less,38.7% for 4-6mm,17.9% for 7mm or above. The average BOP (Bleeding on Probing) on the full jaw was 42.3%,teeth mobility on 17,22,23,32,33,41,46 was grade 1,grade 2 on 11,12,21,and grade 3 on 16,24,26,31 (Miller classification). Additionally, grade 1 on 36,16(mesial, distal),26 (mesial, distal) and 36,grade 2 furcation involvement (Lindhe & Nyman classification) was observed on 47. The plaque score at the first visit (O’Leary’s Plaque Control Record:PCR value) was 83.9%, which indicated poor oral hygiene status (Fig.1b).
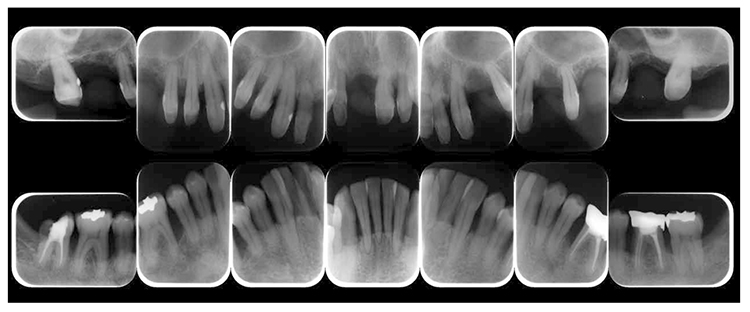
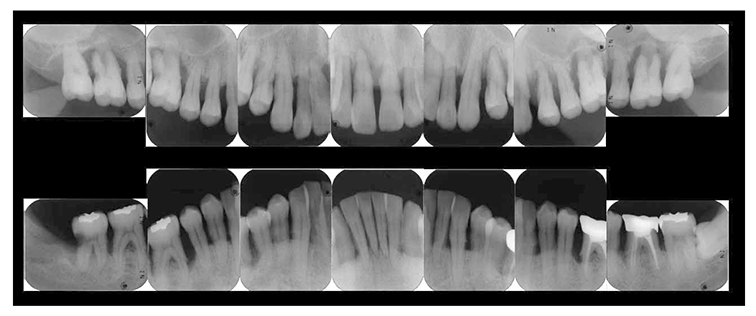
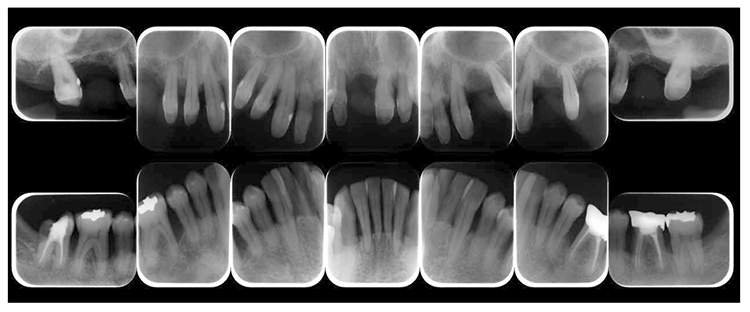
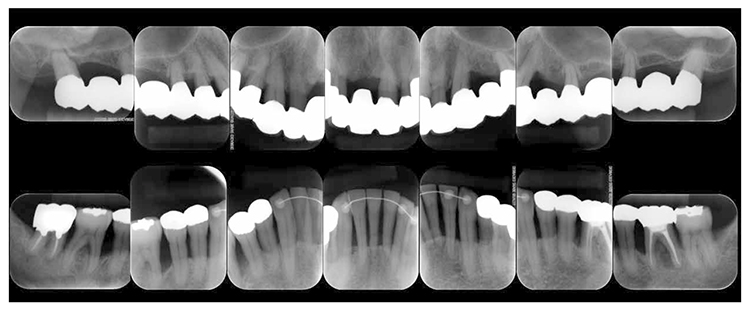
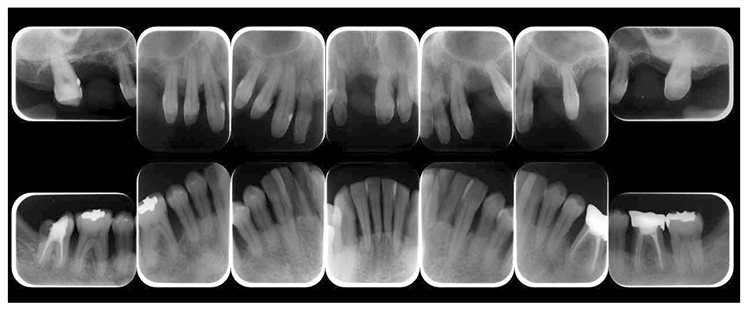
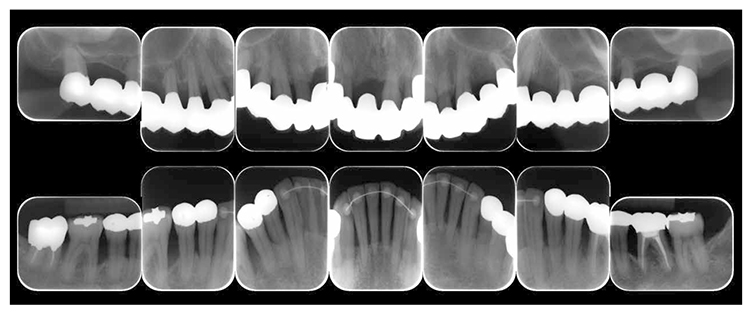
(3) X-ray findings
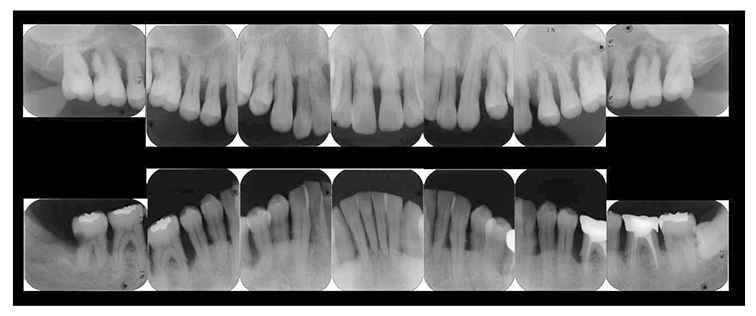
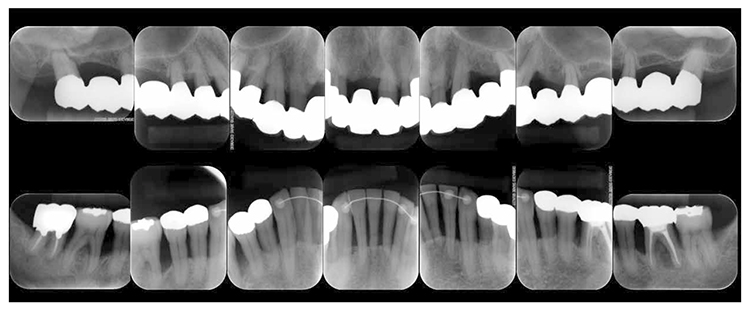
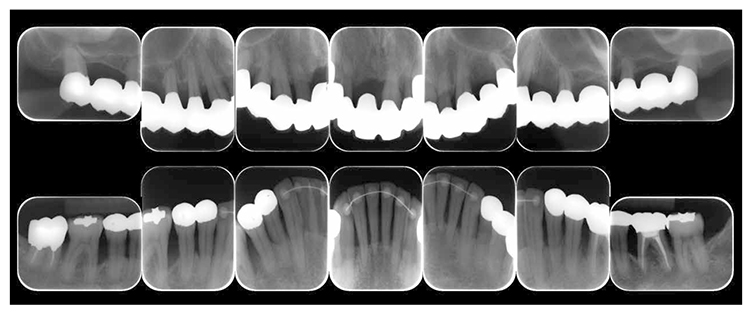
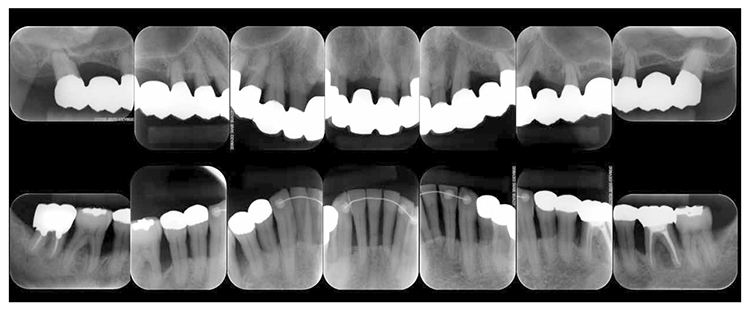
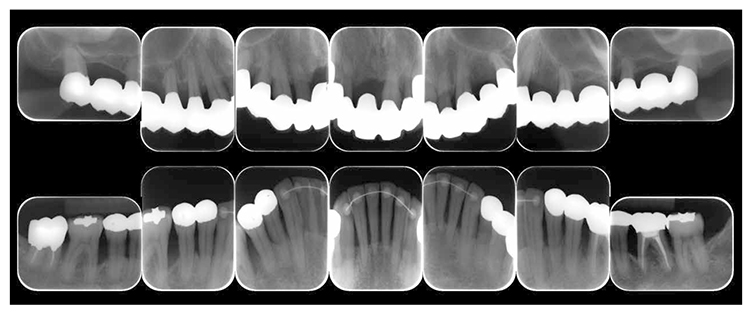
At the first visit, the findings showed moderate to advanced horizontal alveolar bone resorption in the entire jaw, and advanced vertical bone resorption on 24,36,46, 47. Additionally, on 46,47 were radiolucent findings that were likely associated with furcation involvement, and radiolucent areas on the alveolar bone surrounding the root apex were shown on 16,11,26. Furthermore, distally on 47, radiolucent findings showed caries extending into the dental pulp.(Fig.1c).
(Fig.1a) Intraoral photo taken during first visit (June 2007)
(Fig.1b) Results of periodontal tissue examination during first visit (June 2007)
(Fig.1c) Dental X-ray 14 during first visit (June 2007)
6. Bacterial antibody test
Bacterial antibody test for periodontal disease (DEMECAL®,Leisure Inc., Tokyo) was performed. Blood was drawn from the fingertip on an empty stomach, 3 hours after the meal. Antibody findings of 4 bacterias, A.a bacteria (Actinobacillus actinomycetemcomitans), P.g bacteria (Porhyromonas gingivalis), P.i bacteria (Prevotella intermedia), E.cbacteria (Eikenella corrodens) showed that antibody titer did not rise in any of the 4 bacteria species including A.a bacteria that is unique to aggressive periodontitis.
7. Cause
1) Systemic risk factor: none
2) Local risk factor: Plaques, malalignment of teeth, traumatic occlusion
8. Diagnosis
After a comprehensive examination including medical history and clinical condition,the patient was diagnosed with stage Ⅳ, grade C broad type periodontitis.
9. Treatment plan
Treatment strategy
A comprehensive treatment plan was established as follows to provide orthodontic treatment and prosthetic treatment after the periodontal tissue has improved though periodontitis treatments.
① Examination of the periodontal tissue, bacteriological examination, diagnosis
⑥ Treatment for oral function recovery (orthodontic treatment, prosthetic treatment)
⑦ Reevaluation testing
⑧ SPT (Supportive Periodontal Therapy)
Treatment plan was established as shown above and treatment began after obtaining the patient’s consent. The patient was verbally informed of future publication of this case and publication of clinical data, and consent was obtained in writing.
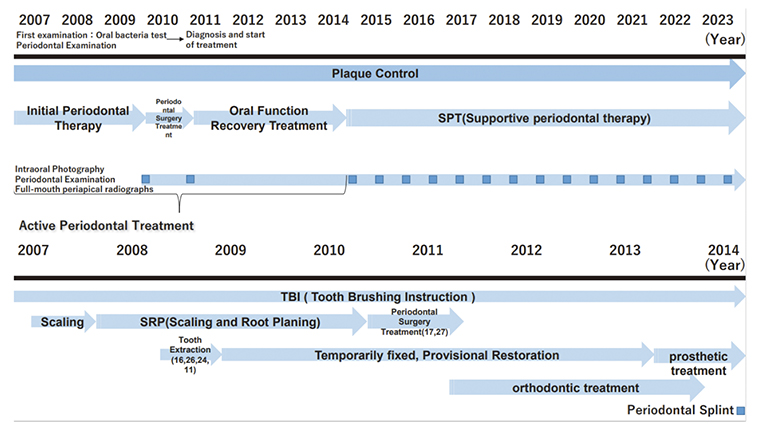
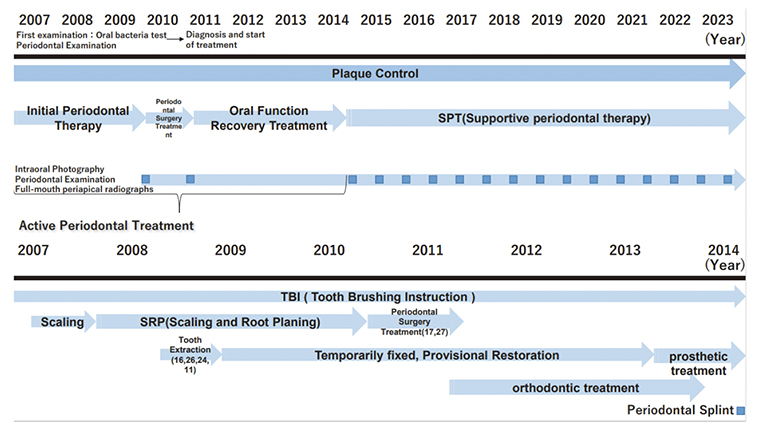
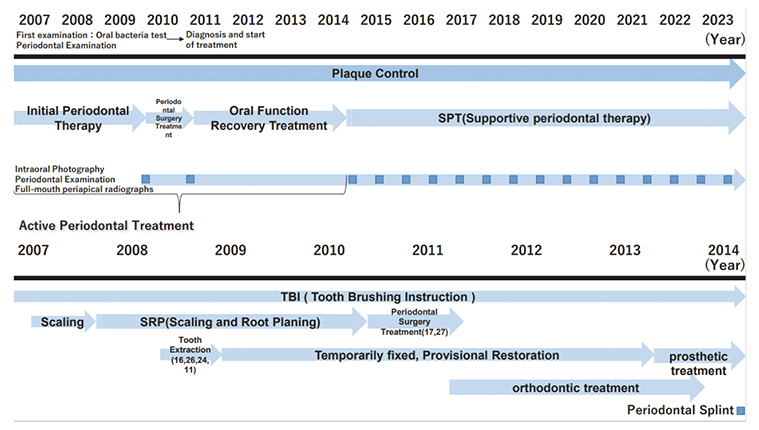
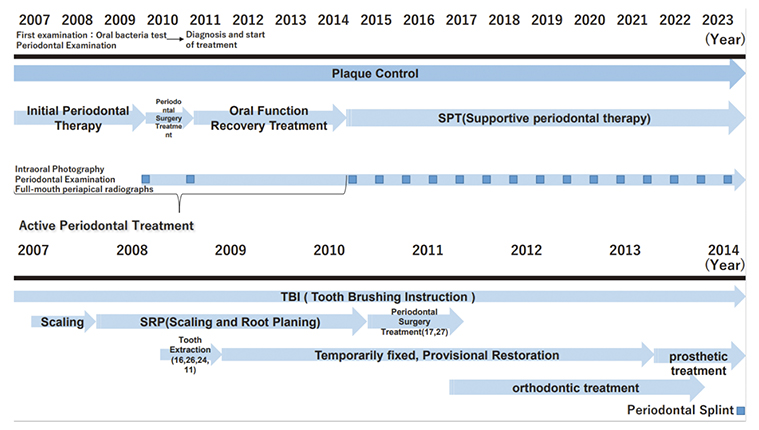
10. Treatment progress (Fig.2)
1) Basic periodontal treatment
The patient was explained that teeth mobility on entire jaw is not only caused by resorption of the alveolar bone but also by poor oral hygiene and thereafter began plaque control with manual toothbrush. The PCR value was as undesirable as 83.9%, and therefore, a manual toothbrush (Butler#211, Sunstar Inc. Osaka) was used, and scrubbing method was taught. After improvement was shown on the labial and lingual surfaces, the patient was instructed to use an interdental brush (DENT EX® 3M, interdental brush S, M, L, Lion Corporation, Tokyo) with an appropriate size for the interproximal space of the teeth. Brushing has shown effectiveness in improving PCR value only after a significant time period due to crowded mandibular anterior teeth, asymmetries of marginal gingiva caused by malalignment of teeth with interdental diastema, uneven teeth axis inclination, gingival recession and changes in gingival position after tooth extraction. During the 14th instruction session, the PCR value declined to 18.3%, and since then has been maintaining well at a steady level with minor fluctuations.
