1) The Nippon Dental University, School of Life Dentistry, Department of Periodontology
2) Wada Dental Clinic
3) Meikai University School of Dentistry, Division of Dental Biomaterials Science,Department of Restorative and Biomaterials Sciences
4) Heartful Dental Clinic
5) Aoba Dental Clinic
6) Matsumoto dental university department of Dental science and materials
7) Mieji Dental Clinic
8) Iryo Hojin Shikyoukai, Yabuki Dental Clinic
9) Fukuda Dental Clinic
Background: Teeth with furcation involvement are generally said to have poor prognosis, which in many cases, treatment is difficult to administer. This study was conducted with the objective of evaluating non-surgical periodontal therapy on furcation involvement retrospectively.
Methods: 133 molars of 80 stage 3-4 periodontitis patients, ages averaging 56±10.6 with furcation involvement, were subjected to this study. All of these patients have completed non-surgical periodontal therapy. Single root tooth surfaces or molar flat surfaces that were similar to the pre-treatment condition of the study tooth surfaces were used as the control group. Full-mouth periodontal examinations, which included those for furcation involvement and oral hygiene instructions were performed on all patients. Additionally, supragingival scaling, subgingival debridement, and reassessments were performed on all patients. Comparison was made between the preoperative and postoperative degree of furcation involvement. Probing pocket depth, bleeding on probing and plaque formation of tooth surfaces were compared with those of the control group.
Results: After the initial periodontal therapy was performed, furcation closure was observed in 20% of the degree I cases, only in 3.5% of degree II cases and no closure in degree III cases. 20% of the degree III furcation involvement cases improved to degree II levels or below. Mean PPD on tooth surface with furcation involvement improved by 0.7mm, showing a significant difference from that of the control group that improved by 1.2mm on average. In degree I and degree II cases, no significant differences in improvement of clinical parameter as compared to the control group. No significant improvement was observed in degree III cases. Especially in areas with pretreatment PPD of 6mm or more, significant difference from that of the control group was observed in degree III cases only.
Conclusion: While non-surgical periodontal treatment had limited effect on furcation closure, clinical parameter improvement was found in non-degree III cases. Therefore, non-surgical periodontal treatment would be a valid approach as the initial step in the treatment of furcation involvement.
Key words:non-surgical periodontal therapy, furcation involvement, retrospective study
I. Introduction