(Fig.2) Treatment process
After gingival margin plaque was reduced with brushing for self-care, SRP was performed for professional care in the order of maxillary left premolar and molar, maxillary right premolar and molar, maxillary anterior teeth, mandibular premolar and molar, mandibular anterior teeth, mandibular left premolar and molar; dental calculus in the gingival margin was removed and scaling and root planning was performed to promote gingival attachment. After completion of 1 course of SRP, the remaining dental calculus in the gingival margin on the entire jaw was detectable by tactile means, and therefore, another SRP was performed on the entire jaw. Despite basic periodontal treatment, continuous attachment loss was apparent on 16 in February 2008 (age 40) , on 26 in May in the same year, on 24 in February 2009 (age 41), and on 11 in April in the same year, and therefore teeth were extracted as the diagnosis showed that the teeth were not preservable due to continuous attachment loss. In the sockets following teeth extraction, temporary prosthetic bridges were placed for 23-27 with 23, 25 and 27 as anchors, temporary prosthetic bridges with 13,14,15 and 17 as anchors, for 12-22 with 12,21 and 22 as anchors.
Focus was placed on occlusal trauma from the mid-early stage of basic periodontal treatment. To eliminate early contact and cuspal interference, reduction and occlusal adjustment were performed. Ultimately, all units were connected and each tooth was stabilized in consideration of esthetics, the extent of the breakdown of periodontal tissues surrounding adjacent teeth, and future crown prosthesis application. From June 2007, along with periodontitis treatment, treatment for infected canal began on 47, and temporary prosthesis was placed after root canal filling was completed.
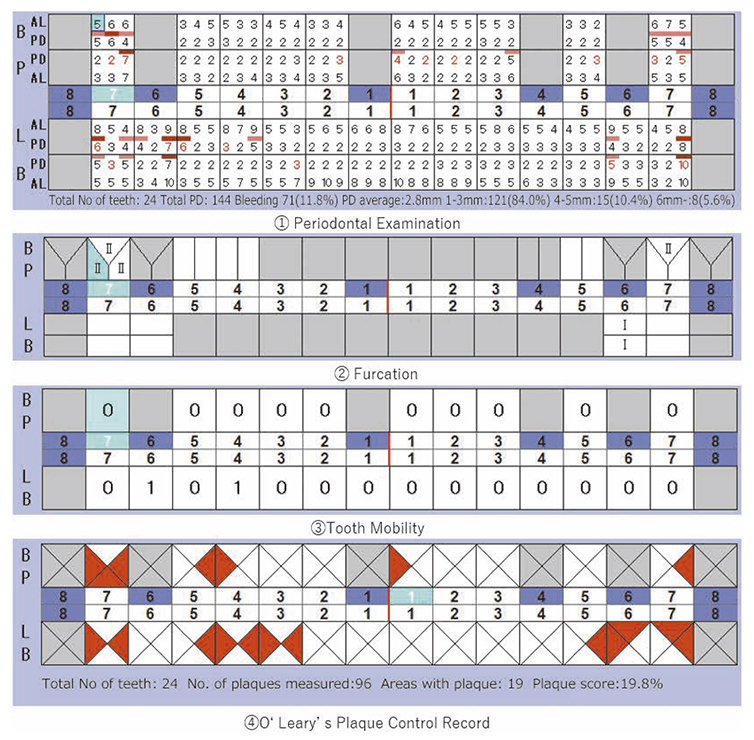
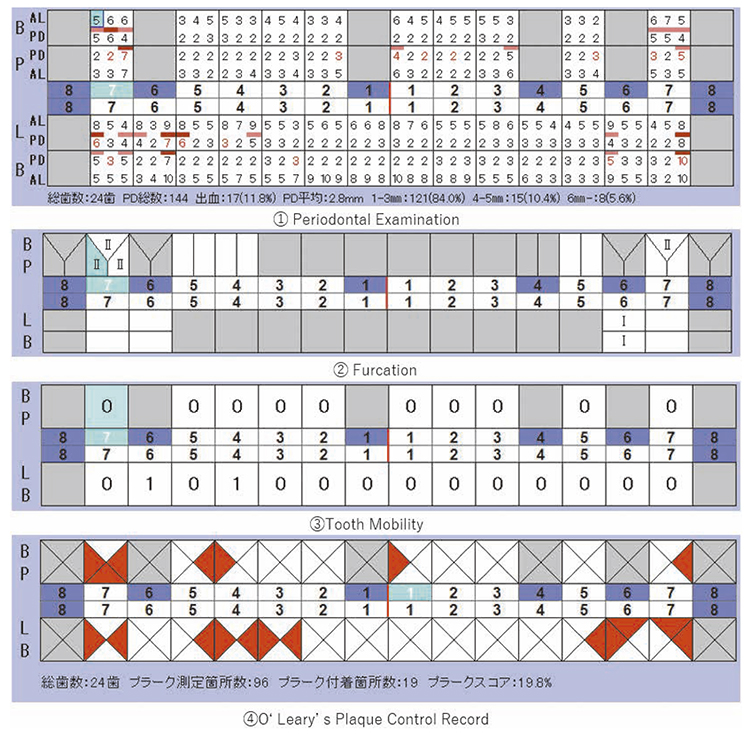
2) Reevaluation testing (February 2010)
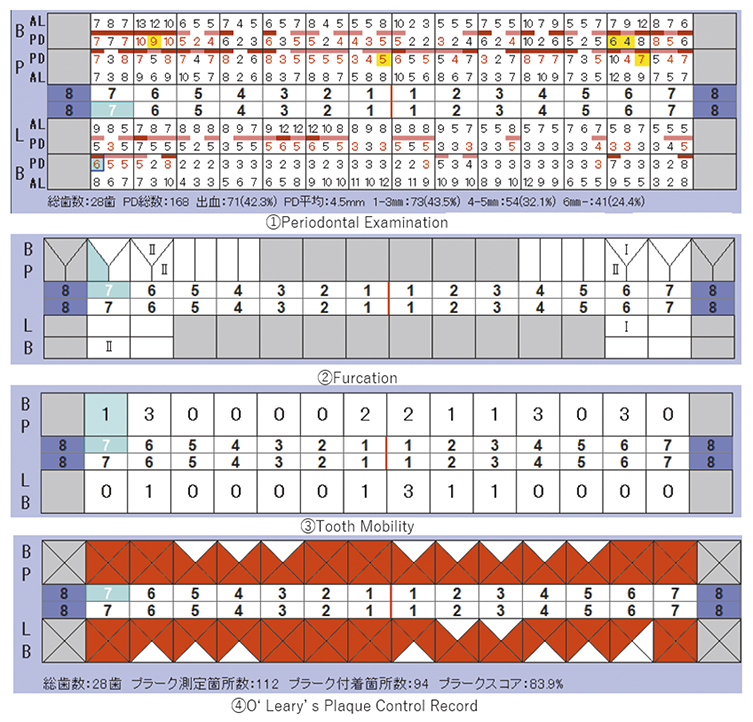
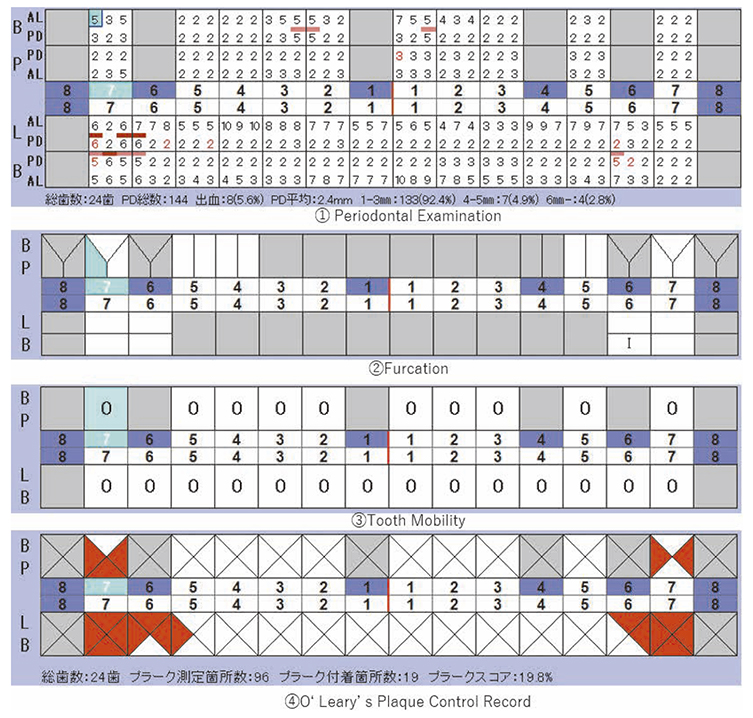
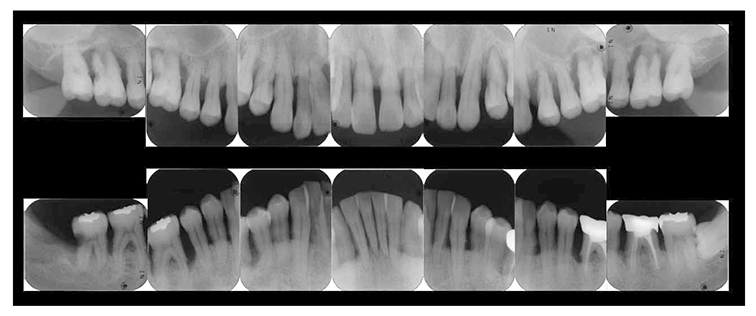
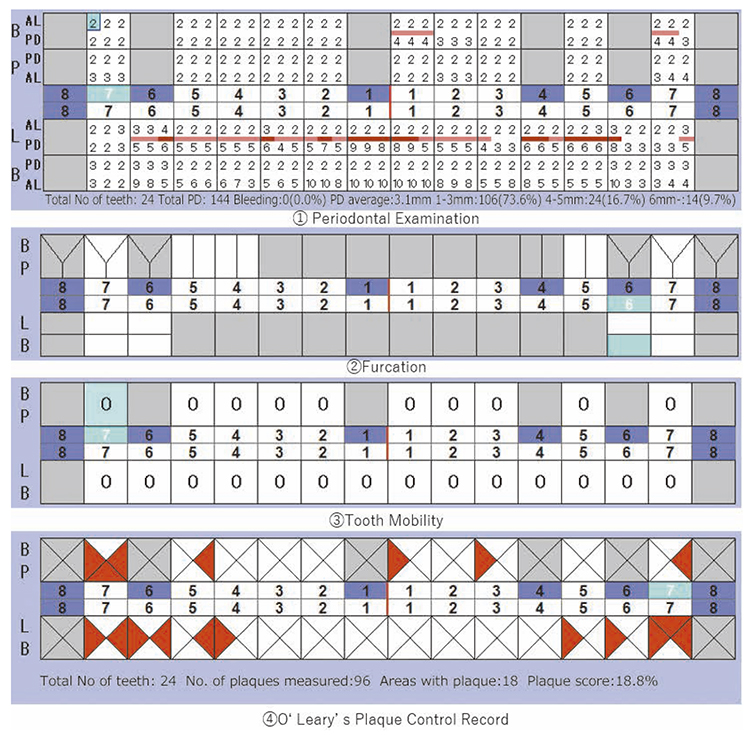
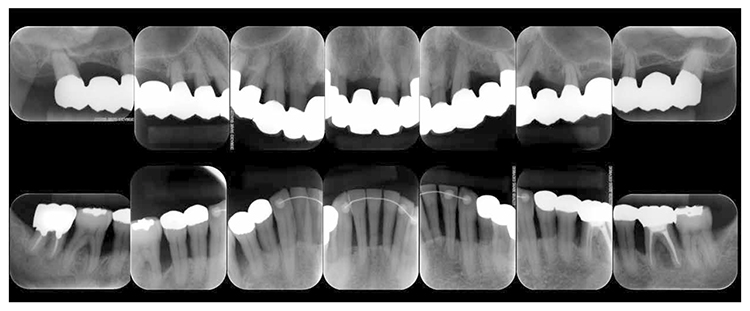
At reevaluation testing after basic periodontal treatment, the color of gingiva improved to pink, and findings showed that inflammation in the marginal gingiva with primarily blood congestion had subsided. Class 4 gingival recession (Miller’s gingival recession classification) was observed on the entire jaw. (Fig.3a). The average PD of the entire jaw was 2.8mm, maximum PD was 10.0mm, the ratio of PD of 3mm or below was 84.0%, PD of 4-6mm was 12.5%, PD of 7mm or above was 3.5% and BOP rate improved to 11.8%. However, PD of 7mm remained on 17, 10.0mm on 27, 5.0mm on 36, and 7.0mm on 46. Additionally grade 1 furcation involvement remained on the buckle and lingual side of 36, mesial distal direction on the buckle side of 17, grade 2 on the buckle side of 27. Teeth mobility was grade 1 on 44 and 46 (Fig.3b). X-ray findings showed that dental calculus was removed from the gingival margin on the maxilla and mandible. Despite the clearly visible alveolar hard line, no improvement was shown on the alveolar bone. (Fig.3c).