Periodontitis is a chronic disease induced by biofilm formation on the surface of the teeth. Therefore, biofilm removal from the tooth surfaces would be the primary therapeutic approach, thereby removing the cause of the disease. At the beginning of the treatment, oral hygiene instructions would be provided, and subgingival debridement would be performed, which would yield positive results on a substantially greater number of single rooted teeth.1,2 Minimal improvements have however been reported on clinical parameters of probing pocket depth (PPD) and clinical attachment level (CAL) of multi-rooted teeth.3 The complex anatomy of the furcation area of molars poses a challenge for complete elimination of deposits and is additionally reported to lead to inferior treatment results compared to those for smoother surfaces.4-7
In such circumstances, root-resective therapy has been widely employed and non-surgical periodontal therapy and access flap procedures were deemed to be insufficient. Studies have however shown that such treatments do not improve the long-term prognosis of in every case.8 In significant number of cases, root fracture, endodontic lesion and loss of retention of the prosthesis have been reported to be the cause of poor prognosis.9,10 Therefore, such treatments may increase the risk of technical complications and/or an incident caused by mechanical factors instead of improving oral hygiene.
As such, a valid approach would be to select treatments that preserve tooth substances at the maximum extent possible instead of actively selecting root resection as the first-choice treatment. Johansson et.al.,11 reported that two-thirds of the molar with furcation involvement were preserved 13-16 years after active periodontal treatments were performed. Additionally, Salvi et.al.,12 reported that during the average maintenance period of 11 years, the risk of losing a tooth with degree I furcation involvement was odds ratio of approximately 1.2 compared with a tooth without furcation involvement, showing positive prognosis.
According to the systematic review of Graziani et.al., clinically significant improvement was shown as a result of performing access flap procedures on degree II furcation involvement.13 Tomasi and Wennström et.al.,14 reported that complete or partial closure were achieved in 25-38% of the areas in degree I and degree II furcation involvement after ultrasonic scalers were used alone or with locally appolication of antimicrobials in non-surgical periodontal therapy. Information is however limited on non-surgical periodontal treatment results for different categories of furcation involvement. This study was conducted to retrospectively evaluate the effect of non-surgical periodontal treatment on various degree of furcation involvement.
II. Subjects and methods