(Fig.3a) Intraoral photo after completion of basic periodontal treatment has completed (2010.1)
(Fig.3b) Reevaluation and examination after completion of basic periodontal treatment (January 2010)
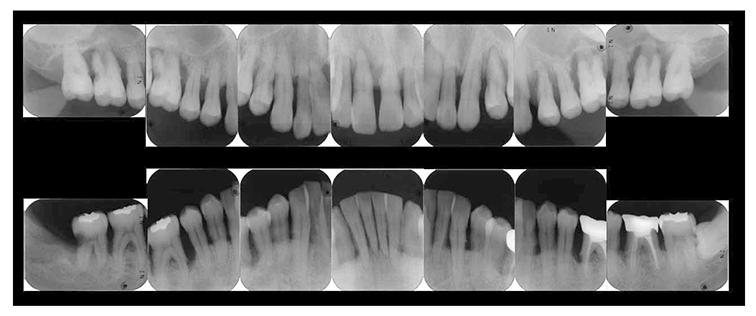
(Fig.3c) Dental X-ray 14 after completion of basic periodontal treatment (January 2010)
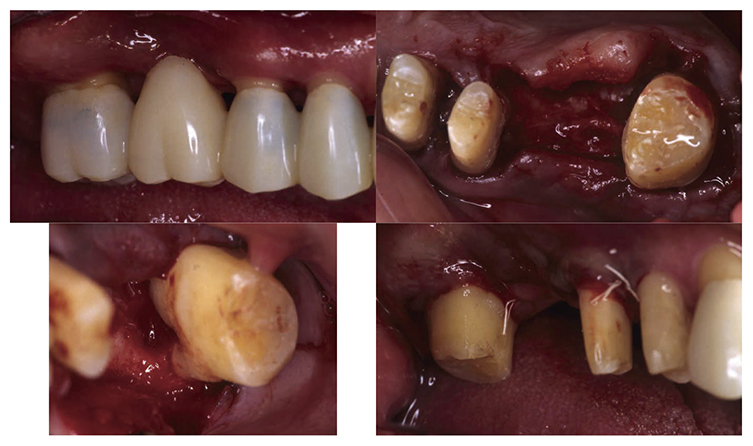
3) Periodontal surgical therapy
At the reevaluation examination after completion of basic periodontal treatment, deep periodontal pockets and grade 2 furcation involvement were observed. Therefore, in April 2010 (age 42), enamel matrix proteins were applied in a procedure for periodontal regeneration (Fig.4),and in June of the same year, gingival flap operation and distal wedge procedure were performed on 27 (Fig.5). For the remaining PD on the lingual side of 36 and 46, due to insufficient keratinized gingiva, the option was to stabilize the condition with SRP.
(Fig.4) Enamel matrix proteins were applied in a procedure for periodontal regeneration in the maxillary left molar (April 1, 2020)
(Fig.5) Gingival flap operation and distal wedge procedure were performed on the maxillary left second molar (June 2010)
4) Reevaluation testing (February 2011)
In the reevaluation testing after periodontal surgery, 4mm of PD remained on the palatal side, distally on 17 and mid-buccal area on 27. BOP was no longer present and furcation involvement improved.
5) Orthodontic treatment of mandibular anterior teeth
6 months after completion of periodontal surgical treatment, the orthodontics at this hospital began orthodontic treatment to improve the crowded mandibular anterior teeth. In October 2010 (at age 42), preoperative examination was performed, and to first improve the imbalance of the perioral muscles, MFT (Myo Functional Therapy) began. With the diagnosis of crowded mandibular anterior teeth thereafter, in December 2010, bands were attached to 36 and 46, brackets were attached to 34,33,32,31,41,42,43 and 44, and these teeth were straightened upright. Wires were adjusted every month thereafter. 1 year and 4 months after dynamic orthodontic treatment, in April 2012 (at age 44), impression was taken on the retainer, and in May 2012, canine-to-canine retainer (FSW retainer) was attached.
6) Prosthetic treatment
After orthodontic treatment was completed, fabrication of the final prosthesis was started.. Preliminary impression of the maxilla and mandible were taken, anatomic facebow and checkbite were obtained, and prosthetic diagnosis was performed. In the treatment plan before surgery, the first choice for the maxilla was the full mouth bridge that connects all teeth. However, since no parallelism was seen on the anchor teeth, and additionally all teeth were vital teeth, convenient pulpectomy was sought as a possibility. Additionally, in designing treatment for patients with severe periodontitis, to disperse the occlusal load to the entire jaw, which was most important, semi-fixed multi-tooth prosthetic using key and keyway attachment was designed for final prosthetic in this case. After taking parallelism of anchor teeth into consideration, multi-tooth models with attachments were designed for 13 and 14, and for 22 and 23. After deciding on the shape of prosthetics, anchor teeth were formed, impression was taken, and subsequently final confirmation was made on accurate fit with coping trial. After final prosthetic treatment on the maxilla, prosthetics were placed on the mandible starting with 47. Since metal crowns were placed on both 47 and 36, onlay-type metal crowns were placed on 44, 45, 34 and 35 for occlusal support. After completion of prosthetic treatment on all teeth, confirmation was made with an occlusal force tester (Dental Prescale®,GC, Tokyo) that occlusal force was equally distributed across the entire jaw. Additionally, nighttime bruxism was addressed by producing and applying nightguards since the patient had the habit of clenching.
7) Reevaluation testing (December 2003)
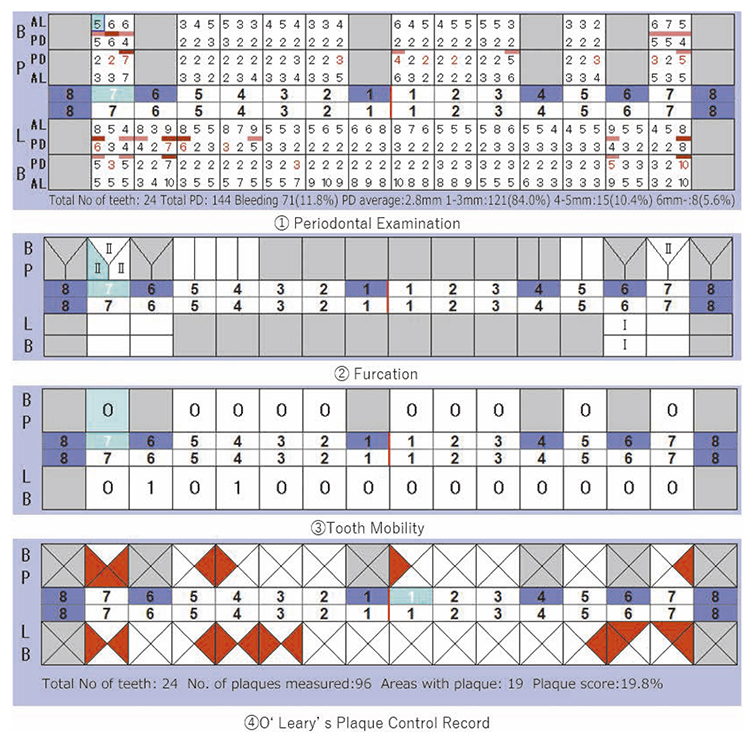
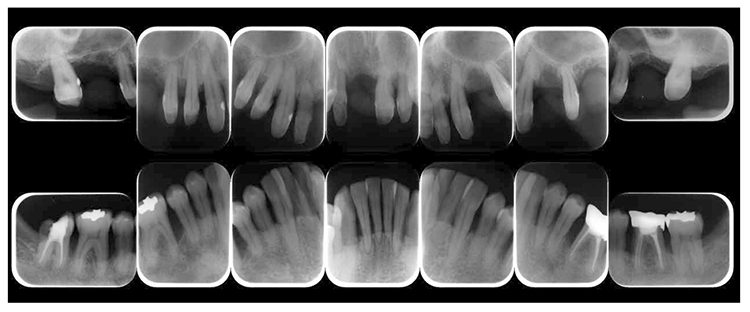
At the reevaluation examination after treatment to restore oral function, the color of gingiva was pink, and with prosthetics, intraoral harmony was replicated esthetically and functionally. (Fig.6a). The average PD across the entire jaw was 2.1mm, maximum PD was 4.0mm, the ratio of PD of 3mm or below was 99.3%, no BOP was found and the condition of the periodontal tissue was stable (Fig.6b). In the X-ray, continuity of the alveolar hard line was replicated and the sequence of bone trabeculae was normal, and therefore, the patient transitioned to the SPT phase (Fig.6c).
(Fig.6a) Intraoral photo after completion of restoration of oral function was completed(2013.4)
(Fig.6b) Reevaluation and examination after completion of restoration of oral function (April 2013)
(Fig.6c) Digital X-ray 14 after completion of restoration of oral function (April 2013)
8)SPT (December 2013 onward)
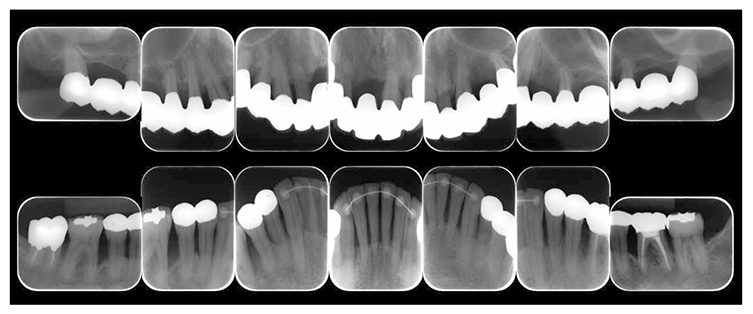
After transitioning to SPT, the patient brushed 4 times daily after every meal and before bedtime and has continued to use an interdental brush. PCR levels have been consistently in the 20% range. SPT , which primarily consists of instructions on brushing and dental surface cleaning, has been implemented every other month to present, and efforts are made to maintain and manage oral hygiene in the long term to ensure that plaque control is not insufficient. While minor discoloring is observed on the prosthetics, the color of the gingiva is salmon pink and a macroscopically healthy appearance has been sustained (Fig.7a) . The average PD on the entire jaw is 2.1mm,maximum PD is 4.0mm,the ratio of PD of 3mm or less is 99.3%. No BOP has been found and the condition of the periodontal tissue has been stable (Fig.7b). In the X-ray, continuity of the alveolar hard line has been replicated and the sequence of the bone trabeculae has been normal (Fig.7c).
(Fig.7a) Intraoral photo: 15 years after first visit (December 2022)
(Fig.7b) Examination for reevaluation: 15 years after first visit (December 2022)
(Fig.7c) 15 years after first visit: dental X-ray 14 (December 2022)
Discussion
Periodontitis is a chronic infectious disease caused by permanent bacteria in oral cavity and at the same time, the host factors such as the defense mechanism, systemic diseases, age, and genetics, and environmental factors such as stress, smoking, drugs among other things affect the progression of lesions, and therefore, long term maintenance of the oral function is not only challenging during dynamic treatment but also after treatment. In advanced periodontitis, with the progression of lesions, progressive periodontal tissue breakdown occurs, which leads to reduced periodontal tissue support. In more than a few cases of such patients, the periodontal tissue cannot bear the chewing forces and occlusal forces that were exerted when these patients were healthy, and therefore complications such as occlusal trauma develop. In such cases, in addition to periodontitis treatment that aims to remove inflammation factors and to improve lesions, an interdisciplinary treatment that targets occlusal reconstruction for occlusal stability is needed. To this end, each of the following stages, basic periodontal treatment primarily for plaque control, periodontal surgery based on the results of reevaluation examinations, treatment for oral function restoration considering secondary occlusal trauma, and the relationship between SPT and occlusal relationship that is most important for the prognosis for long-term stability must be evaluated and addressed properly.
In this case, at the time of the first visit, the patient was 39 years old with a chief complaint of teeth mobility across the full jaw. He was a broad-type periodontitis patient and since moderate to advanced horizontal bone resorption was observed in intra-oral X-rays, removal of inflammation in the periodontal tissues,disease progression control,occlusal stability,restorative esthetics needed to be sought, and an interdisciplinary treatment including periodontitis treatment, orthodontic treatment and prosthetic treatment was needed. Additionally, to stably preserve the functionality and esthetics of the stomatognathic system that were achieved as a result of an interdisciplinary treatment, inflammations (periodontitis) and traumatic occlusion must be controlled. Therefore, supportive periodontal therapy (SPT) must be implemented continuously at appropriate intervals for each case to meet treatment goals and to maintain the patient’s well-being.
1) Diagnosis with periodontitis
The diagnosis used here as of 2023 is based on the new classification that was proposed as the new classification for periodontitis by AAP/EFP during the EuroPerio 9 meeting held in Amsterdam in June 2018. The previous categorization system is different in that periodontitis was divided into two categories, invasive periodontitis and chronic periodontitis. In the new categorization system, these categories are combined to encompass periodontitis as one disease and are grouped into stages and grades in its diagnosis framework. In this case, the probing depth (PPD) was 6mm or more at the first visit. Vertical bone resorption of 3mm or more was observed in addition to furcation lesions occurring twice. 4 teeth were ultimately extracted. However since prosthetic treatment was required on the full jaw, the patient in this case was diagnosed as stage IV and stage C as the progression rate of the grade was as high as 1.0 or above with the primary factors of bone resorption %/ age. Therefore, the patient in this case was diagnosed as stage IV, grade C under the new periodontal classification based on international standards.
2) Basic periodontal treatment
To begin basic periodontal treatment based on proper diagnosis, periodontitis is a bacterial infectious disease that produces symptoms and develops over time from inflammation in the periodontal tissue, formation of periodontal pockets and buildup of subgingival dental plaque, which are caused by proliferation of periodontal pathogens primarily comprised of Anaerobic gram-negative bacteria. Such pathogens grow from dental plaque (dental biofilm) which is a group of bacteria that increase in numbers and from dysbiosis. Taking all the above into account, one of the most essential components of long-term stability during the dynamic treatment period and after treatment is likely to be to improve dental cleaning and control inflammations with improved dental cleaning.
In advanced periodontitis however, along with alveolar bone resorption, morphological changes such as formation of deep periodontal pockets,gingival recession,and pathologic migration occur; the continuity of each tissue is broken, such areas become new plaque retention factors and cause diseases to increase in severity, and thus cause a vicious cycle to amplify one another. Fortunately, in this case, continuity of dentition was preserved without missing teeth, and plaque control was performed in a conventional matter with both, a manual toothbrush and interdental brush with the appropriate size for the interproximal space of the teeth. At the first visit, the PCR value was as undesirable as 83.9%. With the 14th brushing instructions, this value was dropped to 20% or lower. A significant time commitment was required to improve the PCR value, and the periodontal tissue responded well. Secondary occlusal trauma is a local risk factor for periodontal disease, and occlusal adjustment is necessary according to the disease status. In principle, except for first aid, occlusal adjustments in periodontally ill patients should be made after removal of inflammation. This is because tooth movement in periodontal patients may be caused and enhanced by inflammation of the periodontal ligament, and teeth may move after removal of the inflammation, resulting in another occlusal trauma. In the present case, there was severe alveolar bone resorption in all jaws, and almost all teeth had secondary occlusal trauma. In the mandibular anterior and maxillary molars where the teeth were protruding and moving, the contact points were shaved from the early stage of basic periodontal treatment to reduce the harmfulness of traumatic occlusion, and inflammation was reduced by SRP, etc. After the teeth that could not respond to the treatment were extracted and a temporary restorative appliance was installed sequentially, secondary occlusal trauma was noted and the fremitus should be checked at all times. The patient was guided by the group function from the canine to the bicuspid during the occlusal fit position and lateral movement.
3) Orthodontic Treatment
In this case, orthodontic treatment was performed during the oral functional rehabilitation phase to improve the crowding in the lower anterior teeth region. Orthodontic treatment is a highly effective therapeutic method for both aesthetic and functional improvement, even in adults. However, orthodontic treatment in adults often involves issues such as dental caries, pulp diseases, periodontal disease, and dental deficiencies. Furthermore, many adults undergoing orthodontic treatment may also have systemic diseases, requiring even greater consideration and a broad range of knowledge. When treating such patients, a deep understanding of both orthodontics and periodontics is essential. Management of periodontal tissues is necessary at all stages, from orthodontic diagnosis to evaluation of periodontal tissues during treatment, plaque control, and postoperative assessment.
If inflammation of the gums is controlled, there is research indicating that orthodontic treatment does not have a detrimental effect on periodontal tissues.11 Fixed orthodontic appliances can create barriers that compromise oral hygiene and may lead to plaque retention.12,13 However, it has been reported that comprehensive dental care during orthodontic treatment reduces adverse changes such as gum bleeding14,15 and plaque accumulation.14,16 Therefore, orthodontic treatment should only be performed when active periodontal disease is under control. Recent reports suggest a consensus that establishing and maintaining inflammation-free periodontal tissues during and after orthodontic treatment is essential.17 Additionally, it is desirable to apply light forces of 5g to 15g continuously in orthodontic treatment when the periodontal ligament is compromised.18 Thus, in orthodontic treatment for periodontal disease patients, it is important to apply appropriate orthodontic forces according to the extent of remaining periodontal tissues.
In this case, in addition to the stabilization of the condition through periodontal basic treatment, there was no progression of organic changes in the alveolar bone, such as abnormal root resorption or alveolar bone resorption, compared to the initial visit based on X-ray findings after orthodontic treatment. Furthermore, significant enlargement of the periodontal ligament space was not observed, and in some areas, there was improvement in the level of the alveolar bone, with clearer delineation of the alveolar crestal lamina dura. This is believed to be due to the appropriate orthodontic forces during treatment. During orthodontic treatment, plaque control was performed monthly in the periodontal department, and examinations for early contacts and occlusal interferences occurring during dynamic treatment were conducted, with occlusal adjustments performed if necessary. The integrated approach of orthodontics and periodontics is beneficial and can contribute to ideal qualitative, functional, and aesthetic planning, particularly in complex clinical cases, leading to optimal treatment planning.19
4)Prosthetic treatment
In selecting and designing the final prosthetic treatment for this case, mainly dentures, implants and crown bridges were considered. The patient did not choose dentures from the time temporary prosthetics were adopted during basic periodontal treatment. Implant placement for the maxilla anterior region and molar region were then considered. However, the alveolar bone mass was insufficient in all areas, and due to the need for sinus lift, bone graft, and subsequent periodontal surgery, considering the balance between alveolar bone mass of antagonistic implants, the risk of implants causing traumatic occlusion was present. Additionally, the patient did not wish to place implants due to the treatment period and finances, and therefore. implants were excluded from the options, and the decision was to proceed with designing crown bridges.
In cases in which patient’s tooth mobility is caused by significant alveolar bone resorption, and treatments are not effective after occlusal adjustment, crown shape change or temporary splints, a treatment plan is imperative to encompass temporary splints and permanent splints with a broad-spectrum periodontal treatment device. Since significant alveolar bone resorption was observed in this case, a plan was established to build fixed dental prosthesis as the final prosthesis to properly disperse the chewing load not for each individual unit but along the arch overall and to prevent overload on the anchor tooth caused by diminished periodontal support. Reports indicate that a cross-arch fixed bridge provides a degree of rigidity and can prevent overload on the anchor tooth caused by diminished support of the periodontal tissue as the chewing load is properly dispersed not for each individual unit but along the arch overall.20,21 Additionally, reports show that if contamination of the periodontal tissues are under control, an anchor tooth can provide sufficient anchorage with the original alveolar bone support of 20 – 30%.22-24
5) Maintenance and SPT
Long term follow-up reports suggest that if the periodontal tissues are stable and SPT is introduced to prevent the recurrence of periodontitis, a tooth with poor periodontal tissue support may anchor a fixed prosthesis covering a wide range,24,25 which is a vitally important factor in patient’s compliance leading to long-term success, in addition to the individualized dental recall system. These reports indicate that proper level of plaque control may be achieved and maintained not only in full mouth treatments but also in all treatment cases.26 Additionally, some literatures have concluded that long-term success rate may be achieved with patients undergoing a significant periodontal tissue loss after receiving a combination treatment of periodontitis treatment and prosthetic treatment with proper and consistent maintenance case.22 Since periodontal disease is prone to relapse, maintenance and SPT are imperative for long-term maintenance of the periodontal tissues that were cured or stabilized by periodontal treatments. In various literatures, different terminologies such as supportive periodontal care (SPC) and supportive periodontal therapy (SPT) are used.27 The Japanese Society of Periodontology however differentiates maintenance from SPT. The designated meaning of maintenance is “health monitoring” to maintain the periodontal tissues for the long term, whereas SPT is a “treatment” to maintain the periodontal tissues that are symptomatically stable.28
Long-term health of periodontal tissues and stability of dentition depends on the quality and frequency of maintenance care and SPT. Reports show that without regular maintenance and SPT, the probability of losing teeth is 5 to 6 times greater than with such care.29 Therefore, prior to periodontal treatments, the patients must be well informed and understand the objective and necessity of maintenance and SPT.30 Although visible, subgingival calculus and infected tissues are difficult to remove completely with basic periodontal treatments and periodontal surgery. If subgingival biofilms are not sufficiently removed, despite the lack of clinical symptoms, continuous attachment loss would ensue. Therefore, continuous biofilm removal is imperative after completion of APT.
The American Academy of Periodontology (AAP) sets forth the following treatment approaches in its guideline for maintenance and SPT: ① update of medical and dental histories, ② evaluation of current extra- and intraoral, periodontal and peri-implant soft tissues: ③ assessment of oral hygiene status, ④ assessment of the patient’s oral hygiene, ⑤ assessment of the periodontal tissues and risk factors, ⑥ Removal of supragingival and subgingival bacterial plaque and calculus, ⑦ Re-treatment of the disease as needed. Distinction is made from daily examinations in that after-treatment care such as thorough assessment of the periodontal tissues, assessment of risk factors, mechanical debridement of plaques and calculus deposits are included.31 Additionally, making proposals of the timing for individualized maintenance and SPT are of vital importance. An appropriate time period must be established, taking into consideration systemic diseases and patient’s compliance. During the SPT period, various factors including damages to prosthetics, tooth root fractures progression of the disease in the tooth that was once determined to be preservable, aging of the patient, outbreak of systemic disease become intricately relevant. In this case, the patient had progressive periodontitis that required particular attention, and an interdisciplinary approach, including orthodontic treatment and prosthetic treatment was taken on this patient. The SPT period was set at 2 months, during which occasional inflammation was observed in the gingiva. Owing to early interventions, the patient has been maintaining well after 10 years from SPT. With continuous SPT and early intervention of acute symptoms, anchor teeth and periodontally treated teeth are likely preservable in the long term.
The authors declare no conflicts of interest associated with this manuscript.
Rathod SR, Kolte AP, Chintawar S: The dynamic relationship between pathological migrating teeth and periodontal disease. J Indian Soc Periodontol, 17(6): 762-4, 2013.
Meetu Preet Jain,Preet Rajendra Jain,Harneet Singh Chawla, et al: Pathological tooth migration-spontaneous correction of diastema after surgical periodontal therapy: a case report. Pan Afr Med J, 41:39, 2022.
Kessler M: Interrelationships between orthodontics and periodntics. American Journal of Orthodontics, 70:154-172, 1976.
Melsen B, Agerbaek N: Othodontics as an adjunct to rehabilitation. Periodontal 2000, 4: 148-159, 1994.
Panos N Papapanou, Mariano Sanz, Nurcan Buduneli, et al: Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol, 89 Suppl 1: S173-S182. 2018.
Dutzan N , Kajikawa T, Abusleme L, et al: A dysbiotic microbiome triggers TH17 cells to mediate oral mucosal immunopathology in mice and humans. Sci Transl Med, 10: eaat0797, 2018.
Alexander SA: Effects of orthodontic attachments on the gingival health of permanent second molars. Am J Orthod Dentofacial Orthop, 100: 337–340, 1991.
van Gastel J, Quirynen M, Teughels W, et al: Longitudinal changes in microbiology and clinical periodontal parameters after removal of fixed orthodontic appliances. Eur J Orthod, 33: 15–21, 2011.
Erkan M, Pikdoken L, Usumez S: Gingival response to mandibular incisor intrusion. Am J Orthod Dentofacial Orthop, 132: 143–149, 2007.
Ari-Demirkaya A, Ilhan I: Effects of relapse forces on periodontal status of mandibular incisors following orthognathic surgery. J Periodontol, 79: 2069–2077, 2008.
Sinclair PM, Berry CW, Bennett CL, et al: Changes in gingiva and gingival flora with bonding and banding. Angle Orthod, 57:271–278, 1987.
Erbe C, Heger S, Kasaj A, et al: Christina Orthodontic treatment in periodontally compromised patients: a systematic review. Clinical Oral Investigations, 27: 79-89, 2023.
Melsen B, Agerbaek N, Markenstam G: 辺縁骨損失のある成人患者における切歯の侵入. Am J Orthod Dentofacial Orthop, 96(3):232–241, 1989.
Alsulaimani L, Alqarni H, Akel M, et al: The Orthodontics-Periodontics Challenges in Integrated Treatment: A Comprehensive Review. Cureus, 15(5): e38994, 2023.
Nyman S R, Lang N P: Tooth mobility and the biological rationale for splinting teeth. Periodontol 2000, 4: 15–22, 1994.
Fardal O, Linden GJ: Long-term outcomes for cross-arch stabilizing bridges in periodontal maintenance patients—A retrospective study. J Clin. Periodontol, 37: 299–304, 2010.
S W Yi, I Ericsson, G E Carlsson, et al: Long-term follow-up of cross-arch fixed partial dentures in patients with advanced periodontal destruction, Acta Odontol Scand, 53: 242–248, 1995.
Laurell L, Lundgren D, Falk H et al: Long-term prognosis of extensive polyunit cantilevered fixed partial dentures. J Prosthet Dent, 66: 545–552, 1991.
Lundgren D: Prosthetic reconstruction of dentitions seriously compromised by periodontal disease. J Clin Periodontol, 18: 390–395, 1991.
D Lundgren, S Nyman, L Heijl, G E Carlsson: Functional analysis of fixed bridges on abutment teeth with reduced periodontal support. J Oral Rehabil,2(2): 105-16,1975.
S Kourkouta, K W Hemmings, L Laurell: Restoration of periodontally compromised dentitions using cross-arch bridges.Principles of perio-prosthetic patient management. Br Dent J, 203: 189-95. 2007.
Luigi Checchi,Marco Montevecchi,Maria Rosaria Antonella Gatto,et al: Retrospective study of tooth loss in 92 treated periodontal patients. J Clin Periodontol,29(7):651-6, 2002.
William Becker,Burton E. Becker,Lawrence E. Berg : Periodontal Treatment Without Maintenance: A Retrospective Study in 44 Patients. J Periodontol, 55(9):505-9, 1984.