Approval was obtained by the Academy Of Clinical Dentistry Ethics Committee prior to conducting this study. In this study, data was analyzed on patients presenting with generalized or localized, stage 3 or 4, grade B or C periodontitis affected by degree I-III furcation involvement on the first molar or the second molar between April 2011 and March 2021 at 7 different clinics. Patient information and clinical results were extracted from medical records of patients who completed the reevaluation after receiving at least basic treatment (non-surgical periodontal treatment). The inclusion criteria and the exclusion criteria are as follows.
Inclusion criteria
・Ages 30-70 at the time of initial examination
・Have 20 or more teeth remaining
・The results of the periodontal examination and intraoral radiographs prior to basic treatment can be confirmed
・The results of periodontal examination at the time of reevaluation after basic treatment can be confirmed.
・Furcation involvement with PPD4mm or more can be observed on molar surface.
Patients and teeth with any of the following criteria were excluded.
Exclusion criteria
・Patients with systemic diseases that will affect treatment outcomes
・Smokers
・Restoration and/or orthodontic devices that affect treatment outcomes are placed in the furcation area
・Existing periapical lesions did not resolve until the time of reevaluation
・The data of periodontal examinaion and intraoral radiography before basic treatment cannot be confirmed
・The data of periodontal examination after basic treatment cannot be confirmed
・Pathological changes that are likely to be affected by wisdom teeth
・Teeth that were extracted by the time of reevaluation
In addition to the results of periodontal examinations, the smoking or non-smoking status, systemic findings were recorded. The following clinical parameters were recorded at the time of initial presentation(baseline:BL) and reevaluation, 2 months or more after, completion of non-surgical treatment of the furcation-involved areas (brushing instructions, subgingival debridement with curettes or ultrasonic scalers).
・Presence of plaque
・Degree of pathological changes in the furcation area (Lindhe & Nyman classification)
・PPD(mm) of tooth surface in the furcation area
・Bleeding on probing at the furcation area (BOP)
・Mobility
・Intraoral radiographs at the time of initial diagnosis
Additionally, if there were smooth surfaces of adjacent or contralateral single-rooted teeth or molars of the same patient with similar levels of PPD and BOP, these parameters were recorded as those of the control group.
Data analysis
In this study, improvement of the furcation-involved area in degree was selected as the primary endpoint followed by the analysis on improvement in PPD, BOP, plaque formation of tooth surface at the furcation-involved area as the secondary endpoint.
Furcation areas were classified as degree I, II and III at the time of BL and additionally, the degree at the time of reevaluation and/or frequency of complete or partial closure furcation were calculated.
Mean value, frequency and standard deviation on PPD, BOP, plaque for overall furcation-involved areas and control groups were calculated followed by calculation of mean value and standard deviation corresponding to each category and each control group. Calculations were similarly performed for PPD of 4-5mm and 6mm or more at BL separately. Sites with PPD4-5mm at BL had only two degree III furcation involvement cases, and thus was subjected to combined analysis with degree II cases. For PPD, the differences from BL to reevaluation for each group were analyzed by paired t-test, and comparisons of data between groups at BL, reevaluation, and change between BL to reevaluation were analyzed by student’s t-test. Student’s t-test was used to analyze data of each group at the time of BL and reevaluation, and changes from the time of BL as compared to the time of reevaluation. For multiple comparison, one-way analysis of variance and SNK tests were used.
Comparison was made on BOP and plaque with Chi-squared tests at the time of BL versus reevaluation.
III. Results
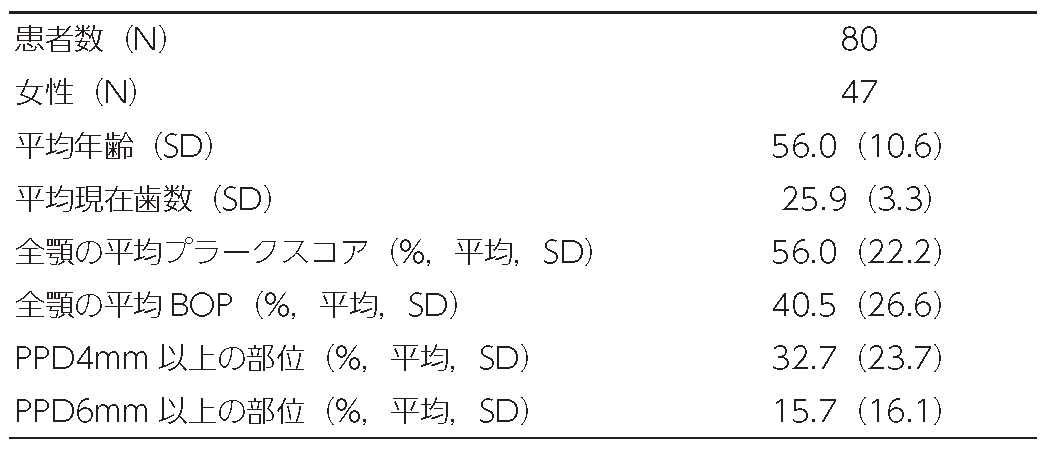
Characteristics of the subjects at BL
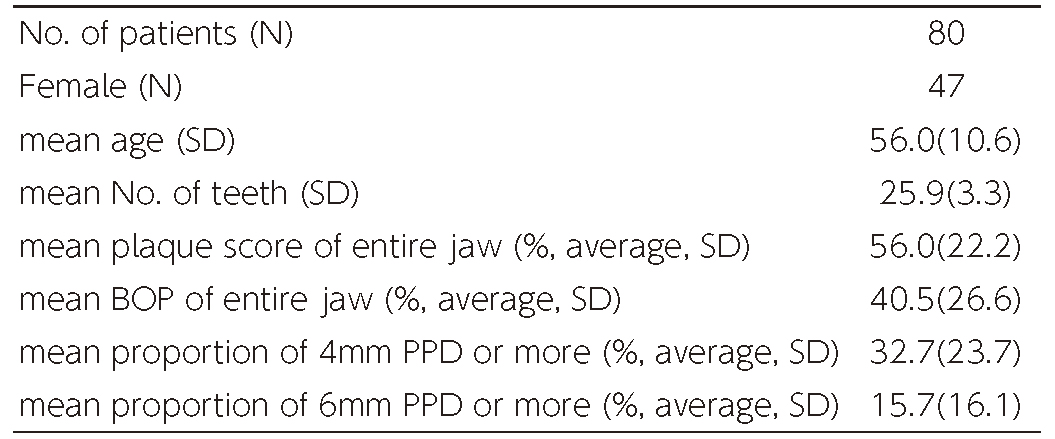
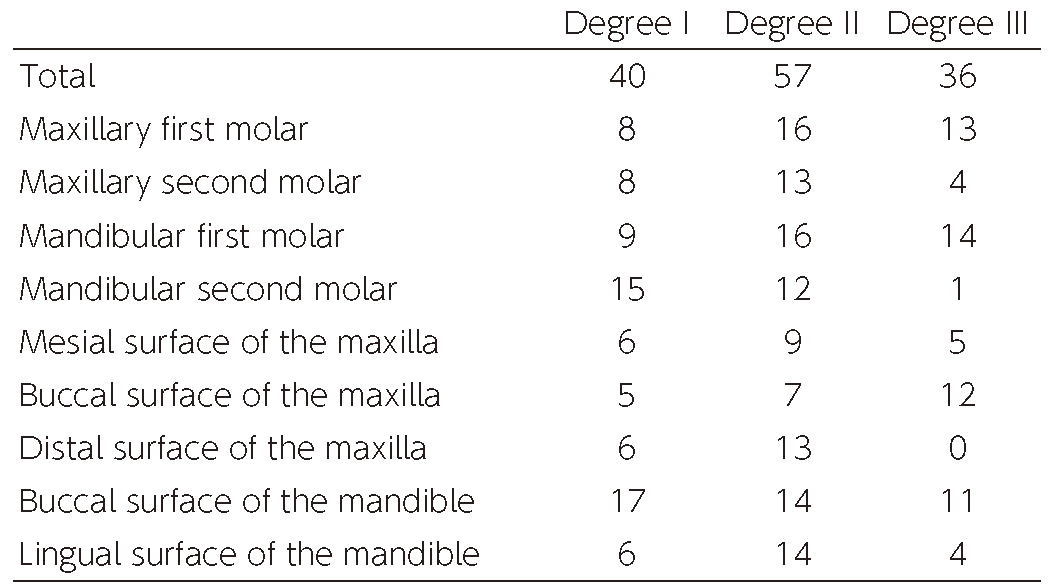
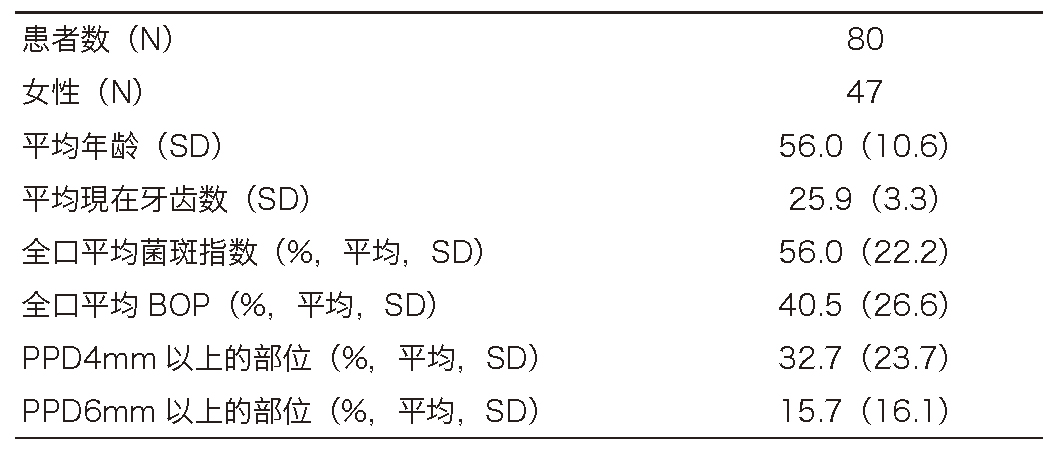
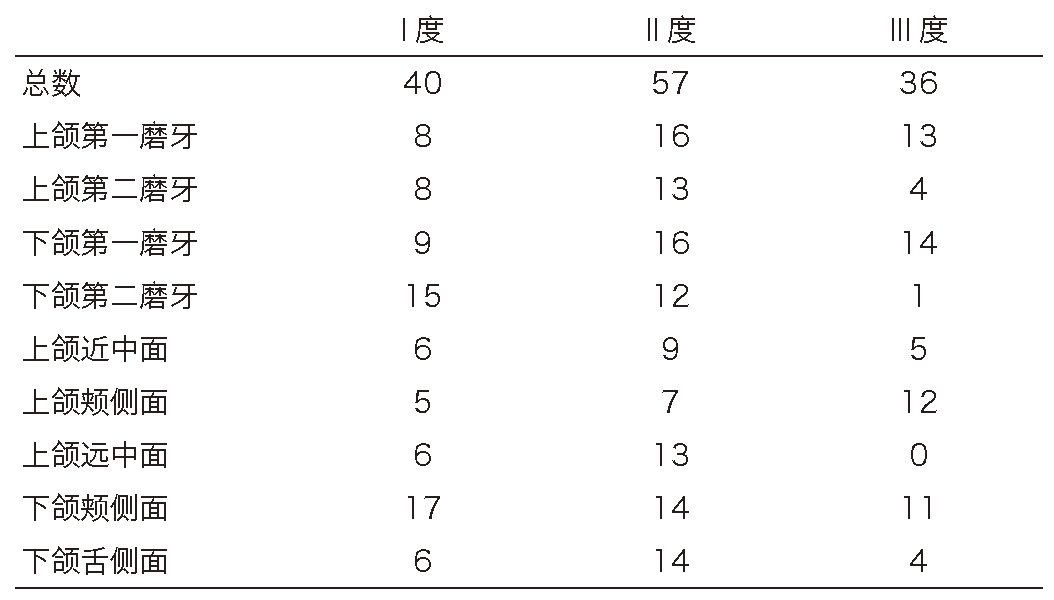
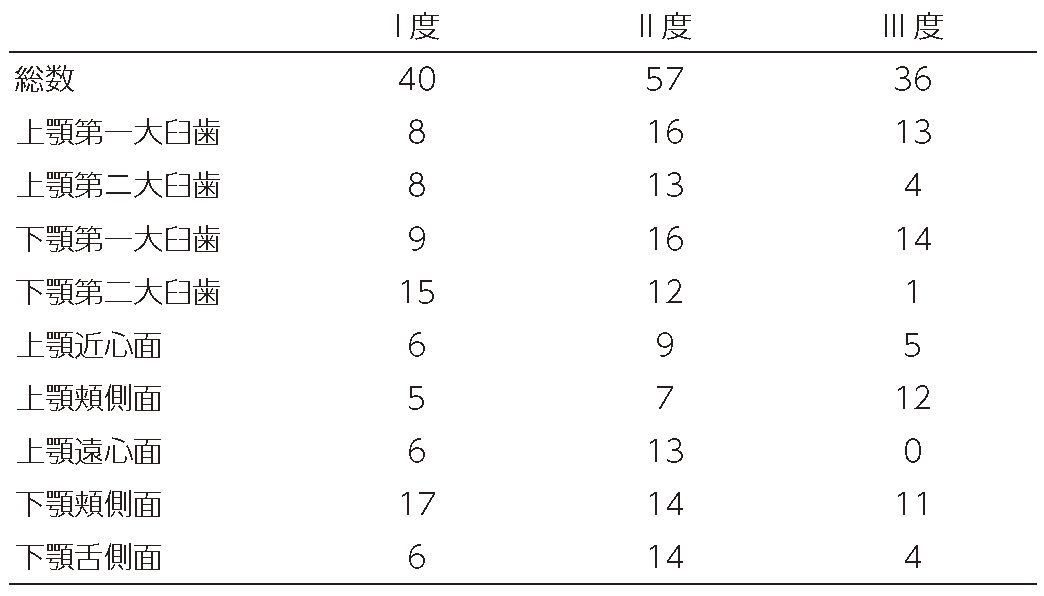
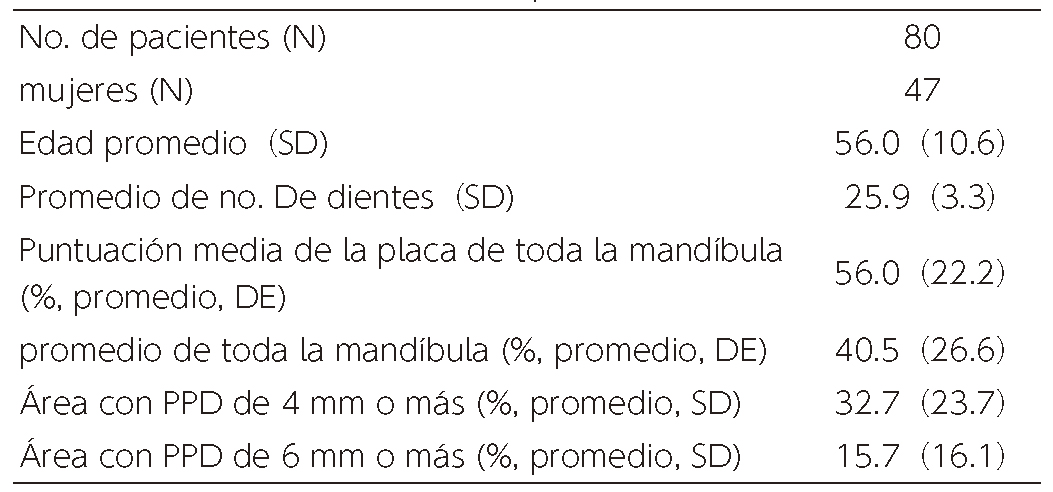
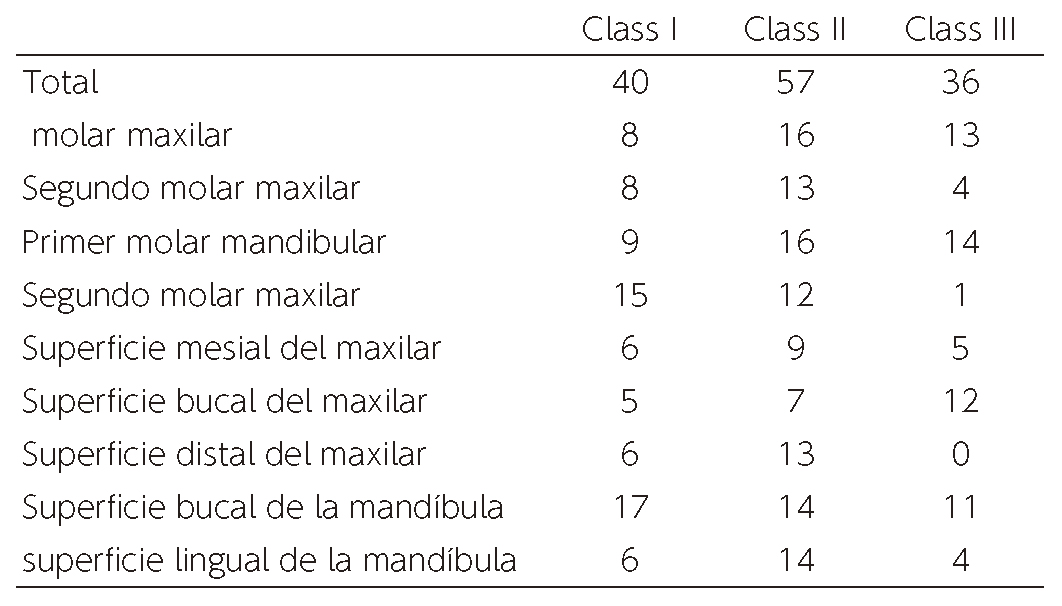
The characteristics of patients at BL are shown on Table 1. Data of 80 periodontal patients (47 females), with average age of 56.0(SD 10.6) were collected. Table 2 shows the distribution of furcation-involved teeth for each categories that were included in the study. The total number of teeth was 133, out of which 40 teeth were degree I, 57 teeth were degree II and 36 teeth were degree III. The smooth surface of 80 teeth with no furcation involvement were placed in the control group.
(Table 1) Characteristics of patients at the time of BL(Table 2) Distribution of affected teeth at the time of BL
Treatment outcomes
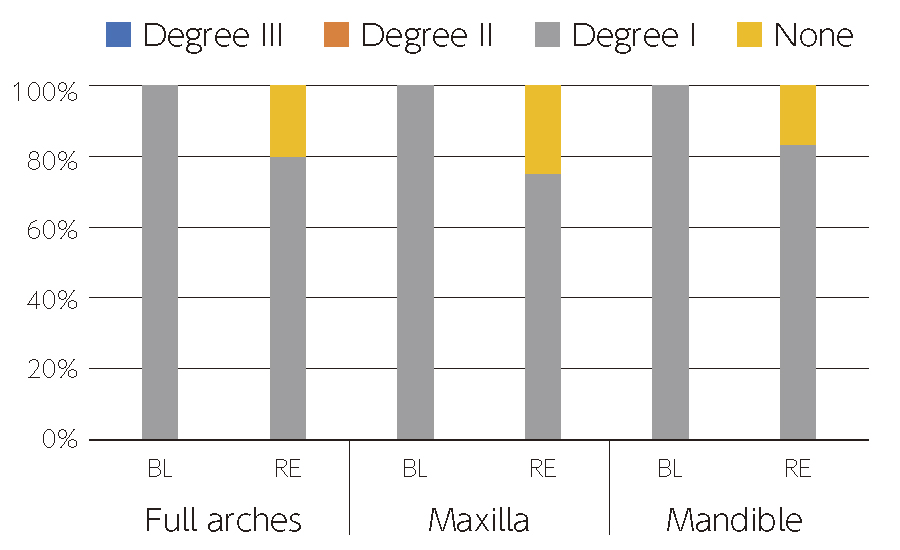
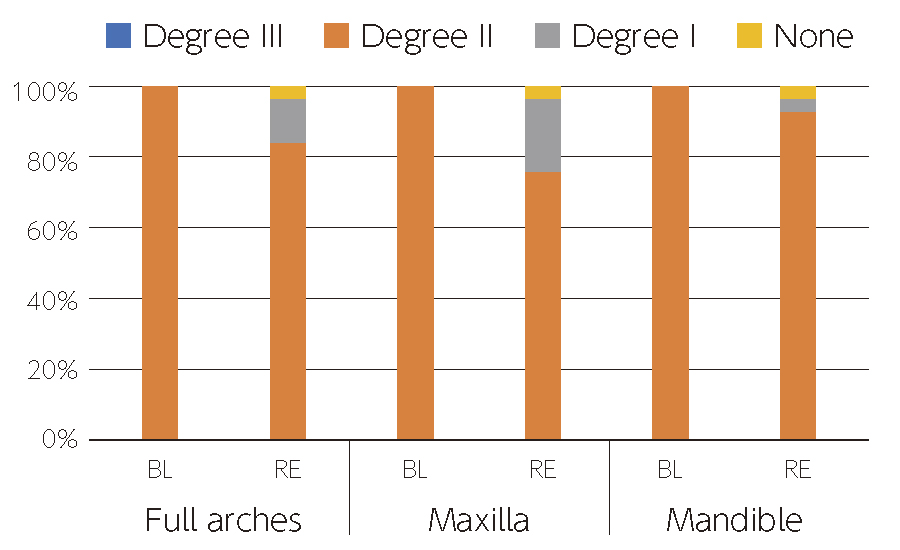
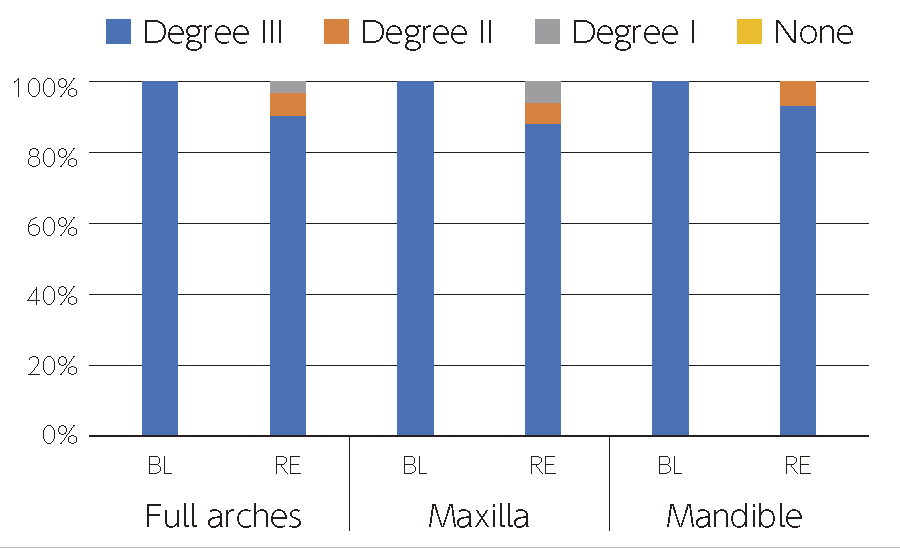
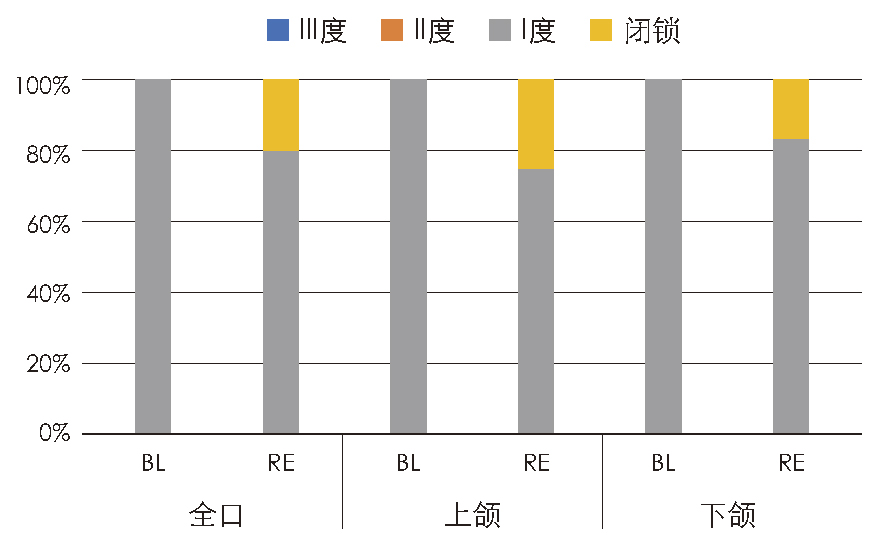
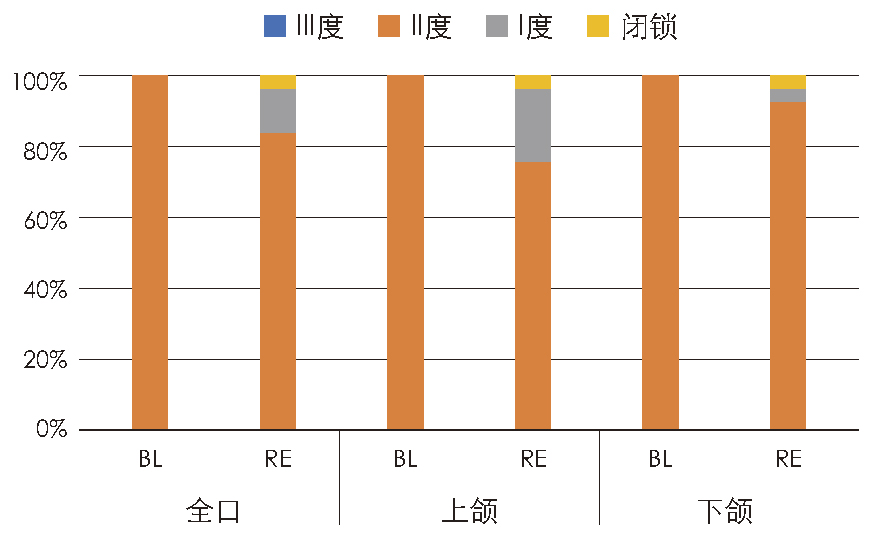
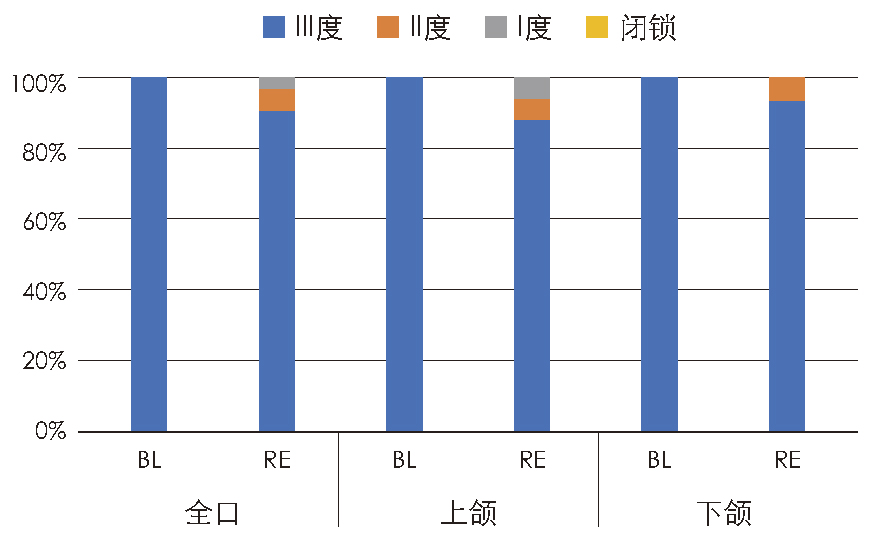
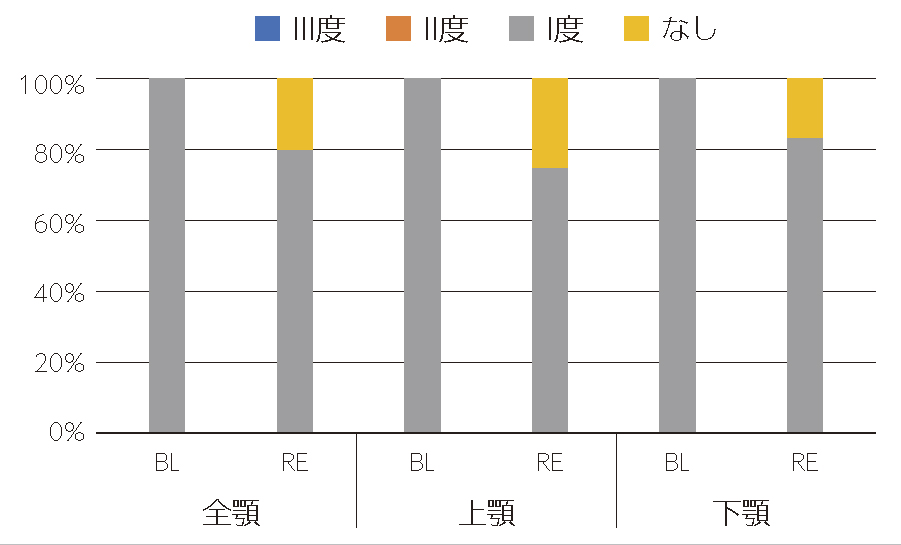
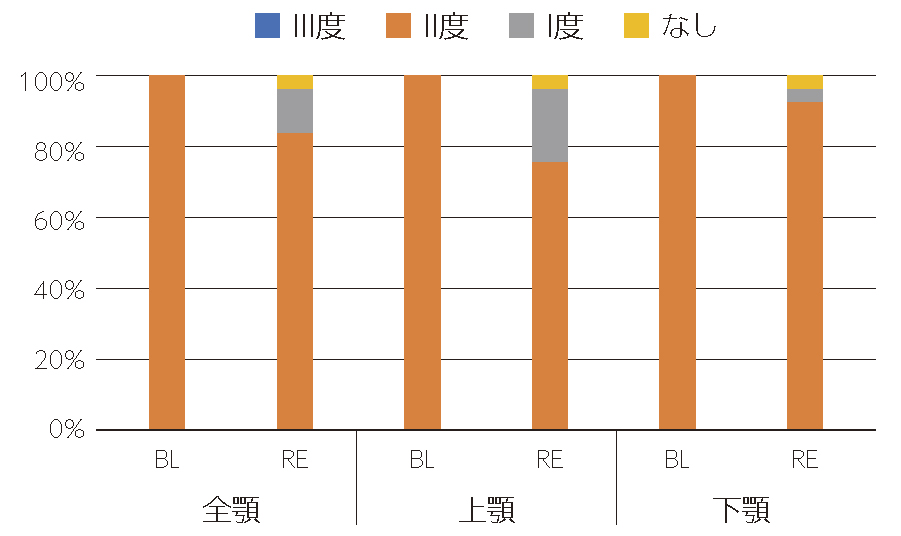
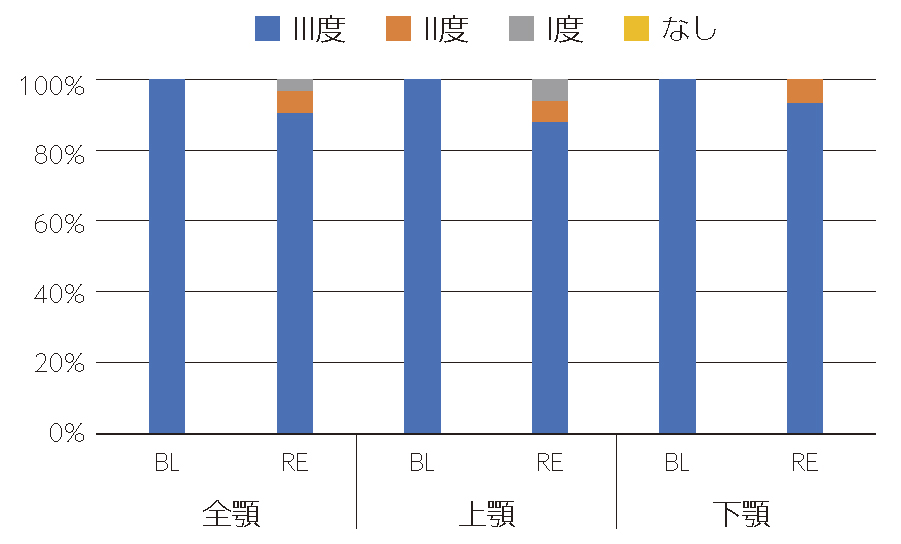
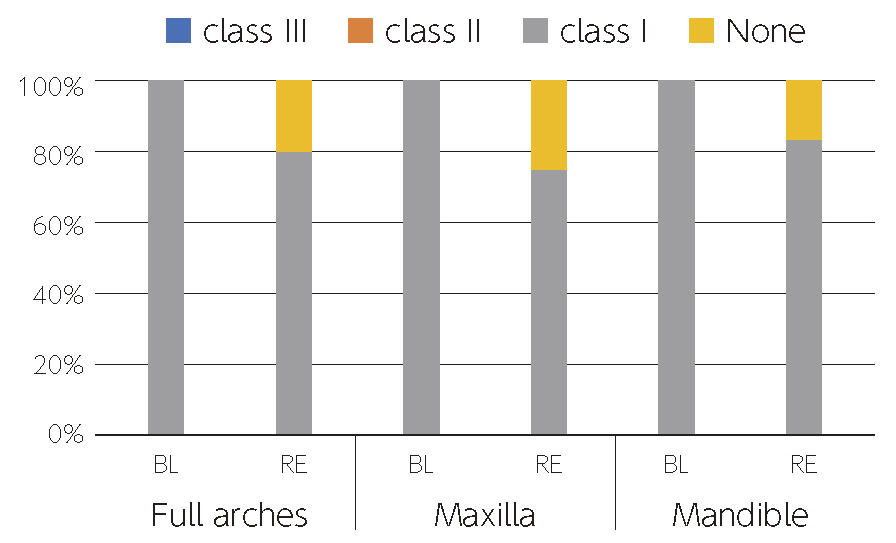
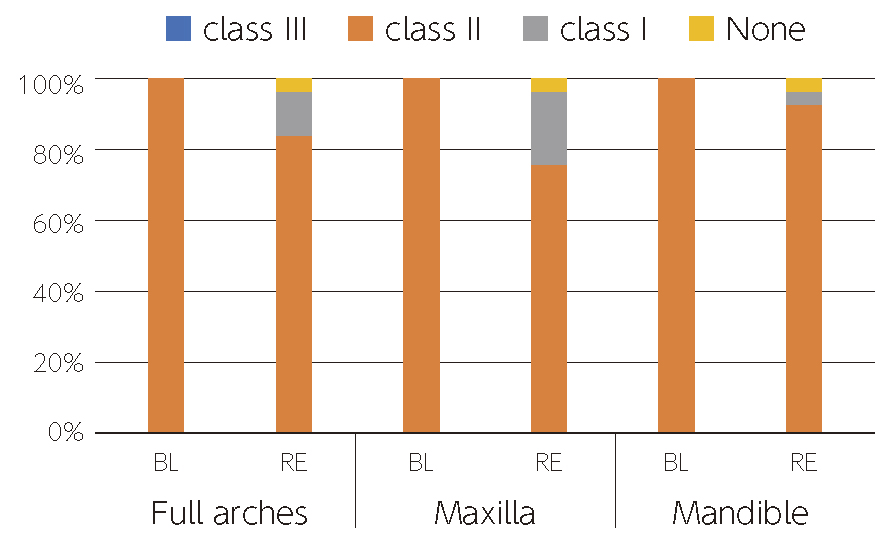
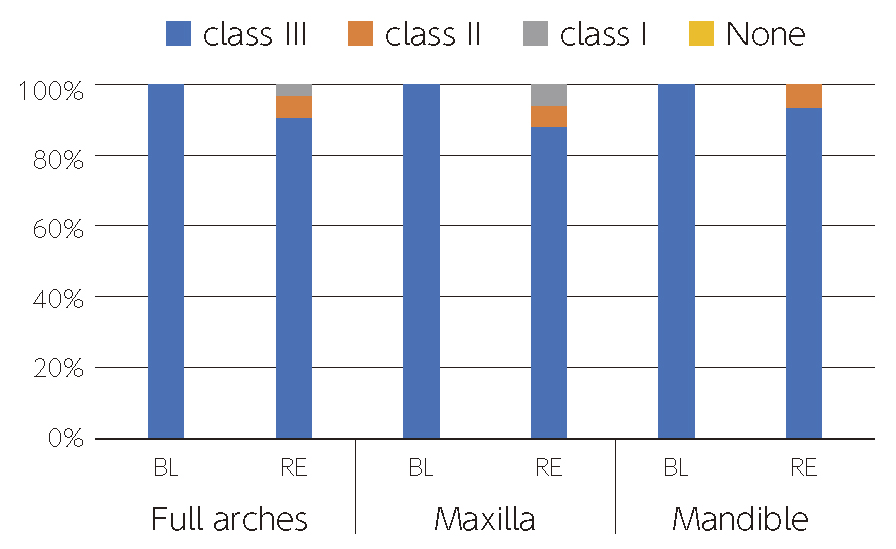