Carolina Manresa, Elena C Sanz-Miralles, Joshua Twigg, et al: Supportive periodontal therapy (SPT) for maintaining the dentition in adults treated for periodontitis. Cochrane Database Syst Rev, 1(1): CD009376, 2018.
MG Newman, H Takei, PR Klokkevold, et al: Newman and Carranza’s Clinical Periodontology 13th Edication.ELSEVIER.2019.
1) Department of Operative Dentistry, Endodontology and Periodontology, School of Dentistry, Matsumoto Dental University.
2) Oral Health Science, Department of Oral Health Promotion, Oral Science Course, Matsumoto Dental University Graduate School of Oral Medicine.
3) Yamaguchi Dental Clinic,Nagano,Japan.
4) Department of Removable Partial Prosthodontics, Tokyo Dental College.
5) Asunaro Pediatric Dental Clinic, Toyama, Japan.
6) Tai Dental Clinic,Kanagawa,Japan.
7) Department of Hard Tissue Research, Graduate School of Oral Medicine, Matsumoto Dental University.
Rathod SR, Kolte AP, Chintawar S: The dynamic relationship between pathological migrating teeth and periodontal disease. J Indian Soc Periodontol, 17(6): 762-4, 2013.
Meetu Preet Jain,Preet Rajendra Jain,Harneet Singh Chawla, et al: Pathological tooth migration-spontaneous correction of diastema after surgical periodontal therapy: a case report. Pan Afr Med J, 41:39, 2022.
Kessler M: Interrelationships between orthodontics and periodntics. American Journal of Orthodontics, 70:154-172, 1976.
Melsen B, Agerbaek N: Othodontics as an adjunct to rehabilitation. Periodontal 2000, 4: 148-159, 1994.
Panos N Papapanou, Mariano Sanz, Nurcan Buduneli, et al: Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol, 89 Suppl 1: S173-S182. 2018.
Dutzan N , Kajikawa T, Abusleme L, et al: A dysbiotic microbiome triggers TH17 cells to mediate oral mucosal immunopathology in mice and humans. Sci Transl Med, 10: eaat0797, 2018.
Alexander SA: Effects of orthodontic attachments on the gingival health of permanent second molars. Am J Orthod Dentofacial Orthop, 100: 337–340, 1991.
van Gastel J, Quirynen M, Teughels W, et al: Longitudinal changes in microbiology and clinical periodontal parameters after removal of fixed orthodontic appliances. Eur J Orthod, 33: 15–21, 2011.
Erkan M, Pikdoken L, Usumez S: Gingival response to mandibular incisor intrusion. Am J Orthod Dentofacial Orthop, 132: 143–149, 2007.
Ari-Demirkaya A, Ilhan I: Effects of relapse forces on periodontal status of mandibular incisors following orthognathic surgery. J Periodontol, 79: 2069–2077, 2008.
Sinclair PM, Berry CW, Bennett CL, et al: Changes in gingiva and gingival flora with bonding and banding. Angle Orthod, 57:271–278, 1987.
Erbe C, Heger S, Kasaj A, et al: Christina Orthodontic treatment in periodontally compromised patients: a systematic review. Clinical Oral Investigations, 27: 79-89, 2023.
Melsen B, Agerbaek N, Markenstam G: 辺縁骨損失のある成人患者における切歯の侵入. Am J Orthod Dentofacial Orthop, 96(3):232–241, 1989.
Alsulaimani L, Alqarni H, Akel M, et al: The Orthodontics-Periodontics Challenges in Integrated Treatment: A Comprehensive Review. Cureus, 15(5): e38994, 2023.
Nyman S R, Lang N P: Tooth mobility and the biological rationale for splinting teeth. Periodontol 2000, 4: 15–22, 1994.
Fardal O, Linden GJ: Long-term outcomes for cross-arch stabilizing bridges in periodontal maintenance patients—A retrospective study. J Clin. Periodontol, 37: 299–304, 2010.
S W Yi, I Ericsson, G E Carlsson, et al: Long-term follow-up of cross-arch fixed partial dentures in patients with advanced periodontal destruction, Acta Odontol Scand, 53: 242–248, 1995.
Laurell L, Lundgren D, Falk H et al: Long-term prognosis of extensive polyunit cantilevered fixed partial dentures. J Prosthet Dent, 66: 545–552, 1991.
Lundgren D: Prosthetic reconstruction of dentitions seriously compromised by periodontal disease. J Clin Periodontol, 18: 390–395, 1991.
D Lundgren, S Nyman, L Heijl, G E Carlsson: Functional analysis of fixed bridges on abutment teeth with reduced periodontal support. J Oral Rehabil,2(2): 105-16,1975.
S Kourkouta, K W Hemmings, L Laurell: Restoration of periodontally compromised dentitions using cross-arch bridges.Principles of perio-prosthetic patient management. Br Dent J, 203: 189-95. 2007.
Luigi Checchi,Marco Montevecchi,Maria Rosaria Antonella Gatto,et al: Retrospective study of tooth loss in 92 treated periodontal patients. J Clin Periodontol,29(7):651-6, 2002.
William Becker,Burton E. Becker,Lawrence E. Berg : Periodontal Treatment Without Maintenance: A Retrospective Study in 44 Patients. J Periodontol, 55(9):505-9, 1984.
Carolina Manresa, Elena C Sanz-Miralles, Joshua Twigg, et al: Supportive periodontal therapy (SPT) for maintaining the dentition in adults treated for periodontitis. Cochrane Database Syst Rev, 1(1): CD009376, 2018.
MG Newman, H Takei, PR Klokkevold, et al: Newman and Carranza’s Clinical Periodontology 13th Edication.ELSEVIER.2019.
1) Department of Operative Dentistry, Endodontology and Periodontology, School of Dentistry, Matsumoto Dental University.
2) Oral Health Science, Department of Oral Health Promotion, Oral Science Course, Matsumoto Dental University Graduate School of Oral Medicine.
3) Yamaguchi Dental Clinic,Nagano,Japan.
4) Department of Removable Partial Prosthodontics, Tokyo Dental College.
5) Asunaro Pediatric Dental Clinic, Toyama, Japan.
6) Tai Dental Clinic,Kanagawa,Japan.
7) Department of Hard Tissue Research, Graduate School of Oral Medicine, Matsumoto Dental University.
初診時の全顎の平均プロービングデプス(Probing Depth:PD)は4.5mm,最大PDは10.0mm,3mm以下のPD率が43.5%,4-6mmのPD率は38.7%,7mm以上のPD率が17.9%であった.全顎の平均プロービング時の出血(Bleeding on Probing:BOP)率は42.3%,歯の動揺度は17,22,23,32,33,41,46で1度,11,12,21は2度,16,24,26,31は3度(Millerの分類)であった.また,36に1度,16(近心,遠心),26(近心,遠心),36,47に2度の根分岐部病変(Lindhe & Nymanの分類)が認められた.初診時のプラークスコア(O’LearyらのPlaque control record:PCR値)は83.9%で口腔清掃状態は不良であった(図1b).
矯正治療終了後,最終補綴物の製作を開始した.上下顎概形印象採得,フェイスボウトランスファー,チェックバイトを施行し,補綴学的診断を施行した.術前の治療計画では,上顎は全ての歯を連結するフルマウスブリッジによる補綴治療を第一選択としていたが,支台歯に平行性が認められず,かつ,すべて生活歯であったため,便宜的な抜髄処置の可能性が推察された.また,重度の歯周炎患者に対する補綴治療を考える際,特に重要である咬合負荷を全顎的に分散させるため,本症例では上顎の最終補綴処置はKey and keyway attachmentを用いた半固定性連結の設計とした.すなわち支台歯の平行性を考慮し,13・14間,22・23間でアタッチメントによる連結機構を設計した.補綴形態決定後は支台歯形成,印象採得後,コーピング試適により適合性の最終確認を行った.上顎最終補綴治療後,下顎の補綴は47から施行し47,36に全部金属冠,咬合支持のため44,45,34,35にアンレータイプの金属冠を装着した.全歯の補綴治療終了後,咬合力測定器(デンタルプレスケール®,GC,東京)にて全顎的に均等に咬合圧が付与されていることを確認した.また,クレンチング習癖があるためナイトガードの作製,装着を行い,夜間のブラキシズムに対応した.
Rathod SR, Kolte AP, Chintawar S: The dynamic relationship between pathological migrating teeth and periodontal disease. J Indian Soc Periodontol, 17(6): 762-4, 2013.
Meetu Preet Jain,Preet Rajendra Jain,Harneet Singh Chawla, et al: Pathological tooth migration-spontaneous correction of diastema after surgical periodontal therapy: a case report. Pan Afr Med J, 41:39, 2022.
Kessler M: Interrelationships between orthodontics and periodntics. American Journal of Orthodontics, 70:154-172, 1976.
Melsen B, Agerbaek N: Othodontics as an adjunct to rehabilitation. Periodontal 2000, 4: 148-159, 1994.
Panos N Papapanou, Mariano Sanz, Nurcan Buduneli, et al: Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol, 89 Suppl 1: S173-S182. 2018.
Dutzan N , Kajikawa T, Abusleme L, et al: A dysbiotic microbiome triggers TH17 cells to mediate oral mucosal immunopathology in mice and humans. Sci Transl Med, 10: eaat0797, 2018.
Alexander SA: Effects of orthodontic attachments on the gingival health of permanent second molars. Am J Orthod Dentofacial Orthop, 100: 337–340, 1991.
van Gastel J, Quirynen M, Teughels W, et al: Longitudinal changes in microbiology and clinical periodontal parameters after removal of fixed orthodontic appliances. Eur J Orthod, 33: 15–21, 2011.
Erkan M, Pikdoken L, Usumez S: Gingival response to mandibular incisor intrusion. Am J Orthod Dentofacial Orthop, 132: 143–149, 2007.
Ari-Demirkaya A, Ilhan I: Effects of relapse forces on periodontal status of mandibular incisors following orthognathic surgery. J Periodontol, 79: 2069–2077, 2008.
Sinclair PM, Berry CW, Bennett CL, et al: Changes in gingiva and gingival flora with bonding and banding. Angle Orthod, 57:271–278, 1987.
Erbe C, Heger S, Kasaj A, et al: Christina Orthodontic treatment in periodontally compromised patients: a systematic review. Clinical Oral Investigations, 27: 79-89, 2023.
Melsen B, Agerbaek N, Markenstam G: 辺縁骨損失のある成人患者における切歯の侵入. Am J Orthod Dentofacial Orthop, 96(3):232–241, 1989.
Alsulaimani L, Alqarni H, Akel M, et al: The Orthodontics-Periodontics Challenges in Integrated Treatment: A Comprehensive Review. Cureus, 15(5): e38994, 2023.
Nyman S R, Lang N P: Tooth mobility and the biological rationale for splinting teeth. Periodontol 2000, 4: 15–22, 1994.
Fardal O, Linden GJ: Long-term outcomes for cross-arch stabilizing bridges in periodontal maintenance patients—A retrospective study. J Clin. Periodontol, 37: 299–304, 2010.
S W Yi, I Ericsson, G E Carlsson, et al: Long-term follow-up of cross-arch fixed partial dentures in patients with advanced periodontal destruction, Acta Odontol Scand, 53: 242–248, 1995.
Laurell L, Lundgren D, Falk H et al: Long-term prognosis of extensive polyunit cantilevered fixed partial dentures. J Prosthet Dent, 66: 545–552, 1991.
Lundgren D: Prosthetic reconstruction of dentitions seriously compromised by periodontal disease. J Clin Periodontol, 18: 390–395, 1991.
D Lundgren, S Nyman, L Heijl, G E Carlsson: Functional analysis of fixed bridges on abutment teeth with reduced periodontal support. J Oral Rehabil,2(2): 105-16,1975.
S Kourkouta, K W Hemmings, L Laurell: Restoration of periodontally compromised dentitions using cross-arch bridges.Principles of perio-prosthetic patient management. Br Dent J, 203: 189-95. 2007.
Luigi Checchi,Marco Montevecchi,Maria Rosaria Antonella Gatto,et al: Retrospective study of tooth loss in 92 treated periodontal patients. J Clin Periodontol,29(7):651-6, 2002.
William Becker,Burton E. Becker,Lawrence E. Berg : Periodontal Treatment Without Maintenance: A Retrospective Study in 44 Patients. J Periodontol, 55(9):505-9, 1984.
Carolina Manresa, Elena C Sanz-Miralles, Joshua Twigg, et al: Supportive periodontal therapy (SPT) for maintaining the dentition in adults treated for periodontitis. Cochrane Database Syst Rev, 1(1): CD009376, 2018.
MG Newman, H Takei, PR Klokkevold, et al: Newman and Carranza’s Clinical Periodontology 13th Edication.ELSEVIER.2019.
1) Department of Operative Dentistry, Endodontology and Periodontology, School of Dentistry, Matsumoto Dental University.
2) Oral Health Science, Department of Oral Health Promotion, Oral Science Course, Matsumoto Dental University Graduate School of Oral Medicine.
3) Yamaguchi Dental Clinic,Nagano,Japan.
4) Department of Removable Partial Prosthodontics, Tokyo Dental College.
5) Asunaro Pediatric Dental Clinic, Toyama, Japan.
6) Tai Dental Clinic,Kanagawa,Japan.
7) Department of Hard Tissue Research, Graduate School of Oral Medicine, Matsumoto Dental University.
La función oral en pacientes con enfermedad periodontal sólo puede mantenerse con un control inflamatorio estricto, un posicionamiento vertical y horizontal adecuado de los maxilares y el restablecimiento de las relaciones oclusales, tal y como se tipifica en la avulsión molar con guía antelar. Sin embargo, en casos graves de periodontitis, se producen movimientos dentarios y desplazamientos patológicos debido a un alto grado de destrucción del tejido periodontal. Como resultado, el equilibrio oclusal se ve alterado y una carga excesiva más allá de la capacidad de adaptación del periodonto actúa a menudo como una oclusión traumática, dando lugar a un estado de trauma oclusal secundario y a un mayor aumento de la destrucción del tejido periodontal.
En este estudio, presentamos el caso de un paciente con periodontitis extensa justo antes del colapso oclusal, que fue tratado con un enfoque de equipo integral que incluía periodoncia, ortodoncia y prostodoncia, con la inflamación y la estabilidad oclusal como objetivos del tratamiento, y con buenos resultados y estabilidad a largo plazo.
El paciente, un hombre de 39 años, acudió al Departamento de Periodoncia del Hospital Universitario Dental de Matsumoto con la queja principal de que se le movían los dientes de toda la mandíbula. Se diagnosticó al paciente periodontitis extensa con espaciamiento interdental e irregularidades dentarias en el plexo. Posteriormente, la paciente se sometió a un tratamiento de ortodoncia para corregir la mala práctica dental y lograr la continuidad dentaria. Finalmente, el tratamiento protésico completo estableció la oclusión y se consiguió un buen entorno oral. El paciente ha estado en terapia periodontal de apoyo (SPT) durante 10 años.
Palabras clave: broad type periodontitis, malalignment of teeth, prosthetic treatment, team approach, interdisciplinary treatment
Introducción.
La periodontitis es una enfermedad inflamatoria crónica causada por la infección de la encía con bacterias comensales orales y se caracteriza por la destrucción y reabsorción del tejido conectivo gingival y el hueso alveolar, y es una enfermedad relacionada con el estilo de vida que afecta aproximadamente al 50% de los japoneses de 40 años o más.1 Por lo general, a medida que progresa la periodontitis, se producen movimientos y desplazamientos dentales patológicos en función del grado de la enfermedad. De hecho, se ha informado de que el movimiento dental patológico se produce en el 30-55,8% de los pacientes con periodontitis.2-4 En los pacientes con periodontitis avanzada, la descomposición del tejido periodontal es marcada y éste suele ser incapaz de soportar las fuerzas masticatorias y oclusales a las que era capaz de adaptarse en condiciones sanas. Las fuerzas de mordida que superan la capacidad de adaptación del periodonto actúan como una mordida traumática sobre los dientes cada vez más alterados, destruyendo el tejido periodontal. Esto actúa como un trauma oclusal secundario sobre el ligamento periodontal, provocando un mayor deterioro de la enfermedad. Incluso cuando el periodonto está sano, la maloclusión y la maloclusión pueden causar maloclusión en la relación de contacto oclusal con los dientes opuestos, dando lugar a un contacto prematuro, fuerzas laterales no deseadas y oclusión traumática, que también causa trauma oclusal primario en los tejidos periodontales sanos. Por lo tanto, la enfermedad periodontal como inflamación y la oclusión como traumatismo están relacionadas con el deterioro de ambas patologías, como causa y como consecuencia. Para la estabilidad a largo plazo del entorno oral y la prevención de la reaparición de diversos problemas, en la periodontitis con mordida traumática son esenciales no sólo el control de la inflamación, sino también la estabilidad oclusal y la distribución de las fuerzas oclusales. También es esencial el tratamiento oclusal para la periodontitis con oclusión traumática, como la estabilidad de la oclusión y la distribución de las fuerzas oclusales.
Además, los pacientes con enfermedad periodontal avanzada a menudo sufren trastornos complejos que implican caries dental, enfermedad de la pulpa dental, estética, articulaciones temporomandibulares además de la enfermedad periodontal, por lo que en muchos casos requieren un tratamiento interdisciplinar en sus planes de tratamiento que consiste en una combinación de múltiples enfoques de tratamiento, como restauración coronal, endodoncia, ortodoncia y tratamientos protésicos además del tratamiento de la periodontitis por especialistas en cada área.5-7
En este estudio, informamos de un caso de un paciente joven con periodontitis avanzada, en el que se pudo preservar un gran número de dientes mediante un tratamiento integral en una única unidad oral en colaboración con los distintos departamentos del Hospital de la Universidad Dental de Matsumoto, y que mantuvo un buen estado tras la SPT a largo plazo.
CASO
Paciente: 39 años (en el primer examen), varón
Fecha de la primera visita: junio de 2007
Queja: Movimiento dentario en toda la mandíbula
1. Antecedentes sistémicos
No hay antecedentes sistémicos.
2. Historia oral
La paciente no tenía antecedentes de caries dental ni de enfermedad periodontal y nunca antes había acudido a una clínica dental. Sin embargo, ese mismo año, se dio cuenta de que se le movían los dientes de toda la mandíbula y acudió a la sala de exploración inicial del Hospital Universitario Dental de Matsumoto (en lo sucesivo, "el hospital principal"). Debido a su apretada agenda laboral, se sometió al tratamiento de caries y a la limpieza de bolsas periodontales varias veces antes de completar el tratamiento. En 2005 (36 años), además del movimiento dental, empezó a notar sangrado gingival, halitosis y estancamiento de restos de comida en los espacios interdentales, y en junio de 2007 (39 años), visitó de nuevo esta clínica y fue remitido al Departamento de Periodoncia.
3. Antecedentes familiares
Ambos padres llevan prótesis completas superiores e inferiores desde los 65 años. El hermano, que es 5 años mayor que él, ha estado recibiendo tratamientos en un dentista cercano tras ser diagnosticado de periodontitis.
4. Estilo de vida y hábitos
El paciente tiene antecedentes de haber fumado 20 cigarrillos al día durante 5 años a los 20 años. No bebía con regularidad, pero ocasionalmente tomaba 180 ml de bebidas alcohólicas con sus compañeros de trabajo.
5. Estado actual
1) Hallazgos sistémicos
Altura de 166 cm, peso de 64,0 kg, IMC (Índice de Masa Corporal) de 23,2, complexión media, estatura media.
2) Hallazgos intraorales
(1) Resultados macroscópicos
La encía marginal no presentaba enrojecimiento ni inflamación evidentes en toda la mandíbula; no obstante, se observó cierta congestión sanguínea. La forma gingival de los dientes anteriores de la mandíbula y el maxilar era la de una gruesa repisa. Se observó una recesión gingival significativa en los dientes anteriores de la mandíbula y en el lado de la hebilla del primer molar maxilar izquierdo y derecho.El arco dental en el maxilar y la mandíbula tenía una forma parabólica. Sin embargo, se observó separación dental entre los incisivos centrales maxilares, el incisivo central maxilar derecho y el incisivo lateral, el canino y el primer premolar maxilar derecho, el canino y el primer premolar maxilar izquierdo, y apiñamiento en los incisivos centrales mandibulares (Fig.1a)
(2) Examen del tejido periodontal
En el momento de la primera visita, la PD (profundidad de sondaje) media en todo el maxilar era de 4,5 mm, la PD máxima era de 10,0 mm, el 43,5% tenía una PD de 3 mm o menos, el 38,7% de 4 a 6 mm, el 17,9% de 7 mm o más. El promedio de BOP (sangrado al sondaje) en toda la mandíbula fue del 42,3%. la movilidad de los dientes en 17, 22, 23, 32, 33, 41, 46 fue grado 1, grado 2 en 11, 12, 21, y grado 3 en 16, 24, 26, 31 (clasificación de Miller).
Además, en 36 se encontraron lesiones de bifurcación radicular (clasificación de Lindhe & Nyman) de 1er grado, 16 (proximal, centrífuga), 26 (proximal, centrífuga), 36 y 47 de 2º grado. La puntuación de placa (registro de control de placa de O'Leary et al.: valor PCR) en la primera visita era del 83,9% y la limpieza bucal era deficiente (Fig.1b).
(3) Hallazgos radiográficos
En la primera visita, los hallazgos mostraron reabsorción ósea alveolar horizontal de moderada a avanzada en toda la mandíbula, y reabsorción ósea vertical avanzada en 24, 36, 46, 47. Además, en 46, 47 había hallazgos radiolúcidos que probablemente estaban asociados con la afectación de la furcación, y en 16, 11, 26 se mostraban áreas radiolúcidas en el hueso alveolar que rodeaba el ápice radicular. Además, distalmente en 47, los hallazgos radiolúcidos mostraban caries que se extendían a la pulpa dental.(Fig.1c).
(Fig.1a) Intraoral photo taken during first visit (June 2007)
(Fig.1b) Results of periodontal tissue examination during first visit (June 2007)
(Fig.1c) Dental X-ray 14 during first visit (June 2007)
6. Prueba de anticuerpos bacterianos
Mediante la prueba de títulos de anticuerpos periodontopatógenos (DEMECAL®, Ledger Co., Ltd., Tokio), se tomaron muestras de sangre en ayunas de las yemas de los dedos 3 horas después de una comida para detectar títulos de anticuerpos de cuatro especies bacterianas: A. a (Actinobacillus actinomycetemcomitans), P. g (Porhyromonas gingivalis), P. i (Prevotella intermedia) y E. c (Eikenella corrodens). No se observó ningún aumento de los títulos de anticuerpos para las cuatro especies bacterianas, incluida A. a., que es específica de la periodontitis invasiva.
7. Causa
1) Factor de riesgo sistémico: ninguno
2) Factor de riesgo local: Placas, mala alineación de los dientes, oclusión traumática
8. Diagnóstico
Tras un examen exhaustivo que incluyó la historia clínica y el estado clínico, el paciente fue diagnosticado de periodontitis de tipo amplio en estadio Ⅳ, grado C..
9. Plan de tratamiento
Política de tratamiento
Después de mejorar el tejido periodontal mediante el tratamiento de la enfermedad periodontal, diseñamos el siguiente plan de tratamiento integral para mejorar el entorno general de la cavidad bucal mediante tratamiento de ortodoncia y tratamiento protésico.
① Examen del tejido periodontal, examen bacteriano, diagnóstico.
② Tratamiento periodontal básico (control de placa, raspado y alisado radicular: SRP, ajuste oclusal, tratamiento de extracción dental, fijación temporal, tratamiento protésico temporal)
③ Inspección de reevaluación
④ Tratamiento quirúrgico periodontal (para áreas restantes de EP)
⑤ Inspección de reevaluación
⑥ Tratamiento de recuperación de la función bucal (tratamiento de ortodoncia, tratamiento protésico)
⑦ Inspección de reevaluación
⑧ SPT (terapia periodontal de apoyo)
Se elaboró el plan de tratamiento anterior y se inició el tratamiento tras obtener el consentimiento de la paciente. Se informó verbalmente a la paciente sobre la publicación de este caso y los datos clínicos, y se obtuvo su consentimiento por escrito.
10. Curso del tratamiento (Fig. 2)
1) Tratamiento periodontal básico
Se informó al paciente de que el movimiento de la mandíbula no sólo se debía a la reabsorción ósea alveolar, sino también a una periodontitis causada por una higiene bucal deficiente, y se inició el control de la placa con un cepillo de dientes manual. Dado que el valor de PCR en la visita inicial era deficiente (83,9%), se instruyó al paciente para que se cepillara los dientes con un cepillo manual (Butler #211, Sunstar Co., Ltd., Osaka, Japón) y con el método de fregado, y una vez observada la mejoría en las caras labial y lingual, se aplicó a las superficies adyacentes un cepillo interdental con un tamaño adecuado para el espacio entre los dientes (Una vez observada la mejoría de las caras labial y lingual, se instruyó en el uso de cepillos interdentales de diferentes tamaños (DENT EX® 3M, cepillos interdentales S, M, L, Lion Corporation, Tokio) según el espacio de las superficies interdentales adyacentes. Llevó tiempo mejorar el efecto del cepillado debido a la posición gingival marginal desigual, la inclinación desigual del eje del diente, la retracción gingival y el cambio de posición gingival tras la extracción del diente, pero el valor de PCR disminuyó al 18,3% en la 14ª sesión de enseñanza y se ha mantenido en un nivel casi bueno desde entonces, aunque ha fluctuado ligeramente. El valor de PCR disminuyó hasta el 18,3% en la 14ª sesión de enseñanza y se ha mantenido en un nivel casi bueno desde entonces, aunque ha fluctuado ligeramente.
(Fig.2) Treatment process
Después de reducir la placa supragingival mediante el cepillado de autocuidado, se aplicó SRP como cuidado profesional en el área de los molares y pequeños del lado superior izquierdo, en el área de los molares y pequeños del lado superior derecho, en el área anterior del maxilar, en el área de los molares y pequeños del lado derecho mandibular y en el área de los molares y pequeños del lado superior derecho. área anterior mandibular El procedimiento se realizó en las áreas pequeñas y molares del lado izquierdo de la mandíbula para eliminar el cálculo subgingival y promover la inserción gingival alisando la superficie de la raíz del diente. Además, al finalizar el primer ciclo de SRP, se detectó la presencia de sarro residual debajo del margen gingival en toda la mandíbula, lo que llevó a la realización de otro SRP completo. Sin embargo, en febrero de 2008 (a los 40 años de edad), el diente 16, en mayo del mismo año el diente 26, en febrero de 2009 (a los 41 años de edad) el diente 24, y en abril del mismo año el diente 11, mostraron una pérdida de la inserción persistente a pesar del tratamiento periodontal básico, lo que llevó al diagnóstico de no ser viable su preservación y se procedió con su extracción. Para el área defectuosa después del procedimiento de extracción del diente, utilizamos prótesis temporales tipo puente 23-27 con 23, 25 y 27 como pilares, y prótesis temporales tipo puente con 13, 14, 15 y 17 como pilares. Se instaló el dispositivo protésico 12-22 con los dispositivos protésicos 12, 21 y 22 como pilares.
Durante el tratamiento periodontal básico, se prestó atención a los traumatismos oclusales desde una fase temprana, y se procedió al tallado y ajuste oclusal para eliminar el contacto prematuro y las interferencias oclusales. Por último, se conectaron todas las unidades y se estabilizó cada diente teniendo en cuenta la estética, el grado de destrucción del tejido periodontal en los dientes vecinos y el futuro tratamiento protésico con coronas. En junio de 2007, paralelamente al tratamiento periodontal, se inició un tratamiento de conductos radiculares infectados en 47 dientes, y se colocó una prótesis provisional tras obturar el conducto radicular.
2) Examen de reevaluación (febrero de 2010)
En el examen de reevaluación tras el tratamiento periodontal básico, la encía mejoró a un color rosa salmón y desaparecieron los hallazgos inflamatorios de la encía marginal, principalmente la congestión. En general, se observó una recesión gingival de clase 4 (clasificación de Miller de la recesión gingival) (Fig.3a).