Fig.1 shows the treatment results of degree I furcation involvement. The overall closure rate was 20% with 25% on the maxillary region and 16.7% on the mandibular region. Similarly in degree II cases, the overall closure rate was 3.5% and 12.3% improved to degree I. Closure rate or the improvement rate to degree I was 24.1% in the maxillary region and 7.2% in the mandibular region (Fig.2). No complete closure was found in degree III cases while the overall improvement rate to degree II was 6.3% and degree I was 3.1%. No improvement to degree I was found in the mandibular area (Fig.3).
(Fig. 1) % distribution after treatment of degree I furcation involvement(Fig. 2) % distribution of each degree of furcation involvement after treatment of degree II(Fig. 3) % distribution of each degree of furcation involvement after treatment of degree III
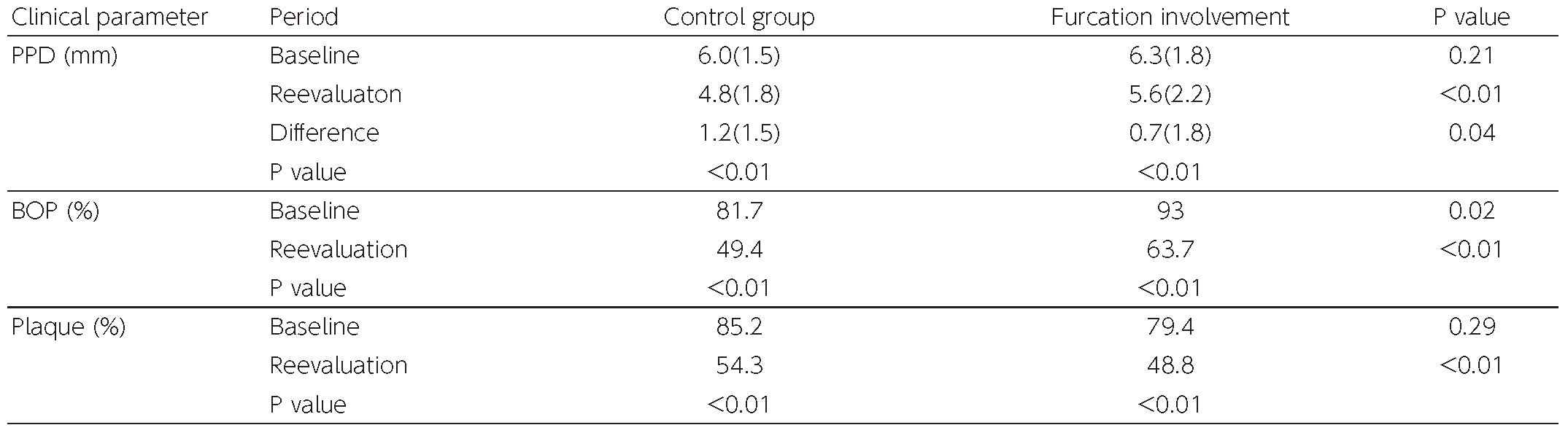
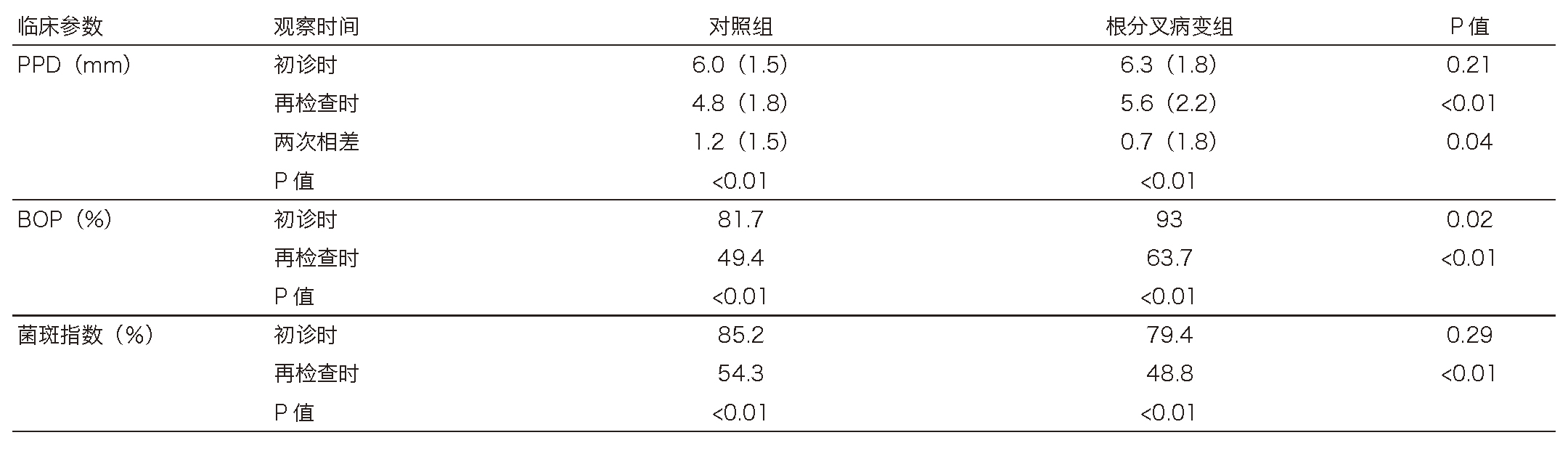
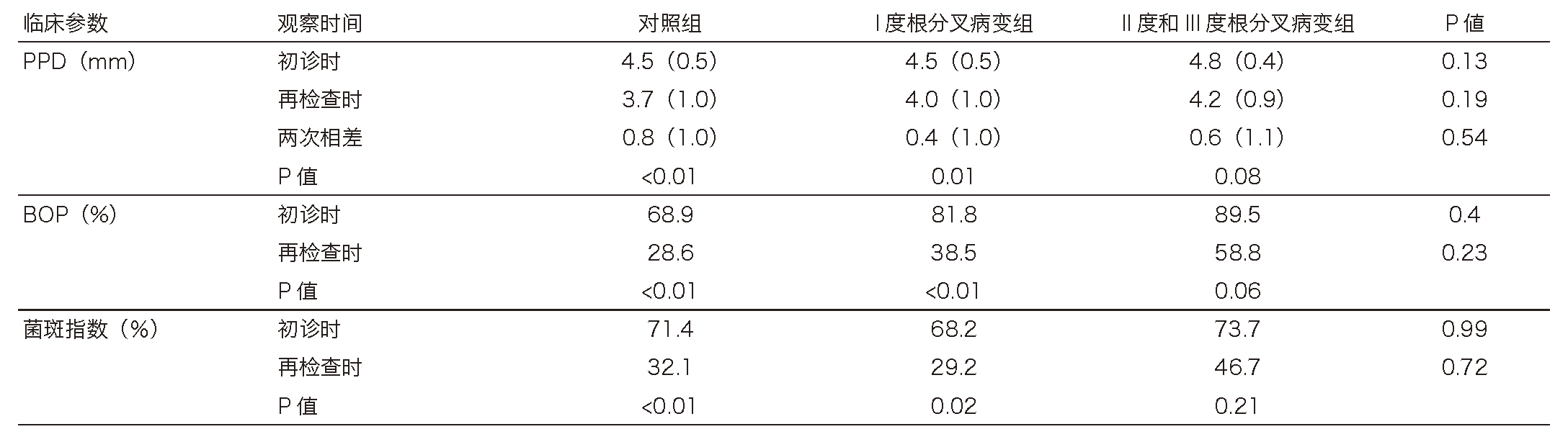
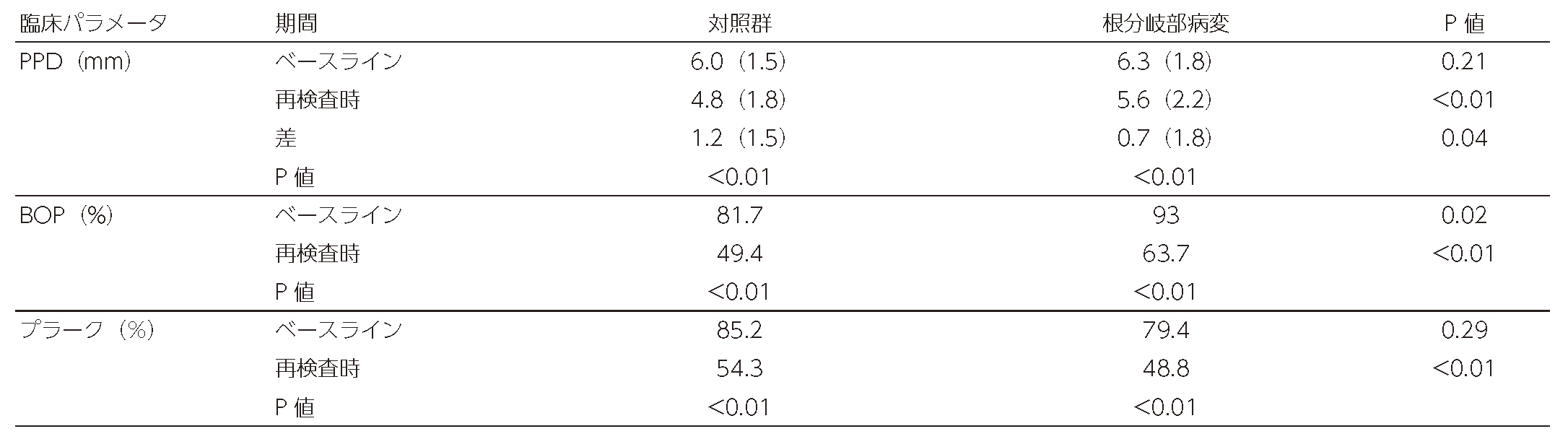
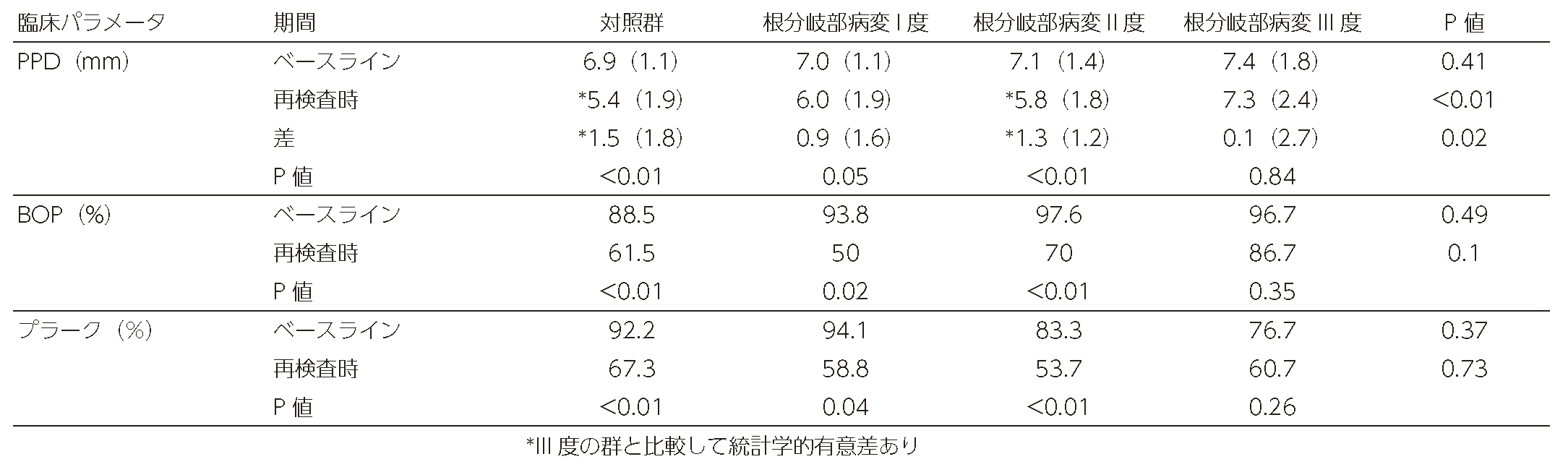
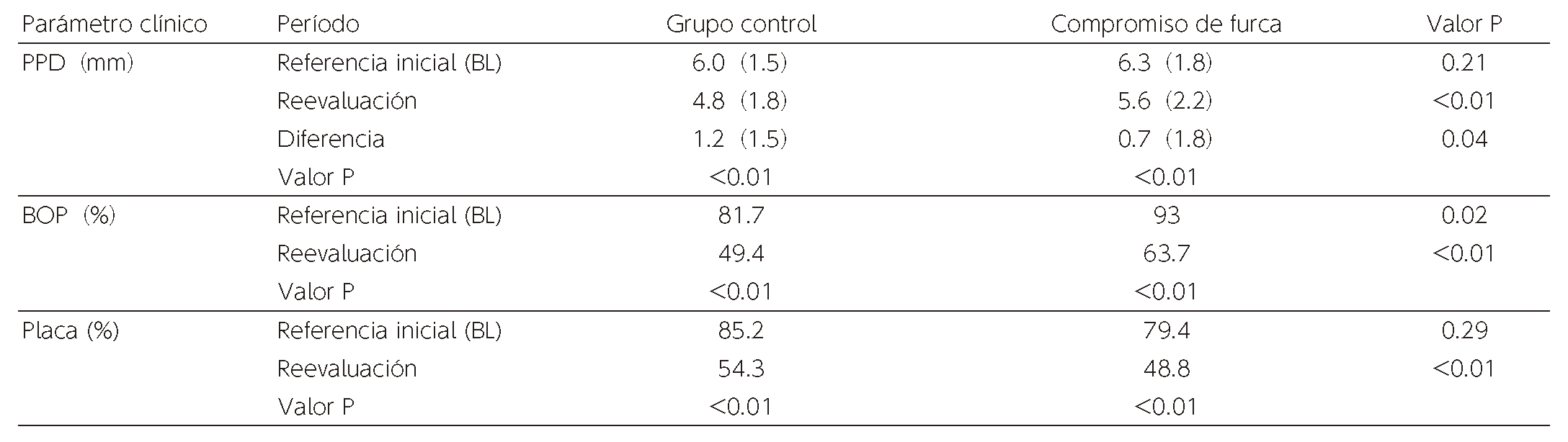
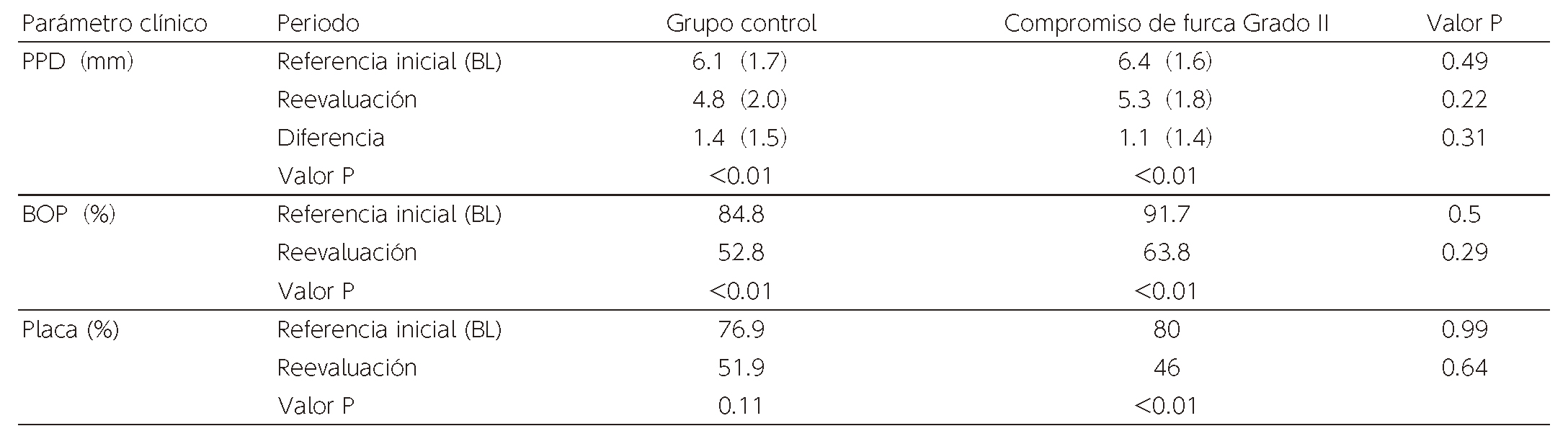
Table 3 illustrates the changes in the clinical parameter of the furcation sites and the those of the control group. BOP frequency at the time of BL was lower in the control group, showing statistically significant difference while no statistically significant difference was found between the groups in values of other parameters at BL. BOP and plaque frequency declined significantly in both groups. The mean PPD of the control group was reduced by 1.2mm, which was higher than the that of furcation involvement group of 0.7mm, making the difference statistically significant.
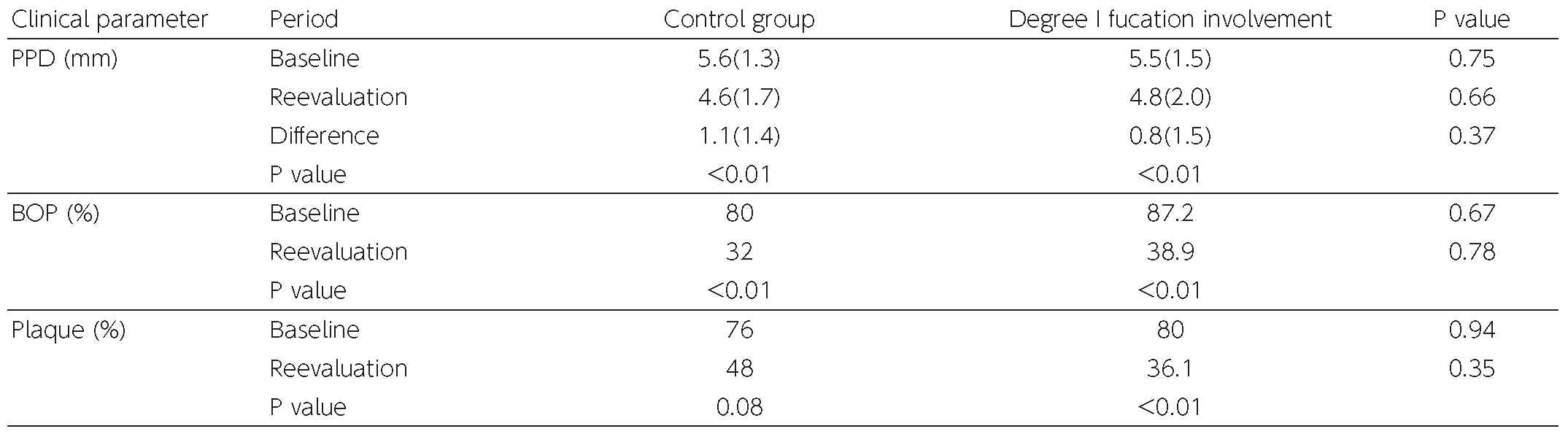
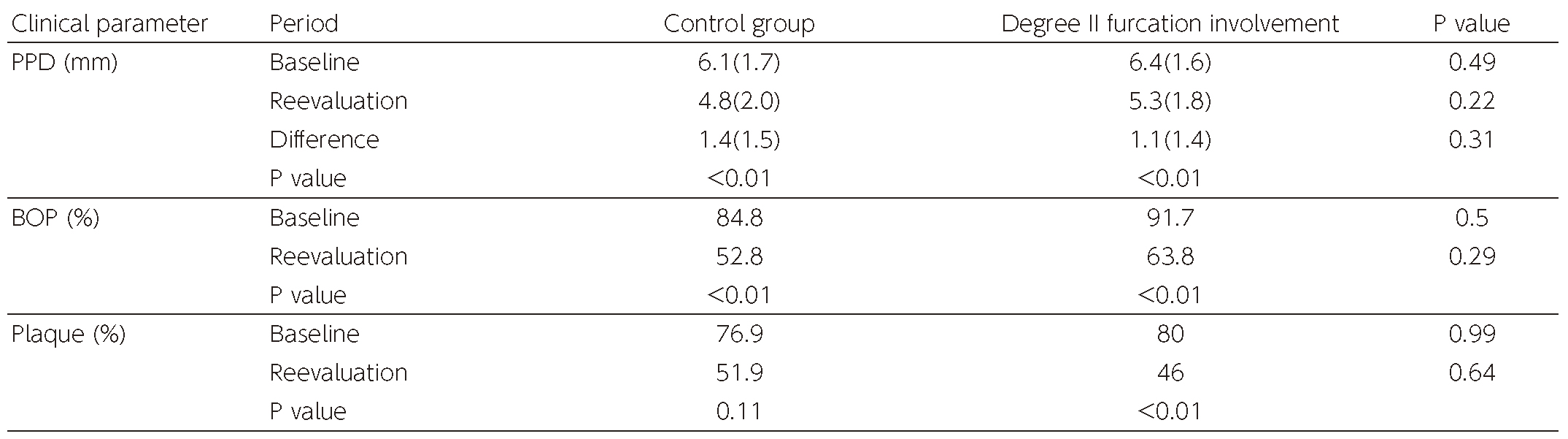
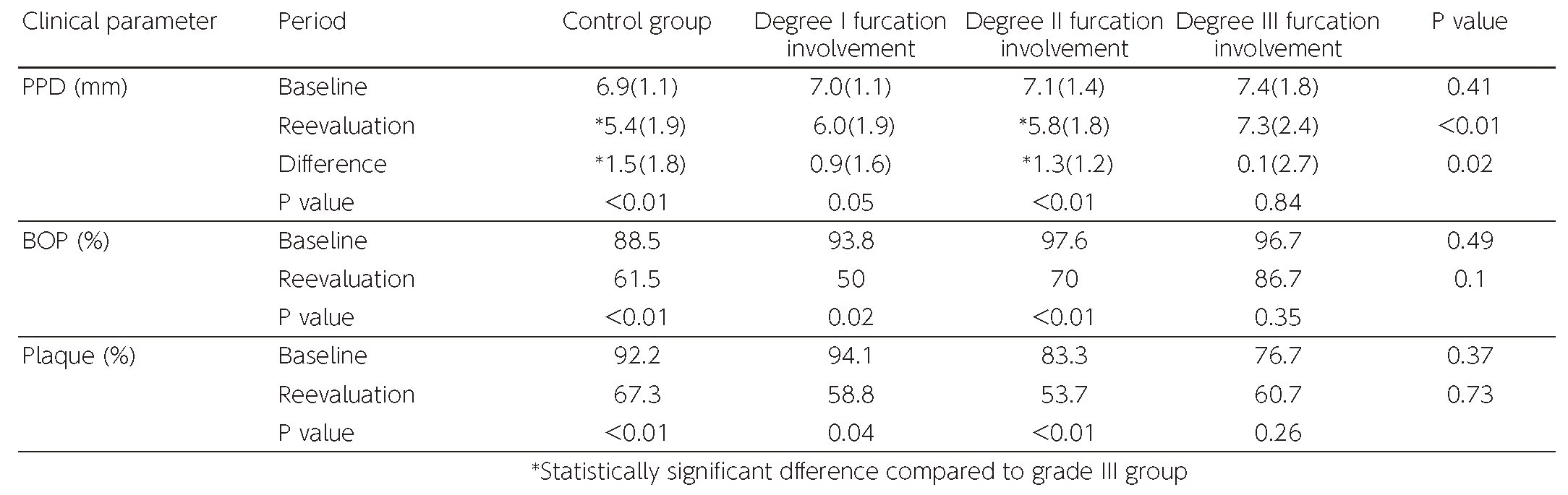
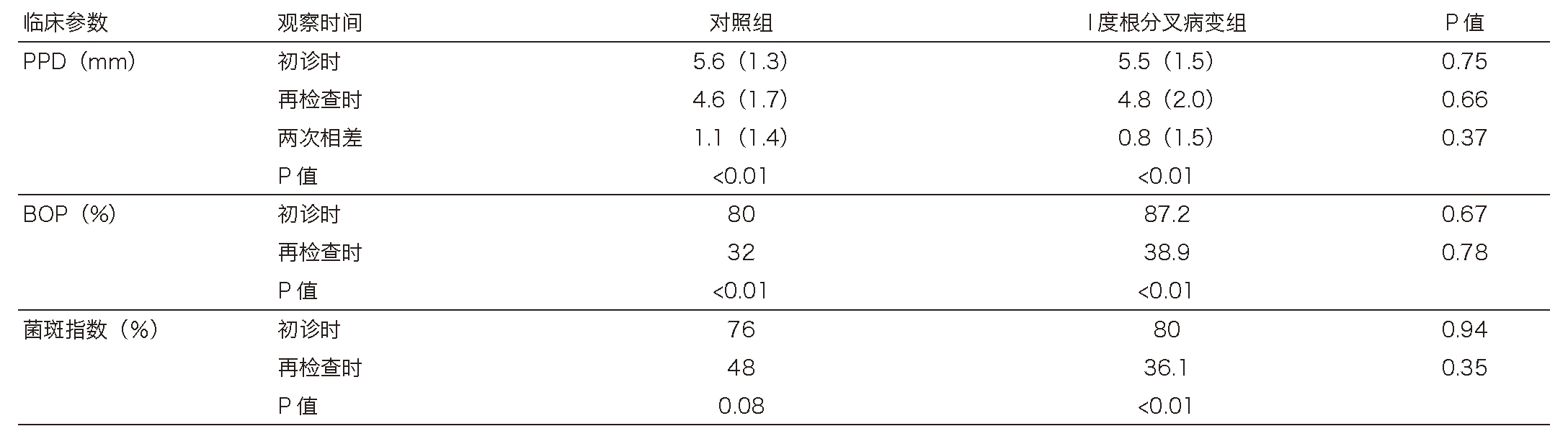
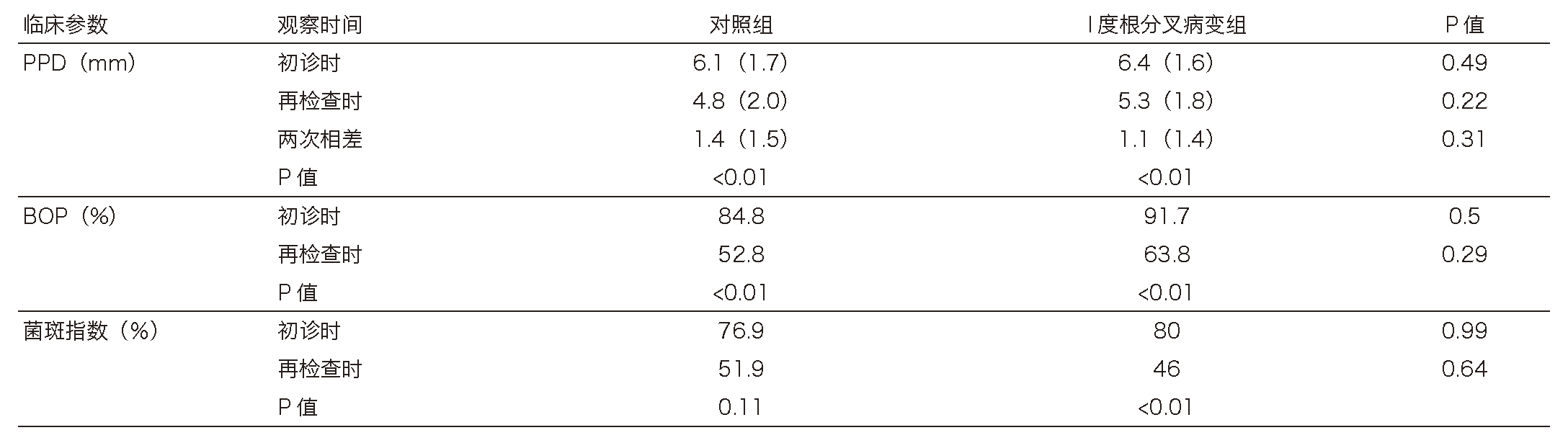
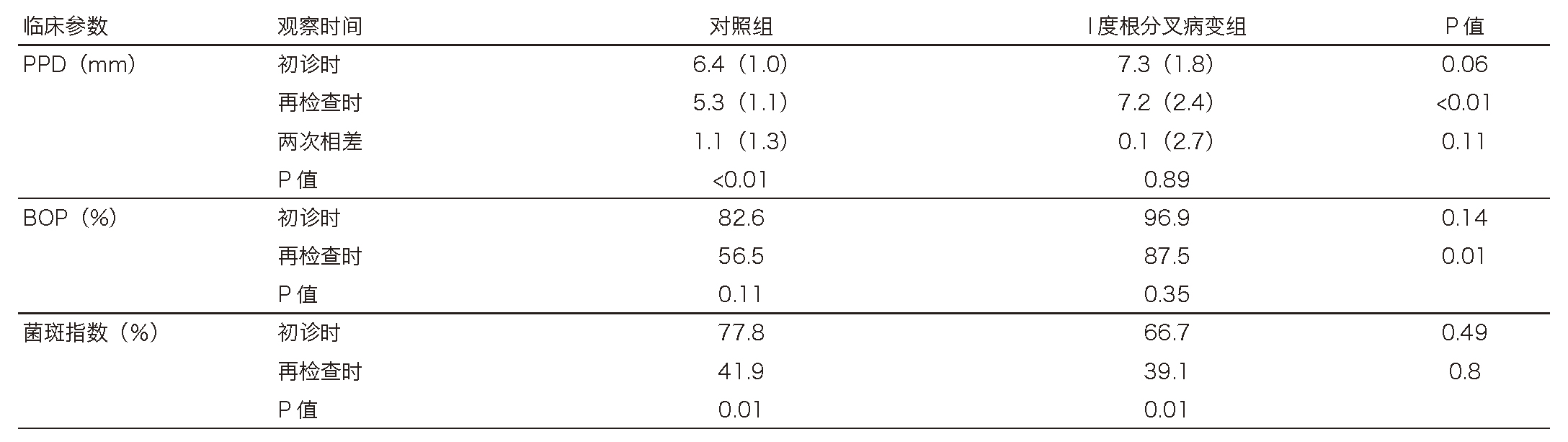
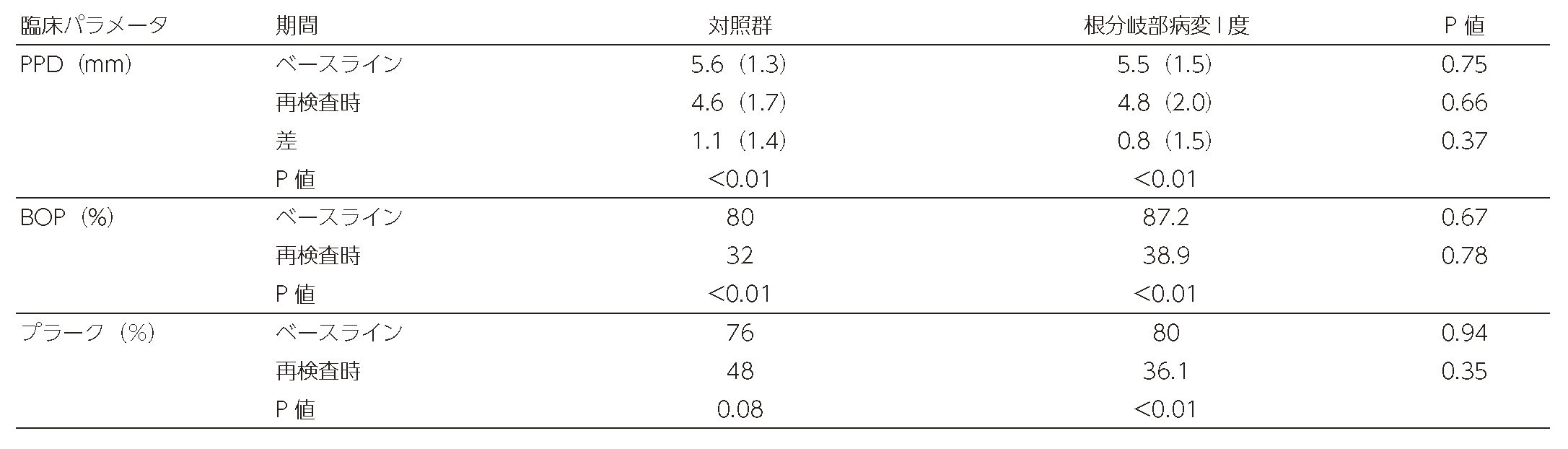
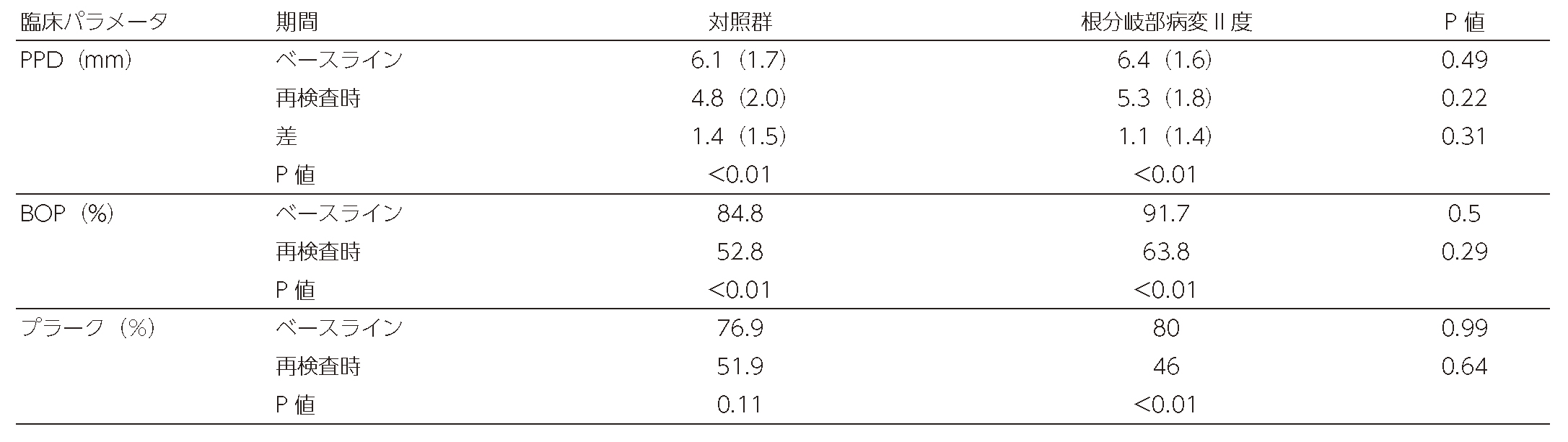
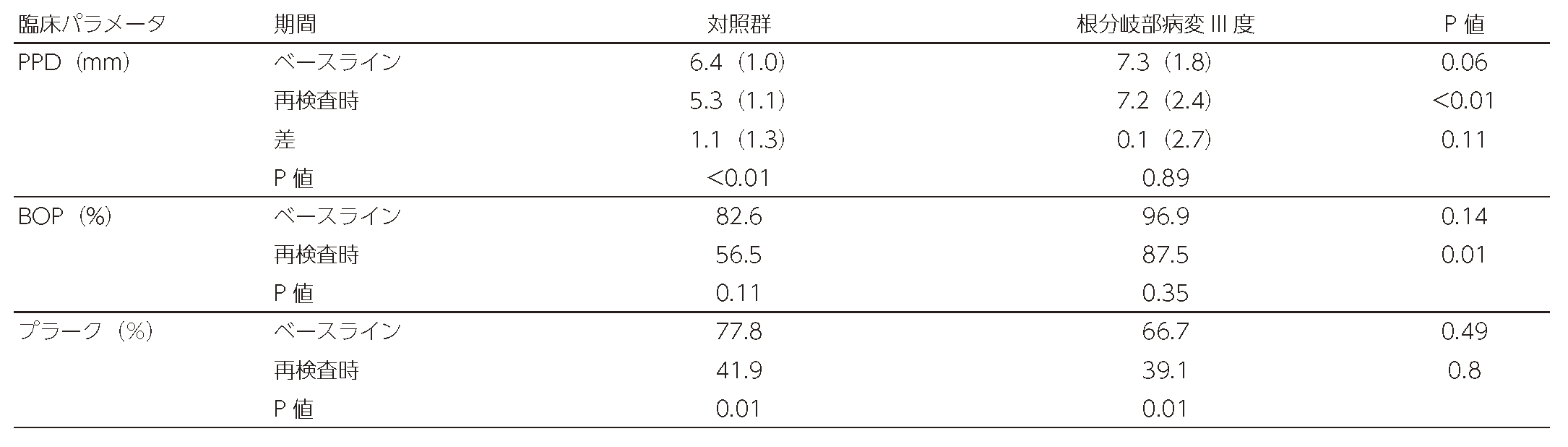
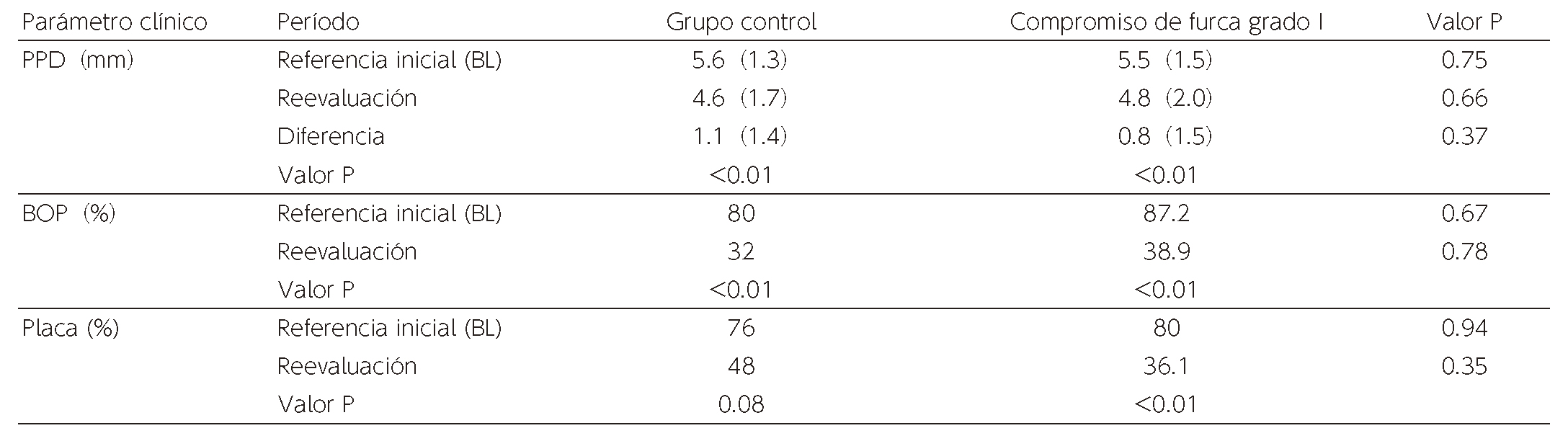
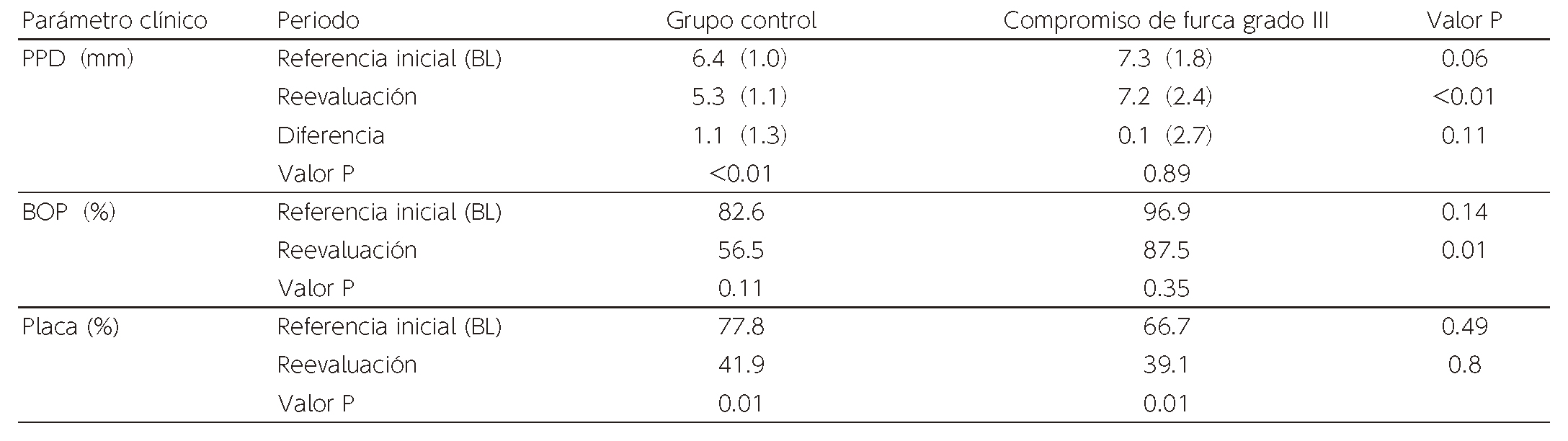
When analyzed separately for each degree of furcation involvement, there wase no statistically significant difference in each clinical parameter in all groups at BL. Statistically significant reduction was observed in plaque in degree I-III groups. Significant improvement was shown in BOP frequency for degree I and II groups before and after treatment while no significant improvement was made in degree III group. Similar trends were observed in control groups (Tables 4-6). On average PPD, significant improvement was made in degree I and II while no statistically significant difference was found as compared to the control group. In degree III cases, the changes between BL and reevaluation were 0.1mm on average, showing no statistically significant difference. Improvement in the control group was 1.1mm on average, exhibiting statistically significant difference.