La PD media de toda la mandíbula fue de 2,8 mm, la PD máxima fue de 10,0 mm, la tasa de PD de 3 mm o menos fue del 84,0%, la tasa de PD de 4-6 mm fue del 12,5%, la tasa de PD de 7 mm o más fue del 3,5% y la tasa de BOP mejoró hasta el 11,8%. Sin embargo, seguían existiendo PD de 7,0 mm en 17, 10,0 mm en 27, 5,0 mm en 36 y 7,0 mm en 46 dientes. Además, había lesiones residuales de bifurcación radicular de un grado en el lado bucolingual de 36, de dos grados en el lado bucal casi central de 17 y en el lado bucal de 27. El grado de movilidad dentaria era de un grado en 44 y 46 (Fig.3b).
Las radiografías intraorales mostraron que se había eliminado el sarro subgingival tanto en el maxilar superior como en el inferior y que el nivel óseo alveolar no había mejorado, aunque la línea dura alveolar era clara (Fig.3c).
(Fig.3a) Intraoral photo after completion of basic periodontal treatment has completed (2010.1)
(Fig.3b) Reevaluation and examination after completion of basic periodontal treatment (January 2010)
(Fig.3c) Dental X-ray 14 after completion of basic periodontal treatment (January 2010)
3) Tratamiento quirúrgico periodontal
Tras el examen de reevaluación posterior a la finalización del tratamiento periodontal básico, se detectaron bolsas periodontales profundas y dos lesiones radiculares residuales en 17 y 27, por lo que en abril de 2010 (42 años) se realizó una terapia de regeneración tisular periodontal con una proteína de matriz de esmalte en 17 (Fig.4), y en junio de 2010 se realizó un curetaje de exfoliación gingival y una cirugía centrífuga de cuña en 27 (Fig.5). En el resto de las localizaciones de PD en las caras linguales 36 y 46, optamos por estabilizar la enfermedad con SRP porque no había suficiente encía queratinizada.
(Fig.4) Enamel matrix proteins were applied in a procedure for periodontal regeneration in the maxillary left molar (April 1, 2020)
(Fig.5) Gingival flap operation and distal wedge procedure were performed on the maxillary left second molar (June 2010)
4) Pruebas de reevaluación (febrero de 2011)
En la prueba de reevaluación después de la cirugía periodontal, quedaban 4 mm de PD en el lado palatino, distalmente en 17 y en la zona media bucal en 27. La BOP ya no estaba presente y la afectación furcal mejoró. La BOP ya no estaba presente y la afectación de la furcación mejoró.
5) Tratamiento de ortodoncia de los dientes anteriores mandibulares
6 meses después de finalizar el tratamiento quirúrgico periodontal, los ortodoncistas de este hospital iniciaron el tratamiento ortodóncico para mejorar el apiñamiento de los dientes anteriores mandibulares. En octubre de 2010 (a la edad de 42 años), se realizó un examen preoperatorio, y para mejorar en primer lugar el desequilibrio de los músculos periorales, se inició la MFT (Terapia Mio Funcional). En diciembre de 2010, bajo el diagnóstico de plexo en los dientes anteriores mandibulares, se ajustaron las bandas 36 y 46 y se colocaron plaquetas en los dientes 34, 33, 32, 31, 41, 42, 43 y 44, y se inició el enderezamiento de los mismos. A partir de entonces, los alambres se ajustaron cada mes. Tras 1 año y 4 meses de tratamiento ortodóncico dinámico, se tomó una impresión del aparato de retención en abril de 2012 (a la edad de 44 años), y se colocó el aparato de retención intercanino (retenedor FSW) en mayo de 2012.
6) Tratamiento protésico
Una vez finalizado el tratamiento ortodóncico, se inició la fabricación de la prótesis definitiva. El diagnóstico protésico se realizó mediante la toma de impresiones de los contornos maxilar y maxilar, transferencias de arco facial y mordidas de control. En el plan de tratamiento preoperatorio, la primera opción de tratamiento protésico para el maxilar era un puente bucal completo que uniera todos los dientes, pero debido a que los dientes pilares no mostraban paralelismo y eran todos dientes vivos, se dedujo la posibilidad de un procedimiento de extracción pulpar por conveniencia. Con el fin de distribuir la carga oclusal por toda la mandíbula, lo cual es especialmente importante cuando se considera el tratamiento protésico de pacientes con periodontitis severa, el tratamiento protésico final del maxilar en este caso se diseñó como una conexión semifija utilizando el aditamento de chaveta y chavetero. En otras palabras, teniendo en cuenta el paralelismo de los dientes pilares, se diseñó un mecanismo de conexión de fijación entre 13 y 14 y entre 22 y 23. Una vez determinada la forma protésica, se formaron los dientes pilares, se tomaron impresiones y se confirmó el ajuste final mediante un ajuste de cofia. Tras el tratamiento protésico definitivo del maxilar superior, se llevó a cabo el tratamiento protésico de la mandíbula a partir del 47, con coronas totalmente metálicas en 47 y 36 y coronas metálicas tipo relé en 44, 45, 34 y 35 para soporte oclusal. Una vez finalizado el tratamiento protésico de todos los dientes, se confirmó mediante un instrumento de medición de la fuerza oclusal (Dental Prescale®, GC, Tokio) que la presión oclusal se aplicaba de forma uniforme en todos los maxilares. Se confeccionó y ajustó un protector nocturno para su hábito de apretar los dientes con el fin de hacer frente a su bruxismo nocturno.
7) Examen de reevaluación (diciembre de 2013).
En el examen de reevaluación después del tratamiento para restablecer la función oral, la encía era de color rosa salmón y se reprodujo la armonía oral mediante un aparato protésico estética y funcionalmente armonioso (Fig. 6a). La PD media de toda la mandíbula era de 2,1 mm, la PD máxima era de 4,0 mm, la tasa de PD por debajo de 3 mm era del 99,3%, y la enfermedad del tejido periodontal era estable sin BOP (Fig.6b). Radiográficamente, se reprodujo la continuidad de la línea dura alveolar y la alineación de los haces óseos era normal, por lo que el paciente fue transferido a SPT (Fig. 6c).
(Fig.6a) Intraoral photo after completion of restoration of oral function was completed(2013.4)
(Fig.6b) Reevaluation and examination after completion of restoration of oral function (April 2013)
(Fig.6c) Digital X-ray 14 after completion of restoration of oral function (April 2013)
8)SPT (a partir de diciembre de 2013).
Tras la transición a SPT, el paciente se cepilló 4 veces al día después de cada comida y antes de acostarse y ha seguido utilizando un cepillo interdental. Los niveles de PCR han estado constantemente en el rango del 20%. SPT , que consiste principalmente en instrucciones sobre el cepillado y la limpieza de la superficie dental, se ha aplicado cada dos meses hasta la actualidad, y se hacen esfuerzos para mantener y gestionar la higiene bucal a largo plazo para garantizar que el control de la placa no sea insuficiente. Aunque se observa una decoloración menor en las prótesis, el color de la encía es rosa salmón y se ha mantenido un aspecto macroscópicamente sano (Fig.7a). La PD media en toda la mandíbula es de 2,1mm, la PD máxima es de 4,0mm, la proporción de PD de 3mm o menos es del 99,3%. No se ha encontrado BOP y la condición del tejido periodontal ha sido estable (Fig.7b). En la radiografía, la continuidad de la línea dura alveolar se ha replicado y la secuencia de las trabéculas óseas ha sido normal (Fig.7c).
(Fig.7a) Intraoral photo: 15 years after first visit (December 2022)
(Fig.7b) Examination for reevaluation: 15 years after first visit (December 2022)
(Fig.7c) 15 years after first visit: dental X-ray 14 (December 2022)
Discusión.
La enfermedad periodontal es una enfermedad infecciosa crónica causada por bacterias orales endémicas, y factores del huésped como los mecanismos de defensa, las enfermedades sistémicas, la edad, la genética y factores ambientales como el estrés, el tabaquismo y los fármacos afectan a la progresión de la enfermedad, dificultando el mantenimiento de la función oral durante y después del tratamiento dinámico. En la periodontitis avanzada, la progresión de las lesiones va acompañada de un alto grado de destrucción del tejido periodontal y de una reducción de la capacidad de soporte del tejido periodontal. Esto se traduce en la incapacidad de soportar las fuerzas oclusales y masticatorias adaptables en condiciones sanas, y a menudo se complica con traumatismos oclusales. En estos casos, además del tratamiento periodontal dirigido a eliminar los factores inflamatorios y mejorar las lesiones, es necesario un tratamiento integral dirigido a la reconstrucción oclusal para estabilizar la oclusión. Por lo tanto, se requiere una evaluación y un tratamiento adecuados en cada fase, incluyendo el tratamiento periodontal básico principalmente para el control de la placa, el tratamiento quirúrgico periodontal basado en los resultados de los exámenes de reevaluación posteriores, el tratamiento para restaurar la función oral teniendo en cuenta el trauma oclusal secundario, y el mantenimiento del SPT y de las relaciones oclusales, que son los más importantes para un pronóstico estable a largo plazo. Los factores más importantes para un pronóstico estable a largo plazo son el SPT y el mantenimiento de la relación oclusal.
1) En este caso, en el momento de la primera visita, el paciente tenía 39 años con una queja principal de movilidad de los dientes en toda la mandíbula. Se trataba de un paciente con periodontitis de tipo amplio y, dado que en las radiografías intraorales se observaba una reabsorción ósea horizontal de moderada a avanzada, era necesario eliminar la inflamación de los tejidos periodontales, controlar la progresión de la enfermedad, mantener la estabilidad oclusal y restaurar la estética, así como llevar a cabo un tratamiento interdisciplinar que incluyera el tratamiento de la periodontitis, el tratamiento ortodóncico y el tratamiento protésico. Además, para preservar de forma estable la funcionalidad y la estética del sistema estomatognático que se lograron como resultado de un tratamiento interdisciplinario, se deben controlar las inflamaciones (periodontitis) y la oclusión traumática. Por lo tanto, la terapia periodontal de apoyo (TPE) debe aplicarse de forma continua a intervalos adecuados para cada caso con el fin de alcanzar los objetivos del tratamiento y mantener el bienestar del paciente.
1) Diagnóstico de la enfermedad periodontal
El diagnóstico utilizado en este estudio se basa en la nueva clasificación propuesta a partir de 2023, es decir, la nueva clasificación de la enfermedad periodontal publicada por la AAP/EFP durante EuroPerio 9 en Ámsterdam en junio de 2018. La diferencia entre la nueva clasificación y la antigua es que la periodontitis se había dividido en dos categorías principales, periodontitis invasiva y periodontitis crónica, pero la nueva clasificación combina estas dos categorías en una sola periodontitis e introduce un marco diagnóstico de etapas y grados. En este caso, la profundidad de sondaje (PPD) era de más de 6 mm en el momento del examen inicial, se observó una reabsorción ósea vertical de más de 3 mm y dos lesiones de bifurcación radicular, y finalmente se extrajeron cuatro dientes, pero como era necesario un tratamiento protésico completo, se asignó al caso el estadio IV. El estadio C se asignó porque el % de reabsorción ósea/edad, que es el principal factor de la tasa de progresión de la enfermedad, era superior a 1,0 y se observó una rápida progresión. En otras palabras, el paciente fue diagnosticado como estadio IV grado C según la nueva clasificación de la enfermedad periodontal de acuerdo con las normas internacionales.8
2) Tratamiento periodontal básico
La enfermedad periodontal es el resultado de un aumento de la cantidad de placa dental (biofilm dental), que es un agregado de bacterias orales, y de una composición cualitativa anormal (disbiosis).9 La inflamación de los tejidos periodontales se produce como resultado del crecimiento de bacterias periodontopatógenas, principalmente bacterias anaerobias Gram-negativas como Porphyromonas gingivalis, y del crecimiento de placa subgingival. El crecimiento de bacterias periodontopatógenas, principalmente bacterias anaerobias Gram negativas como Porphyromonas gingivalis, provoca la inflamación del tejido periodontal, la formación de bolsas periodontales y el crecimiento de placa subgingival. En vista de ello, la mejora de la limpieza y el control de la inflamación gingival se consideran una de las condiciones esenciales para la estabilidad a largo plazo durante y después del tratamiento dinámico. Sin embargo, en la enfermedad periodontal avanzada se producen cambios morfológicos como bolsas periodontales profundas con reabsorción ósea alveolar, recesión gingival y movimiento dentario patológico, y se pierde la continuidad de cada tejido, convirtiéndose estas zonas en nuevos factores de retención de placa, lo que hace que la enfermedad se agrave, dando lugar a un círculo vicioso que se repite. Afortunadamente, en este caso no faltaban dientes y se mantenía la continuidad de la dentición, por lo que el control de placa se realizó en el margen gingival con un cepillo manual y un cepillo interdental adecuado al tamaño de los espacios interdentales, como es habitual. El paciente presentaba un valor de PCR deficiente del 83,9% en la primera visita, pero tras 14 sesiones de cepillado, el valor de PCR se redujo a menos del 20%. El tratamiento ortodóncico mejoró las irregularidades dentales y el entorno de limpieza bucal, y el mantenimiento y la gestión continuos del entorno bucal también contribuyeron a los buenos resultados.
El trauma oclusal secundario es un factor de riesgo local para la enfermedad periodontal, y es necesario realizar un ajuste oclusal según el estado clínico. En principio, a excepción de la abrasión de primeros auxilios, los ajustes oclusales en pacientes con enfermedad periodontal deben realizarse después de eliminar la inflamación. Esto se debe a que el movimiento de los dientes en pacientes con enfermedad periodontal puede estar causado y potenciado por la inflamación del ligamento periodontal, y los dientes pueden moverse tras la eliminación de la inflamación, dando lugar a otro traumatismo oclusal. En el presente caso, había un alto grado de reabsorción ósea alveolar en todos los maxilares y casi todos los dientes presentaban un trauma oclusal secundario. En los molares anteriores mandibulares y maxilares, en los que los dientes sobresalían y se movían, se rasuraron los puntos de contacto en una fase temprana durante el tratamiento periodontal básico para reducir la nocividad de la oclusión traumática, y se redujo la inflamación mediante SRP, etc. Después de extraer los dientes que no podían responder al tratamiento y de colocar secuencialmente un aparato protésico temporal, se observó el trauma oclusal secundario y se comprobó constantemente la flemitis. Se ajustó la mordida del paciente para que se guiara por la función de grupo de los caninos a los premolares durante el ajuste oclusal y el movimiento lateral, al tiempo que se comprobaba constantemente el fremitus.
3) Tratamiento de ortodoncia
Este caso de un paciente fue tratado con ortodoncia para mejorar el plexo de los dientes anteriores mandibulares durante el periodo de tratamiento de restauración de la función oral. El tratamiento de ortodoncia es un método muy eficaz de mejora estética y funcional en adultos. Sin embargo, el tratamiento de ortodoncia en adultos suele ir asociado a problemas como caries, enfermedad pulpar, enfermedad periodontal y pérdida de dientes. Además, también pueden padecer enfermedades sistémicas, que requieren una mayor consideración y conocimientos multidisciplinares.10 Un conocimiento profundo de la ortodoncia y la periodoncia es esencial a la hora de tratar a estos pacientes. La gestión de los tejidos periodontales es necesaria en todas las fases del tratamiento, desde el diagnóstico ortodóncico hasta la evaluación periodontal durante el tratamiento, el control de la placa y la evaluación postoperatoria.
Los estudios han demostrado que el tratamiento ortodóncico no afecta negativamente al tejido periodontal cuando la inflamación gingival está bajo control.11 Aunque los aparatos de ortodoncia fijos pueden crear barreras que comprometan la higiene oral y provoquen la retención de placa,12,13 se ha observado que un cuidado dental exhaustivo durante el tratamiento ortodóncico reduce los cambios adversos, como la hemorragia gingival14-15 y el volumen de placa.14-16 Por lo tanto, el tratamiento ortodóncico sólo debe realizarse cuando la enfermedad periodontal activa esté bajo control. En informes recientes se ha llegado al consenso de que debe garantizarse el establecimiento y mantenimiento de un estado del tejido periodontal libre de inflamación durante y después del tratamiento ortodóncico.17 Además, el tratamiento ortodóncico cuando el ligamento periodontal está comprometido debe seguir aplicando fuerzas ligeras de 5 g a 15 g.18 Por lo tanto, en el tratamiento ortodóncico en pacientes con enfermedad periodontal, es importante aplicar una fuerza ortodóncica adecuada según el grado de tejido periodontal residual.
En el presente caso, además de la estabilización de la afección mediante el tratamiento periodontal básico, los hallazgos radiográficos mostraron que los cambios orgánicos en el hueso alveolar tras el tratamiento ortodóncico, como la reabsorción radicular anómala y la reabsorción ósea alveolar, no habían progresado en comparación con el examen inicial, ni se había producido una expansión significativa del lumen periodontal, y en algunas zonas el nivel óseo alveolar había mejorado y el espacio del ligamento periodontal no se había ampliado de forma significativa. La reabsorción ósea alveolar no había avanzado en comparación con el examen inicial y no había una ampliación significativa del espacio del ligamento periodontal. Esto se debió probablemente a las fuerzas ortodóncicas apropiadas durante el tratamiento ortodóncico. Durante el tratamiento ortodóncico, el periodoncista examinó mensualmente al paciente para comprobar el control de la placa, el contacto prematuro durante el tratamiento dinámico, la interferencia oclusal y el ajuste oclusal en caso necesario. El enfoque integrado de la ortodoncia y la periodoncia es útil y contribuye a una planificación cualitativa, funcional y estética ideal, especialmente en casos clínicos complejos, y puede conducir a un plan de tratamiento óptimo.19
(5) Tratamiento protésico
A la hora de seleccionar y diseñar el tratamiento protésico definitivo en este caso, se consideraron las prótesis dentales, los implantes y los puentes corona. En primer lugar, la paciente no optó por una dentadura postiza desde el momento de la prótesis provisional en el momento del tratamiento periodontal básico. A continuación, se consideró la colocación de implantes en los premolares y molares maxilares, pero la cantidad de hueso alveolar era baja en todas las zonas, lo que requería elevaciones de seno, injertos óseos y cirugía plástica periodontal posterior, y existía riesgo de oclusión traumática causada por los implantes debido al equilibrio óseo alveolar de los dientes que se iban a tratar con implantes. El paciente no deseaba colocarse implantes debido al tiempo y al coste del tratamiento.
En los pacientes con dientes alterados debido a una reabsorción ósea alveolar grave, si no se observa ningún efecto del tratamiento con el ajuste oclusal, la modificación de la morfología de la corona o la fijación temporal, es necesario desarrollar un plan de tratamiento que considere la fijación temporal o permanente con una amplia gama de dispositivos de tratamiento periodontal. En el presente caso, como se observó un alto grado de reabsorción ósea alveolar en el maxilar, se planificó realizar la restauración maxilar definitiva con un dispositivo protésico fijo de arcada cruzada para distribuir la carga masticatoria de forma más adecuada a lo largo de toda la arcada en lugar de unidades individuales y evitar la sobrecarga de los dientes pilares debido a la reducción del soporte periodontal. Se ha informado de que los puentes fijos con un diseño de arcada cruzada proporcionan cierta rigidez y distribuyen más adecuadamente la carga masticatoria a lo largo de toda la arcada en lugar de unidades individuales, evitando así la sobrecarga de los dientes pilares debido a un menor soporte del tejido periodontal.20,21 También se ha informado de que cuando la infección periodontal está controlada, incluso si el soporte óseo alveolar original es del 20-30%, el diente pilar puede funcionar adecuadamente.22-24
6) Mantenimiento y SPT
Los informes de seguimiento a largo plazo sugieren que si los tejidos periodontales son estables y se introduce el SPT para prevenir la recidiva de la periodontitis, un diente con un soporte deficiente de los tejidos periodontales puede anclar una prótesis fija que cubra un amplio rango,24,25 lo cual es un factor de vital importancia en el cumplimiento del paciente que conduce al éxito a largo plazo, además del sistema de recuerdo dental individualizado. Estos informes indican que el nivel adecuado de control de la placa se puede lograr y mantener no sólo en los tratamientos de boca completa, sino también en todos los casos de tratamiento.26 Además, algunas literaturas han llegado a la conclusión de que la tasa de éxito a largo plazo se puede lograr con los pacientes que sufren una pérdida significativa de tejido periodontal después de recibir un tratamiento combinado de tratamiento de la periodontitis y el tratamiento protésico con el caso de mantenimiento adecuado y coherente.22 Dado que la enfermedad periodontal es propensa a la recidiva, el mantenimiento y la SPT son imperativos para el mantenimiento a largo plazo de los tejidos periodontales que fueron curados o estabilizados por los tratamientos periodontales. En diversas literaturas, se utilizan diferentes terminologías, como cuidados periodontales de apoyo (SPC) y terapia periodontal de apoyo (SPT).27 Sin embargo, la Sociedad Japonesa de Periodoncia diferencia el mantenimiento de la TPE. El significado designado de mantenimiento es "supervisión de la salud" para mantener los tejidos periodontales a largo plazo, mientras que SPT es un "tratamiento" para mantener los tejidos periodontales que son sintomáticamente estables.28
La salud periodontal y la estabilidad dental a largo plazo dependen de la calidad y la frecuencia del mantenimiento y la fisioterapia. Se ha demostrado que el riesgo de pérdida de dientes es de cinco a seis veces mayor en los pacientes que no reciben un mantenimiento y un TSP regulares que en los que sí los reciben.29 Por lo tanto, el propósito y la necesidad del mantenimiento y la fisioterapia deben ser bien explicados y comprendidos por el paciente antes del tratamiento periodontal.30 Es difícil eliminar por completo el sarro subgingival y el tejido infectado, incluso en zonas que pueden visualizarse directamente mediante un tratamiento periodontal básico o procedimientos quirúrgicos periodontales. Si no se elimina suficientemente el biofilm subgingival, se induce una pérdida persistente de inserción a pesar de la ausencia de síntomas clínicos. Por lo tanto, es importante eliminar el biofilm de forma continuada una vez finalizado el APT.
Como punto de tratamiento durante los mantenimientos y SP, La Academia Americana de Periodoncia (AAP) establece los siguientes enfoques de tratamiento en su guía para el mantenimiento y SPT: ① actualización de los historiales médicos y dentales, ② evaluación de los tejidos blandos extraorales e intraorales, periodontales y periimplantarios actuales: ③ evaluación del estado de higiene oral, ④ evaluación de la higiene oral del paciente, ⑤ evaluación de los tejidos periodontales y de los factores de riesgo, ⑥ eliminación de la placa bacteriana supragingival y subgingival y del cálculo, ⑦ retratamiento de la enfermedad según sea necesario. Se distingue de los exámenes diarios en que se incluyen los cuidados posteriores al tratamiento, como la evaluación exhaustiva de los tejidos periodontales, la evaluación de los factores de riesgo, el desbridamiento mecánico de las placas y los depósitos de cálculo.31
También es muy importante sugerir un periodo de mantenimiento y SPT adecuado para cada paciente individual. Debe fijarse en un periodo adecuado32 teniendo en cuenta la enfermedad sistémica y el cumplimiento del paciente.
Durante el periodo de SPT intervienen diversos factores de forma compleja, como la rotura de la prótesis, la fractura radicular, el deterioro de los dientes considerados salvables, el propio envejecimiento del paciente y el desarrollo de enfermedades sistémicas. El presente caso de un paciente con periodontitis grave y tratamiento integral que incluía ortodoncia y prótesis requería una atención especial: el periodo de SPT se fijó en 2 meses, y aunque se observó inflamación gingival varias veces durante el periodo de SPT, el paciente se mantuvo en buen estado 10 años después del SPT mediante tratamiento precoz. El SPT continuado y el tratamiento precoz de los síntomas agudos pueden conducir a la conservación a largo plazo incluso de los dientes pilares cargados y de los dientes tratados ortodóncicamente.
No hay conflictos de intereses que revelar en relación con este artículo.
Rathod SR, Kolte AP, Chintawar S: The dynamic relationship between pathological migrating teeth and periodontal disease. J Indian Soc Periodontol, 17(6): 762-4, 2013.
Meetu Preet Jain,Preet Rajendra Jain,Harneet Singh Chawla, et al: Pathological tooth migration-spontaneous correction of diastema after surgical periodontal therapy: a case report. Pan Afr Med J, 41:39, 2022.
Kessler M: Interrelationships between orthodontics and periodntics. American Journal of Orthodontics, 70:154-172, 1976.
Melsen B, Agerbaek N: Othodontics as an adjunct to rehabilitation. Periodontal 2000, 4: 148-159, 1994.
Panos N Papapanou, Mariano Sanz, Nurcan Buduneli, et al: Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol, 89 Suppl 1: S173-S182. 2018.
Dutzan N , Kajikawa T, Abusleme L, et al: A dysbiotic microbiome triggers TH17 cells to mediate oral mucosal immunopathology in mice and humans. Sci Transl Med, 10: eaat0797, 2018.
Alexander SA: Effects of orthodontic attachments on the gingival health of permanent second molars. Am J Orthod Dentofacial Orthop, 100: 337–340, 1991.
van Gastel J, Quirynen M, Teughels W, et al: Longitudinal changes in microbiology and clinical periodontal parameters after removal of fixed orthodontic appliances. Eur J Orthod, 33: 15–21, 2011.
Erkan M, Pikdoken L, Usumez S: Gingival response to mandibular incisor intrusion. Am J Orthod Dentofacial Orthop, 132: 143–149, 2007.
Ari-Demirkaya A, Ilhan I: Effects of relapse forces on periodontal status of mandibular incisors following orthognathic surgery. J Periodontol, 79: 2069–2077, 2008.
Sinclair PM, Berry CW, Bennett CL, et al: Changes in gingiva and gingival flora with bonding and banding. Angle Orthod, 57:271–278, 1987.
Erbe C, Heger S, Kasaj A, et al: Christina Orthodontic treatment in periodontally compromised patients: a systematic review. Clinical Oral Investigations, 27: 79-89, 2023.
Melsen B, Agerbaek N, Markenstam G: 辺縁骨損失のある成人患者における切歯の侵入. Am J Orthod Dentofacial Orthop, 96(3):232–241, 1989.
Alsulaimani L, Alqarni H, Akel M, et al: The Orthodontics-Periodontics Challenges in Integrated Treatment: A Comprehensive Review. Cureus, 15(5): e38994, 2023.
Nyman S R, Lang N P: Tooth mobility and the biological rationale for splinting teeth. Periodontol 2000, 4: 15–22, 1994.
Fardal O, Linden GJ: Long-term outcomes for cross-arch stabilizing bridges in periodontal maintenance patients—A retrospective study. J Clin. Periodontol, 37: 299–304, 2010.
S W Yi, I Ericsson, G E Carlsson, et al: Long-term follow-up of cross-arch fixed partial dentures in patients with advanced periodontal destruction, Acta Odontol Scand, 53: 242–248, 1995.
Laurell L, Lundgren D, Falk H et al: Long-term prognosis of extensive polyunit cantilevered fixed partial dentures. J Prosthet Dent, 66: 545–552, 1991.
Lundgren D: Prosthetic reconstruction of dentitions seriously compromised by periodontal disease. J Clin Periodontol, 18: 390–395, 1991.
D Lundgren, S Nyman, L Heijl, G E Carlsson: Functional analysis of fixed bridges on abutment teeth with reduced periodontal support. J Oral Rehabil,2(2): 105-16,1975.
S Kourkouta, K W Hemmings, L Laurell: Restoration of periodontally compromised dentitions using cross-arch bridges.Principles of perio-prosthetic patient management. Br Dent J, 203: 189-95. 2007.
Luigi Checchi,Marco Montevecchi,Maria Rosaria Antonella Gatto,et al: Retrospective study of tooth loss in 92 treated periodontal patients. J Clin Periodontol,29(7):651-6, 2002.
William Becker,Burton E. Becker,Lawrence E. Berg : Periodontal Treatment Without Maintenance: A Retrospective Study in 44 Patients. J Periodontol, 55(9):505-9, 1984.
Carolina Manresa, Elena C Sanz-Miralles, Joshua Twigg, et al: Supportive periodontal therapy (SPT) for maintaining the dentition in adults treated for periodontitis. Cochrane Database Syst Rev, 1(1): CD009376, 2018.
MG Newman, H Takei, PR Klokkevold, et al: Newman and Carranza’s Clinical Periodontology 13th Edication.ELSEVIER.2019.