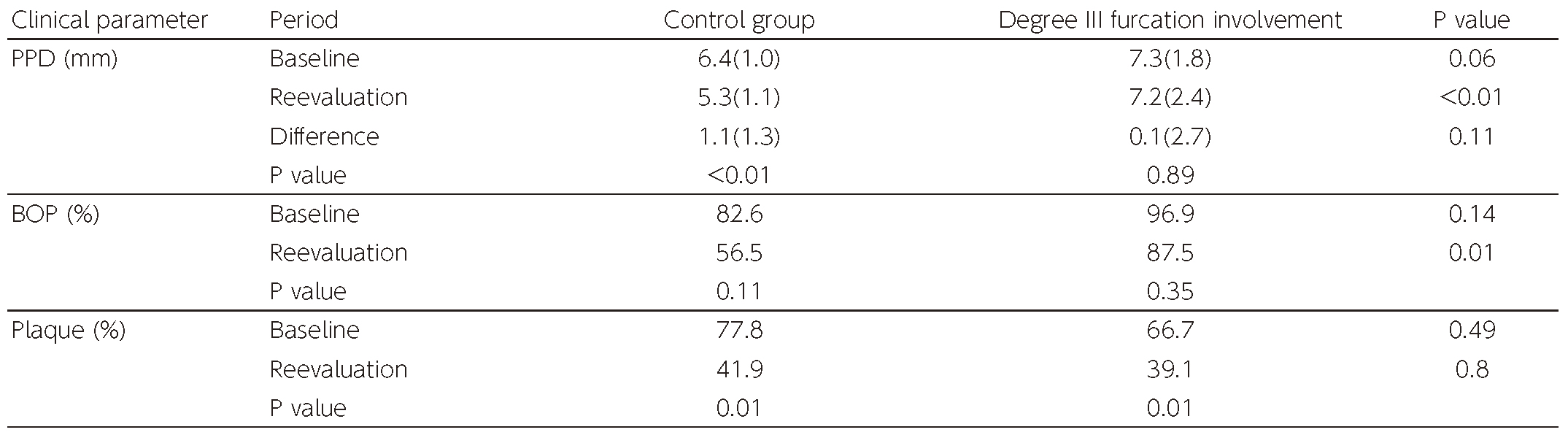
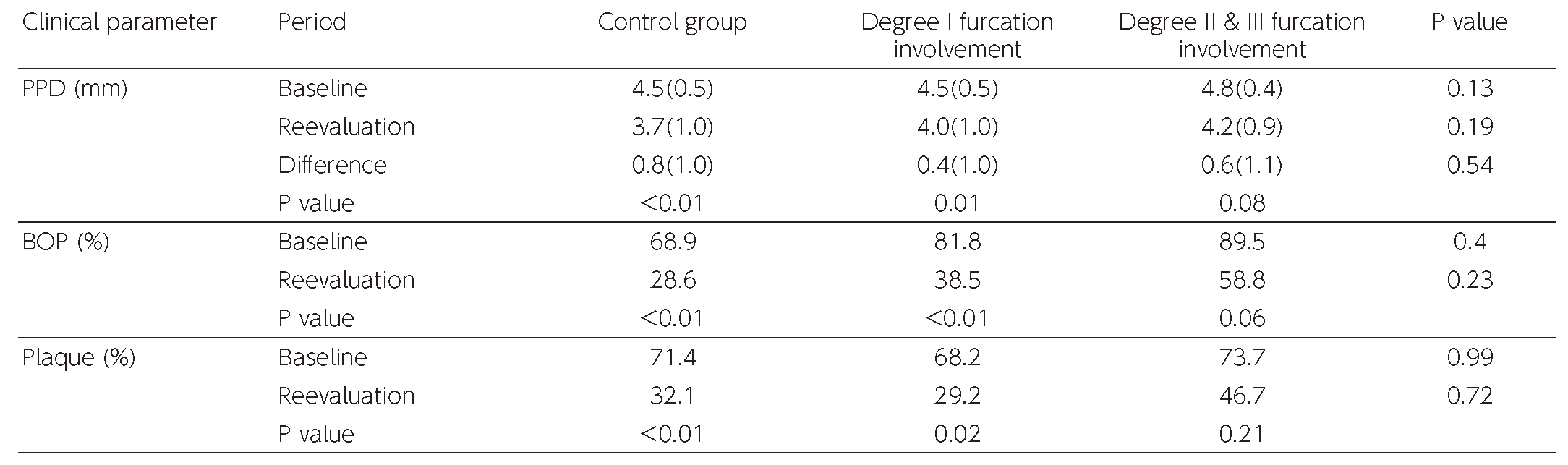
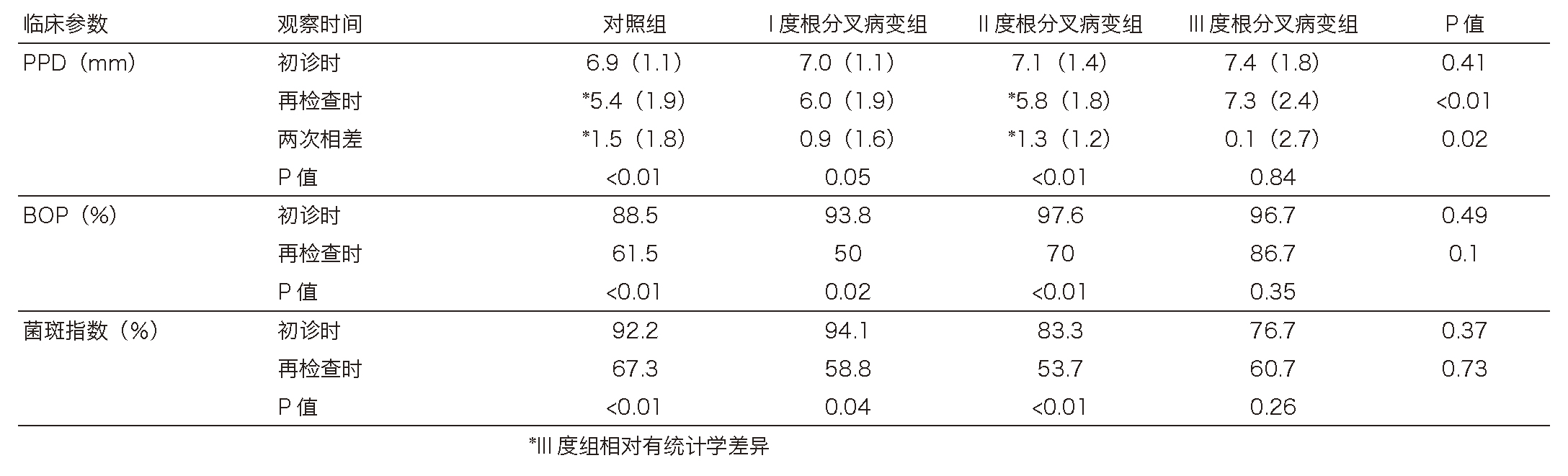
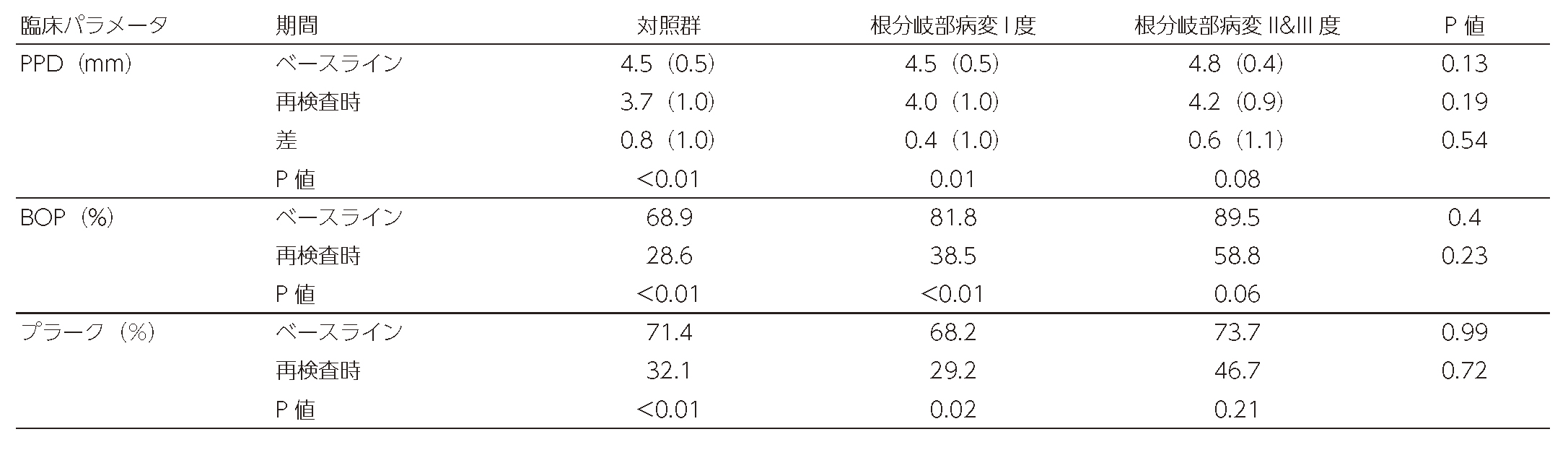
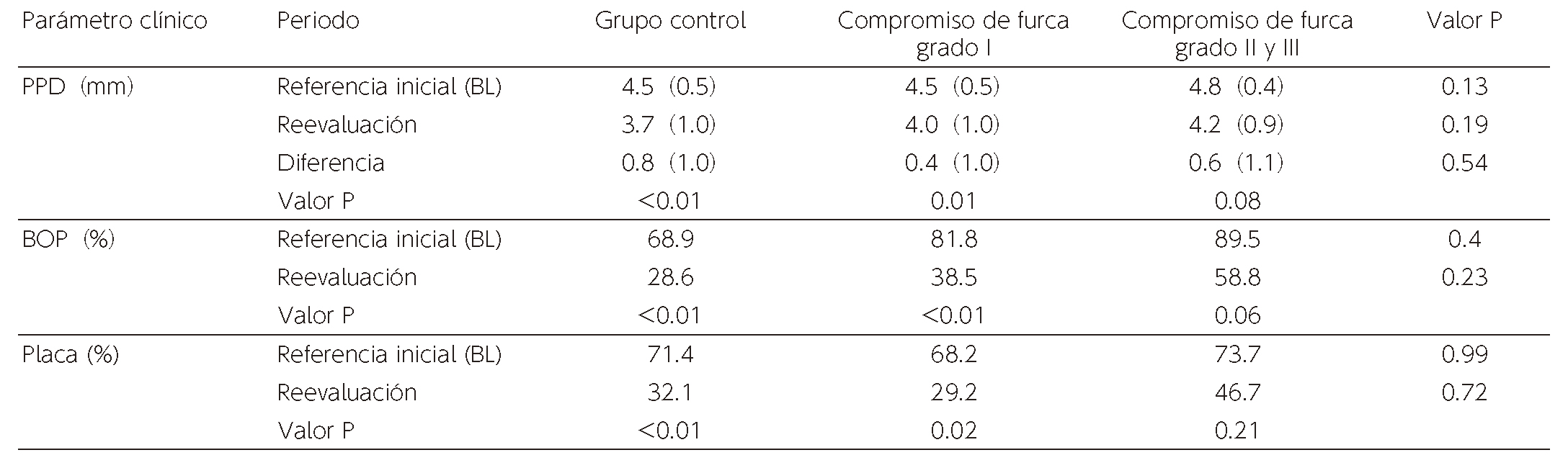
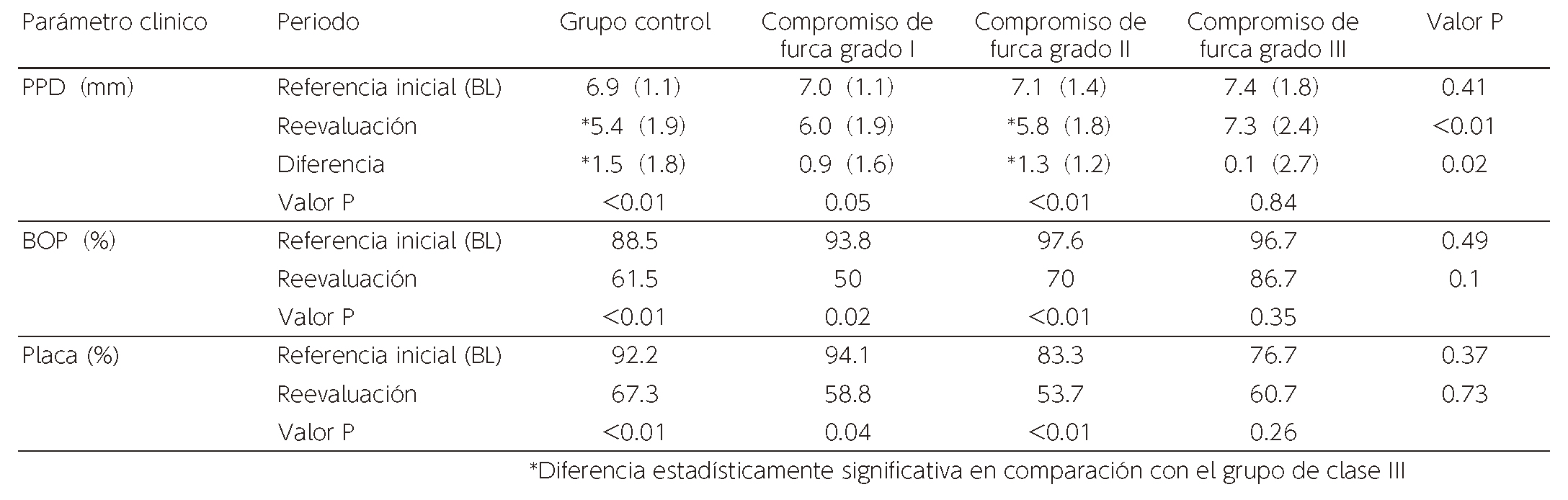
Table 7 illustrates the changes in clinical parameter of each group when PPD was 4-5mm at BL. No significant difference in clinical parameters were observed among the groups at BL. Significant reductions on frequency of plaque were seen in the control group and degree I group while no significant changes were observed in degree II / III group. No significant difference in the improvement of PPD was found among the 3 groups. Table 8 shows the a results of group of PPD with 6mm or more at BL. No significant difference was shown in clinical parameters among groups at BL. On Plaque and BOP frequency, significant improvement was observed in control groups, degree I and degree II groups while no significant change was seen in degree III group. The control group and degree II group had higher improvement than degree III group on mean PPD, exhibiting a statistically significant difference.
(Table 3) Parameters of furcation-involved tooth surfaces and control group tooth surfaces at BL and reevaluation(Table 4) Parameters of degree I furcation-involved tooth surfaces and control group tooth surfaces at BL and reevaluation(Table 5) Parameters of degree II furcation-involved tooth surfaces and control group tooth surfaces at BL and reevaluation(Table 6) Parameters of degree III furcation-involved tooth surfaces and control group tooth surfaces at BL and reevaluation(Table 7) Parameters of teeth surfaces with 4-5mm PPD at BL, at the time of BL and reevaluation(Table 8) Parameters of tooth surfaces with 6mm PPD or more at BL, at the time of BL and reevaluation
IV. Discussion
In retrospective research results, complete closure by non-surgical treatment was achieved in 20% of the cases in degree I, 3.5% in degree II and 0% in degree III. 15.8% of the degree II cases and 9.4% of the degree III cases improved to degree I or below. Such results indicate that complete closure of furcation-involved areas by non-surgical treatment are difficult to achieve in degree II and III. Additionally, improvement to degree I level occurred only on a limited number of cases. Study conducted by Salvi et.al12 in an average SPT period of 11.5 years indicated that odd ratio for losing a tooth during the SPT period in degree I furcation involvement was 1.17compared with molars without furcation involvement with no statistically significant difference, and therefore degree I furcation involvement do not pose the risk of tooth loss. Such results show that “partial closure” to degree I level may serve as a treatment goal. Tomasi and Wennström14 reported that as a result of implementing non-surgical periodontal treatment on 38% of degree I furcation sites, complete closure was achieved, and in degree II cases, 25% had partial closure or complete closure. While the reason for such higher closure rates compared to those in our study is not clear, differences in plaque control, anatomic form and time restrictions may be factors affecting the results. In our study however, while the closure rate was lower, no cases have deteriorated, and therefore, the thought was that non-surgical therapies were worthwhile implementing at the initial stage of the treatment. Additionally, the above-mentioned study conducted by Tomasi and Wennström14indicates that furcation involvement improve further by repeating non-surgical treatments, and therefore, such approach is likely to be effective.
In this study, data on single-root teeth or smooth surface of molars with remaining PPD equivalent to PPD or furcation-involved sites was used as the control group. Since the results of non-surgical periodontal treatment of single-rooted tooth surfaces and smooth surfaces of molars are shown to be not different, merging these teeth into one control group is likely justified.6,7 The number of tooth surfaces with furcation area did not precisely match the number of sites on flat surfaces showing similar value of clinical parameter in each patient posed a limitation on this study that was designed to be a retrospective study.
On average, 1.2mm improvement was made on PPD of tooth surfaces of the control group by non-surgical treatment. The meta-analysis in the systematic review of Suvan et.al.,15showed that PPD improvement by SRP was 1.38mm on average. Since the difference from the results in our study is minimal, the results of the control group in our study are likely to be close to the generally accepted average. PPD reduction on tooth surfaces with furcation involvement measured 0.7mm on average, showing a statistically significant difference from that of the control group. Nordland et.al., indicated that if PPD before treatment was 4.5mm or more, compared to non-molars and smooth surface of molars, the reduction in PPD by non-surgical treatment in furcation sites would be less.6 Such results are partly explained by a higher plaque formation rate on the furcation area. In this study however, no difference was observed in the plaque formation rate between the furcation involvement group and the control group. In a study conducted by Knöfler et.al., comparing the results of SRP on full mouth and SRP on each quadrant,16 while PPD of furcation-involved teeth surface was 4-6mm before treatment, PPD reduction after non-surgical treatment on furcation-involved surfaces was 0.9-1.0mm, and on smooth surfaces 1.0-1.3mm. BOP at sites with furcation improved by approximately 30%, yielding similar results to those in our study. Therefore, to evaluate treatment results of furcation involvement, PPD value before treatment should be considered.
In this study, furcation involvement at the time of initial examination was analyzed by degree. The treatment results of only degree III furcation involvement were less effective compared to those of the control group, which likely affected the entire results for furcation involvement cases. The degree of furcation involvement in the study of Nordland et.al.,6 is unknown with a high likelihood that the degree of those before treatment differed from that of the subjects in our study. In the study conducted by Tomasi and Wennström,14 the one-stage non-surgical periodontal treatment on degree I and II furcation involvement resulted in PPD reduction averaging 1.1-1.3mm, which was similar to the treatment results of Nordland et.,al.6 In our study, PPD reduction averaged 0.8mm in degree I and 1.1mm in degree II. The slightly lower improvement compared to those of treatment results in the study above may be partly explained as follows: in the data of Tomasi and Wennström14 for example, PPD before treatment in degree I was an average of 5.8mm and in degree II, 7.1mm whereas in our study, degree I averaged 5.5mm and degree II 6.4mm.
In our study, when PPD was 6mm or more at the sites of degree III furcation, no significant improvement was shown compared to other groups. One reason is likely to be that improvement in plaque control in such areas was at 15%, which was limited compared to other groups. Dannewitz et.al.,17 reported that as a result of treating 4 teeth out of 67 degree III furcation-involved teeth with SRP only, 3 teeth were lost in a 5 year period while 9 out of 62 teeth were lost after surgical treatment including root resection, regenerative therapy, or flap surgery. In degree III furcation sites with deep PPD, non-surgical periodontal treatment had a limited effect, and therefore, other treatment modalities, including teeth extraction, should be considered in treatment plans.
This study is a retrospective study conducted by multiple facilities and therefore, the process including reproducibility of examinations, standardized treatment protocols, and various time constraints, may not have been sufficiently standardized. For example, while PPD did not improve in degree III furcation involvement cases, improvement to lower degree was observed, which may be due to regression to the mean. The furcation involvement itself may have been undervalued due to detection biases. There is a need to confirm our study results in prospective studies at a larger scale in the near future.
V. Conclusion
Non-surgical periodontal treatments have limited effectiveness in closing furcation areas while improved clinical parameters in other areas were obtained except for degree III cases. Therefore, non-surgical treatments would be a valid approach as an initial treatment. Additional research is needed at a larger scale to confirm such research results in the near future.
Reference
Badersten A, Nilvéus R, Egelberg J. Effect of nonsurgical periodontal therapy. I. Moderately advanced periodontitis. J Clin Periodontol. 1981 Feb;8(1):57-72. doi: 10.1111/j.1600-051x.1981.tb02024.x.
Badersten A, Nilveus R, Egelberg. Effect of nonsurgical periodontal therapy. II. Severely advanced periodontitis. J Clin Periodontol. 1984 Jan;11(1):63-76. doi: 10.1111/j.1600-051x.1984.tb01309.x.
Tomasi C, Leyland AH, Wennström JL. Factors influencing the outcome of non-surgical periodontal treatment: a multilevel approach. J Clin Periodontol. 2007 Aug;34(8):682-90. doi: 10.1111/j.1600-051X.2007.01111.x
Svärdström G, Wennström JL. Furcation topography of the maxillary and mandibular first molars. J Clin Periodontol. 1988 May;15(5):271-5. doi: 10.1111/j.1600-051x.1988.tb01583.x.PMID: 3164728
Matia JI, Bissada NF, Maybury JE, Ricchetti P. Efficiency of scaling of the molar furcation area with and without surgical access. Int J Periodontics Restorative Dent. 1986;6(6):24-35.
Nordland P, Garrett S, Kiger R, Vanooteghem R, Hutchens LH, Egelberg The effect of plaque control and root debridement in molar teeth. J Clin Periodontol. 1987 Apr;14(4):231-6. doi: 10.1111/j.1600-051x.1987.tb00972.x.PMID: 3294917
Loos B, Nylund K, Claffey N, Egelberg Clinical effects of root debridement in molar and non-molar teeth. A 2-year follow-up. J Clin Periodontol. 1989 Sep;16(8):498-504. doi: 10.1111/j.1600-051x.1989.tb02326.x.PMID: 2778083
Dommisch H, Walter C, Dannewitz B, Eickholz P. Resective surgery for the treatment of furcation involvement: A systematic review. J Clin Periodontol. 2020 Jul;47 Suppl 22:375-391. doi: 10.1111/jcpe.13241.
Langer B, Stein SD, Wagenberg B. An evaluation of root resections. A ten-year study. J Periodontol. 1981 Dec;52(12):719-22. doi: 10.1902/jop.1981.52.12.719.
Bühler H. Evaluation of root-resected teeth. Results after 10 years. J Periodontol. 1988 Dec;59(12):805-10. doi: 10.1902/jop.1988.59.12.805.
Johansson KJ, Johansson CS, Ravald N. The prevalence and alterations of furcation involvements 13 to 16 years after periodontal treatment. Swed Dent J. 2013;37(2):87-95.
Salvi GE, Mischler DC, Schmidlin K, Matuliene G, Pjetursson BE, Brägger U, Lang NP. Risk factors associated with the longevity of multi-rooted teeth. Long-term outcomes after active and supportive periodontal therapy. J Clin Periodontol. 2014 Jul;41(7):701-7. doi: 10.1111/jcpe.12266. Epub 2014 May 26.
Graziani F, Gennai S, Karapetsa D, Rosini S, Filice N, Gabriele M, Tonetti M. Clinical performance of access flap in the treatment of class II furcation defects. A systematic review and meta-analysis of randomized clinical trials. J Clin Periodontol. 2015 Feb;42(2):169-81. doi: 10.1111/jcpe.12327.
Tomasi C, Wennström JL.J Periodontol. Locally delivered doxycycline as an adjunct to mechanical debridement at retreatment of periodontal pockets: outcome at furcation sites. J Periodontol. 2011 Feb;82(2):210-8. doi: 10.1902/jop.2010.100308.
Suvan J, Leira Y, Moreno Sancho FM, Graziani F, Derks J, Tomasi C. Subgingival instrumentation for treatment of periodontitis. A systematic review. J Clin Periodontol. 2020 Jul;47 Suppl 22:155-175. doi: 10.1111/jcpe.13245.
Knöfler GU, Purschwitz RE, Jentsch HF. Clinical evaluation of partial- and full-mouth scaling in the treatment of chronic periodontitis. J Periodontol. 2007 Nov;78(11):2135-42. doi: 10.1902/jop.2007.070010.
Dannewitz B, Zeidler A, Hüsing J, Saure D, Pfefferle T, Eickholz P, Pretzl B. Loss of molars in periodontally treated patients: results 10 years and more after active periodontal therapy. J Clin Periodontol. 2016 Jan;43(1):53-62. doi: 10.1111/jcpe.1
1) The Nippon Dental University, School of Life Dentistry, Department of Periodontology
2) Wada Dental Clinic
3) Meikai University School of Dentistry, Division of Dental Biomaterials Science,Department of Restorative and Biomaterials Sciences
4) Heartful Dental Clinic
5) Aoba Dental Clinic
6) Matsumoto dental university department of Dental science and materials
7) Mieji Dental Clinic
8) Iryo Hojin Shikyoukai, Yabuki Dental Clinic
9) Fukuda Dental Clinic
Badersten A, Nilvéus R, Egelberg J. Effect of nonsurgical periodontal therapy. I. Moderately advanced periodontitis. J Clin Periodontol. 1981 Feb;8(1):57-72. doi: 10.1111/j.1600-051x.1981.tb02024.x.
Badersten A, Nilveus R, Egelberg. Effect of nonsurgical periodontal therapy. II. Severely advanced periodontitis. J Clin Periodontol. 1984 Jan;11(1):63-76. doi: 10.1111/j.1600-051x.1984.tb01309.x.
Tomasi C, Leyland AH, Wennström JL. Factors influencing the outcome of non-surgical periodontal treatment: a multilevel approach. J Clin Periodontol. 2007 Aug;34(8):682-90. doi: 10.1111/j.1600-051X.2007.01111.x
Svärdström G, Wennström JL. Furcation topography of the maxillary and mandibular first molars. J Clin Periodontol. 1988 May;15(5):271-5. doi: 10.1111/j.1600-051x.1988.tb01583.x.PMID: 3164728
Matia JI, Bissada NF, Maybury JE, Ricchetti P. Efficiency of scaling of the molar furcation area with and without surgical access. Int J Periodontics Restorative Dent. 1986;6(6):24-35.
Nordland P, Garrett S, Kiger R, Vanooteghem R, Hutchens LH, Egelberg The effect of plaque control and root debridement in molar teeth. J Clin Periodontol. 1987 Apr;14(4):231-6. doi: 10.1111/j.1600-051x.1987.tb00972.x.PMID: 3294917
Loos B, Nylund K, Claffey N, Egelberg Clinical effects of root debridement in molar and non-molar teeth. A 2-year follow-up. J Clin Periodontol. 1989 Sep;16(8):498-504. doi: 10.1111/j.1600-051x.1989.tb02326.x.PMID: 2778083
Dommisch H, Walter C, Dannewitz B, Eickholz P. Resective surgery for the treatment of furcation involvement: A systematic review. J Clin Periodontol. 2020 Jul;47 Suppl 22:375-391. doi: 10.1111/jcpe.13241.
Langer B, Stein SD, Wagenberg B. An evaluation of root resections. A ten-year study. J Periodontol. 1981 Dec;52(12):719-22. doi: 10.1902/jop.1981.52.12.719.
Bühler H. Evaluation of root-resected teeth. Results after 10 years. J Periodontol. 1988 Dec;59(12):805-10. doi: 10.1902/jop.1988.59.12.805.
Johansson KJ, Johansson CS, Ravald N. The prevalence and alterations of furcation involvements 13 to 16 years after periodontal treatment. Swed Dent J. 2013;37(2):87-95.
Salvi GE, Mischler DC, Schmidlin K, Matuliene G, Pjetursson BE, Brägger U, Lang NP. Risk factors associated with the longevity of multi-rooted teeth. Long-term outcomes after active and supportive periodontal therapy. J Clin Periodontol. 2014 Jul;41(7):701-7. doi: 10.1111/jcpe.12266. Epub 2014 May 26.
Graziani F, Gennai S, Karapetsa D, Rosini S, Filice N, Gabriele M, Tonetti M. Clinical performance of access flap in the treatment of class II furcation defects. A systematic review and meta-analysis of randomized clinical trials. J Clin Periodontol. 2015 Feb;42(2):169-81. doi: 10.1111/jcpe.12327.
Tomasi C, Wennström JL.J Periodontol. Locally delivered doxycycline as an adjunct to mechanical debridement at retreatment of periodontal pockets: outcome at furcation sites. J Periodontol. 2011 Feb;82(2):210-8. doi: 10.1902/jop.2010.100308.
Suvan J, Leira Y, Moreno Sancho FM, Graziani F, Derks J, Tomasi C. Subgingival instrumentation for treatment of periodontitis. A systematic review. J Clin Periodontol. 2020 Jul;47 Suppl 22:155-175. doi: 10.1111/jcpe.13245.
Knöfler GU, Purschwitz RE, Jentsch HF. Clinical evaluation of partial- and full-mouth scaling in the treatment of chronic periodontitis. J Periodontol. 2007 Nov;78(11):2135-42. doi: 10.1902/jop.2007.070010.
Dannewitz B, Zeidler A, Hüsing J, Saure D, Pfefferle T, Eickholz P, Pretzl B. Loss of molars in periodontally treated patients: results 10 years and more after active periodontal therapy. J Clin Periodontol. 2016 Jan;43(1):53-62. doi: 10.1111/jcpe.1
1) The Nippon Dental University, School of Life Dentistry, Department of Periodontology
2) Wada Dental Clinic
3) Meikai University School of Dentistry, Division of Dental Biomaterials Science,Department of Restorative and Biomaterials Sciences
4) Heartful Dental Clinic
5) Aoba Dental Clinic
6) Matsumoto dental university department of Dental science and materials
7) Mieji Dental Clinic
8) Iryo Hojin Shikyoukai, Yabuki Dental Clinic
9) Fukuda Dental Clinic
Badersten A, Nilvéus R, Egelberg J. Effect of nonsurgical periodontal therapy. I. Moderately advanced periodontitis. J Clin Periodontol. 1981 Feb;8(1):57-72. doi: 10.1111/j.1600-051x.1981.tb02024.x.
Badersten A, Nilveus R, Egelberg. Effect of nonsurgical periodontal therapy. II. Severely advanced periodontitis. J Clin Periodontol. 1984 Jan;11(1):63-76. doi: 10.1111/j.1600-051x.1984.tb01309.x.
Tomasi C, Leyland AH, Wennström JL. Factors influencing the outcome of non-surgical periodontal treatment: a multilevel approach. J Clin Periodontol. 2007 Aug;34(8):682-90. doi: 10.1111/j.1600-051X.2007.01111.x
Svärdström G, Wennström JL. Furcation topography of the maxillary and mandibular first molars. J Clin Periodontol. 1988 May;15(5):271-5. doi: 10.1111/j.1600-051x.1988.tb01583.x.PMID: 3164728
Matia JI, Bissada NF, Maybury JE, Ricchetti P. Efficiency of scaling of the molar furcation area with and without surgical access. Int J Periodontics Restorative Dent. 1986;6(6):24-35.
Nordland P, Garrett S, Kiger R, Vanooteghem R, Hutchens LH, Egelberg The effect of plaque control and root debridement in molar teeth. J Clin Periodontol. 1987 Apr;14(4):231-6. doi: 10.1111/j.1600-051x.1987.tb00972.x.PMID: 3294917
Loos B, Nylund K, Claffey N, Egelberg Clinical effects of root debridement in molar and non-molar teeth. A 2-year follow-up. J Clin Periodontol. 1989 Sep;16(8):498-504. doi: 10.1111/j.1600-051x.1989.tb02326.x.PMID: 2778083
Dommisch H, Walter C, Dannewitz B, Eickholz P. Resective surgery for the treatment of furcation involvement: A systematic review. J Clin Periodontol. 2020 Jul;47 Suppl 22:375-391. doi: 10.1111/jcpe.13241.
Langer B, Stein SD, Wagenberg B. An evaluation of root resections. A ten-year study. J Periodontol. 1981 Dec;52(12):719-22. doi: 10.1902/jop.1981.52.12.719.
Bühler H. Evaluation of root-resected teeth. Results after 10 years. J Periodontol. 1988 Dec;59(12):805-10. doi: 10.1902/jop.1988.59.12.805.
Johansson KJ, Johansson CS, Ravald N. The prevalence and alterations of furcation involvements 13 to 16 years after periodontal treatment. Swed Dent J. 2013;37(2):87-95.
Salvi GE, Mischler DC, Schmidlin K, Matuliene G, Pjetursson BE, Brägger U, Lang NP. Risk factors associated with the longevity of multi-rooted teeth. Long-term outcomes after active and supportive periodontal therapy. J Clin Periodontol. 2014 Jul;41(7):701-7. doi: 10.1111/jcpe.12266. Epub 2014 May 26.
Graziani F, Gennai S, Karapetsa D, Rosini S, Filice N, Gabriele M, Tonetti M. Clinical performance of access flap in the treatment of class II furcation defects. A systematic review and meta-analysis of randomized clinical trials. J Clin Periodontol. 2015 Feb;42(2):169-81. doi: 10.1111/jcpe.12327.
Tomasi C, Wennström JL.J Periodontol. Locally delivered doxycycline as an adjunct to mechanical debridement at retreatment of periodontal pockets: outcome at furcation sites. J Periodontol. 2011 Feb;82(2):210-8. doi: 10.1902/jop.2010.100308.
Suvan J, Leira Y, Moreno Sancho FM, Graziani F, Derks J, Tomasi C. Subgingival instrumentation for treatment of periodontitis. A systematic review. J Clin Periodontol. 2020 Jul;47 Suppl 22:155-175. doi: 10.1111/jcpe.13245.
Knöfler GU, Purschwitz RE, Jentsch HF. Clinical evaluation of partial- and full-mouth scaling in the treatment of chronic periodontitis. J Periodontol. 2007 Nov;78(11):2135-42. doi: 10.1902/jop.2007.070010.
Dannewitz B, Zeidler A, Hüsing J, Saure D, Pfefferle T, Eickholz P, Pretzl B. Loss of molars in periodontally treated patients: results 10 years and more after active periodontal therapy. J Clin Periodontol. 2016 Jan;43(1):53-62. doi: 10.1111/jcpe.1
1) La Universidad Dental de Nippon, Escuela de Odontología de la Vida, Departamento de Periodoncia
2) Clínica Dental Wada
3) Escuela de Odontología de la Universidad de Meikai, División de Ciencias de Biomateriales Dentales, Departamento de Ciencias Restaurativas y biomateriales
4) Clínica Dental Heartful
5) Clínica Dental Aoba
6) Matsumoto dental universidad departamento de ciencias dentales y materiales
7) Clínica Dental Mieji
8) Iryo Hojin Shikyoukai, Clínica Dental Yabuki
9) Clínica Dental Fukuda
Antcedentes: Generalmente se dice que los dientes con afectación por furcación tienen mal pronóstico, que, en muchos casos, el tratamiento es difícil de administrar. Este estudio se realizó con el objetivo de evaluar retrospectivamente el tratamiento periodontal no quirúrgico sobre la afectación de la furcación.
Métodos: 133 molares de 80 pacientes con periodontitis en estadio 3-4, edades promedio de 56±10,6 con afectación de furcación, fueron sometidos a este estudio. Todos estos pacientes han completado la terapia periodontal no quirúrgica. Los sujetos con afectación de furcación en la superficie de los dientes de una sola raíz o la superficie plana de los molares en condiciones previas al tratamiento se colocaron en el grupo de control. Los exámenes de tejido periodontal, que incluyeron aquellos para la afectación de la furcación, se realizaron en arcos completos de todos los pacientes y todos los pacientes recibieron instrucciones de higiene oral. Además, se realizó detartraje supragingival y un raspado y alisado radicular, y se realizaron reevaluaciones en todos los pacientes. Se realizó comparación entre el índice de afectación de furcación preoperatorio y postoperatorio, comparando el sondaje de profundidad de la bolsa, sangrado al sondeo y la formación de placa de los del grupo control.
Resultados: Tras la realización de la terapia periodontal inicial, se observó cierre de la furcación en el 20% de los casos, un 3.5% de medición de furca clase II y no se observó cierre de defectos de furcación de clase III. El 20% de los casos de afectación de furcación de clase III mejoraron a niveles de clase II o inferiores. La PPD media en la superficie del diente con afectación de furcación mejoró en 0.7m, mostrando una diferencia significativa con respecto a la del grupo de control que mejoró en 1.2mm en promedio. En los casos de clase I y clase II, no hubo mejoría significativa en el parámetro clínico en comparación con el grupo control. No se observó mejoría significativa en los casos de clase III. Principalmente en áreas con PPD previa al tratamiento de 6 mm o más, se observó una diferencia significativa de la del grupo control solo en los casos de clase III.
Conclusión: Si bien el tratamiento periodontal no quirúrgico tuvo un efecto limitado sobre el cierre de la furcación, se encontró mejoría de los parámetros clínicos en otras áreas en casos no de clase III. Por lo tanto, el tratamiento periodontal no-quirúrgico sería un enfoque válido como paso inicial en el tratamiento de la afectación de la furcación.
Palabras clave: terapia periodontal no quirúrgica, afectación de la furcación, estudio retrospectivo
I. Introducción
La periodontitis es una enfermedad crónica inducida por la formación de biopelículas en la superficie de los dientes. Por lo tanto, la eliminación de la biopelícula de la superficie de los dientes sería el enfoque terapéutico primario, eliminando así la causa de la enfermedad. Al inicio del tratamiento, se proporcionarían instrucciones de higiene bucal y se realizaría un desbridamiento subgingival, lo que arrojaría resultados positivos en un número sustancialmente mayor de dientes de raíces individuales.1,2 Sin embargo, se han reportado mejoras mínimas en los parámetros clínicos de profundidad de bolsa al sondeo (PPD) y nivel de inserción clínica ("CAL") de dientes de múltiples raíces.3 La anatomía compleja del área de furcación de los molares plantea un desafío para la eliminación completa de los depósitos y, además, se informa que conduce a resultados de tratamiento inferiores en comparación con los de las superficies más lisas.4-7
En tales circunstancias, la terapia de resección radicular se ha empleado ampliamente ya que la terapia periodontal no quirúrgica y los procedimientos de colgajo de acceso se consideraron insuficientes. Sin embargo, los estudios han demostrado que tales tratamientos no mejoran el pronóstico a largo plazo de los pacientes en todos los casos.8 En un número significativo de casos, se ha reportado fractura radicular, lesión endodóntica y desprendimiento de la prótesis como causa de mal pronóstico.9,10 Por lo tanto, estos tratamientos pueden aumentar el riesgo de complicaciones tecnológicas y / o síntomas accidentales causados por factores mecánicos en lugar de mejorar la higiene bucal.
Un enfoque válido sería seleccionar tratamientos que preserven el tejido dental en la mayor medida posible en lugar de seleccionar activamente la resección radicular como el tratamiento de primera elección. Johansson et.al., 11 reportaron que dos tercios del molar con afectación de furcación se conservaron.13-16 años después de que se realizaron los tratamientos periodontales. Además, Salvi et.al.,12 afirmó que, durante el período de mantenimiento promedio de 11 años, el riesgo de perder un diente con afectación de furcación de Clase I fue de aproximadamente 1,2 veces más en comparación con un diente sin afectación por furcación, mostrando un pronóstico positivo.
De acuerdo con la revisión sistemática de Graziani et.al., se mostró una mejoría clinicamente significativa como resultado de la realización de procedimientos de colgajo de acceso en casos de afectación de furcación de Clase II.13 Tomasi y Wennström et.al.,14 afirmaron que se logró un cierre total o parcial en el 25-38% de las áreas en los casos de afectación de furcación de Clase I y Clase II después de que los dispocitivos ultrasónicos se usaron solos o con la administración local de fármacos antibacterianos en la terapia periodontal no quirúrgica. Sin embargo, la información sobre los resultados del tratamiento periodontal no quirúrgico para los diferentes tipos de afectación de la furcación es limitada. Este estudio se realizó para evaluar retrospectivamente el efecto del tratamiento periodontal no quirúrgico en varios tipos de afectación de la furcación.
II. Materiales y métodos
El Comité de Ética de la Academia de Odontología Clínica avaló el protocolo c antes de realizar este estudio. En este estudio, se analizaron los datos de pacientes que presentan un periodonto con afectación de tipo amplio o furcación localizada de clase I, II y III en el primer molar o el segundo molar, periodontitis etapa 3 o superior, grado B o superior entre abril de 2011 y marzo de 2021 en 7 clínicas diferentes. La información del paciente y los resultados clínicos se extrajeron de los registros médicos de los pacientes que completaron el proceso de reevaluación después de recibir al menos un tratamiento básico (tratamiento periodontal no quirúrgico). Los criterios de inclusión y los criterios de exclusión son los siguientes.
Criterios de inclusión
・Edades 30-70 en el momento de la presentación inicial
・20 o más dientes restantes
・Es posible confirmar los resultados de las pruebas y las fotos de rayos X del tejido periodontal antes del tratamiento básico.
・Posibilidad de confirmar los resultados de la prueba del tejido periodontal en el momento de la reevaluación después del tratamiento básico.
・Se puede observar una afectación de furca con 4mm o más de PPD en la superficie molar.
Se excluyeron los pacientes y dientes con cualquiera de los siguientes criterios aplicables.
Criterios de exclusión
・Pacientes con enfermedades sistémicas que afectarán los resultados del tratamiento.
・Los dispositivos de restauración y/o aparatos de ortodoncia que afectan los resultados del tratamiento se colocan en el área de furcación
・Patología periapical no resuelta hasta el momento de la reevaluación.
・Imposibilidad de confirmar los resultados de las pruebas y las fotos de rayos X de los tejidos periodontales antes del tratamiento básico
・No se pueden confirmar los resultados de las pruebas de los tejidos periodontales después del tratamiento básico
・Los cambios que probablemente se vean afectados por terceras molares
・Dientes que fueron extraídos en el momento de la reevaluación
Además de los resultados de las pruebas de los tejidos periodontales, el estado de tabaquismo o no fumador, se registraron los hallazgos sistémicos. Los siguientes parámetros clínicos se registraron en el momento de la reevaluación, 2 meses o más después de la presentación inicial de cada paciente (antes del tratamiento básico: BL) y el tratamiento básico de las áreas involucradas en la furcación (intrucciones sobre el cepillado, desbridamiento subgingival con curetas o instrumentos ultrasónicos).
・Formación de placa
・Grado de cambios patológicos en el área de furcación (clasificación de Lindhe & Nyman)
・PPD (mm) de la superficie del diente en el área de furcación
・Sangrado al sondeo en el momento de sondear el área de furcación (BOP)
・Movilidad
・Registros radiográficos en el momento del diagnóstico inicial
Además, los parámetros de PPD y BOP similares de un diente adyacente, diente monorradicular o una superficie lisa de un molar de los mismos pacientes, si existieran, se registraron como los del grupo control.
Análisis de los datos
En este estudio, se seleccionó la mejora del área involucrada en la furcación se usó como puntuación por clases como el criterio de valoración primario, seguido del análisis de la mejora en ppD, BOP, formación de placa de la superficie dental en el área involucrada en furcación como criterio de valoración secundario.
Las áreas de furcación se clasificaron como clases I, II y III en el momento de BL y, además, se calcularon las clases en el momento de la reevaluación y/o la frecuencia de cierre.
Se calculó el valor promedio, la frecuencia y la desviación estándar en PPD, BOP, placa para las áreas generales involucradas en la furcación y los grupos de control, seguidos del cálculo del valor promedio y la desviación estándar correspondientes a cada clase y cada grupo de control. Los cálculos se realizaron de manera similar para PPD de 4-5mm y 6mm o más en el momento de BL. La DP en el momento de la BL era de 4.5mm en solo dos casos de afectación de furcación de clase III y, por lo tanto, se sometió a un análisis combinado con casos de clase II. Se realizaron pruebas T, que son adecuadas para identificar los cambios de BL a reevaluación de cada grupo para PPD. La prueba t de Studen t se utilizó para analizar los datos de cada grupo en el momento de la BL y la reevaluación, y los cambios desde el momento de la BL en comparación con el momento de la reevaluación. Para el análisis multigrupo se utilizaron análisis de varianza y pruebas SNK.
Se realizó una comparación sobre la BOP y la formación de placa con las pruebas x2 en el momento de la BL versus la reevaluación.
III. Resultados
Características de los sujetos en el momento de BL
Las características de los pacientes en el momento de la BL se muestran en la Tabla 1. Se recogieron datos de pacientes periodontales, edades promedio de 56.0 (DE 10.6) de 80 sujetos (47 mujeres). La Tabla 2 muestra la agrupación de los dientes involucrados en la furcación que formaron parte de este estudio. El número de dientes ascendió a 133, de los cuales 40 dientes eran de clase I, 57 dientes eran de clase II y 36 dientes eran casos de clase III. La superficie lisa de 80 dientes sin afectación de furcación se colocó en el grupo de control.
(Tabla 1) Características de los pacientes en el momento de BL(Tabla 2) Distribución de los dientes afectados en el momento de BL
Resultados del tratamiento
La Fig.1 muestra los resultados del tratamiento de los casos de afectación de furcación de clase 1. La tasa global de cierre fue del 20%, con un 25% en el region maxilar y un 16.7% en la región mandibular. Del mismo modo, en los casos de clase II, la tasa general de cierre fue del 3.5% y el 12.3% mejoró a la clase I. La tasa de cierre o la tasa de mejora a la clase I fue del 24.1% en la región maxilar y del 7.2% en la región mandibular (Fig.2). No se encontró un cierre completo en los casos de clase III, mientras que la tasa de mejora general a la clase 2 fue del 6.3% y la clase 1 fue del 3.1%. No se encontró mejoría a la clase 1 en el área mandibular (Fig.3).
(Fig.1) % de distribución luego de tratamiento en furcas grado I(Fig.2) % de distribución luego de tratamiento en furcas grado II(Fig.3) % de distribución luego de tratamiento en furcas grado III
La Tabla 3 ilustra los cambios en el parámetro clínico de la sección transversal del área de furcación y la superficie de los dientes del grupo de control. La frecuencia de la BOP en el momento de la BL fue baja en el grupo de control, mostrando diferencias estadísticamente significativas, mientras que no se encontraron diferencias estadísticamente significativas en los números paramétricos de la BL en otras áreas entre los grupos. La BOP y la frecuencia de la placa disminuyeron significativamente en ambos grupos. El PPD promedio del grupo de control se redujo en 1.2mm en promedio, que fue más alto que los 0.7mm del grupo de participación de furcación, lo que hace que la diferencia sea estadísticamente significativa.
En el análisis de la afectación de la furcación por clase, no se encontraron diferencias estadísticamente significativas en cada parámetro clínico en todos los grupos en el momento de la BL. Se observó una mejoría estadísticamente significativa en la formación de placa en los grupos de clase I-III. Se mostró una mejoría significativa en la frecuencia de la BOP para los grupos de clase I y II antes y después del tratamiento, mientras que no se apreció una mejoría significativa en el grupo de clase III. Se observaron tendencias similares en los grupos control (Tablas 4-6). En promedio, se realizó una mejoría significativa en los grupos I y II, mientras que no se encontraron diferencias estadísticamente significativas en comparación con el grupo control. En los casos de clase III, los cambios entre BL y reevaluación fueron de 0.1mm en promedio, sin mostrar diferencias estadísticamente significativas. La mejoría en el grupo de control fue de 1.4 mm en promedio, exhibiendo una diferencia estadísticamente significativa.
La Tabla 7 ilustra los cambios en el parámetro clínico de cada grupo cuando la PPD era de 4-5mm en BL. No se observaron diferencias significativas en los parámetros clínicos entre los grupos en BL. Se observaron mejoras significativas en las placas en el grupo de control y el grupo de clase I, mientras que no se observaron cambios significativos en los grupos de clase II y III. No se encontraron diferencias significativas en la mejoría de la PPD entre los 3 grupos. La Tabla 8 muestra los resultados del análisis de PPD con 6mm o más en BL. No se mostraron diferencias significativas en los parámetros clínicos entre los grupos en BL. En la frecuencia de la placa y BOP, se observó una mejoría significativa en los grupos de control, los grupos de clase I y clase II, mientras que no se observó ningún cambio significativo en el grupo de clase III. El grupo de control y el grupo de clase II tuvieron una mejoría mayor que el grupo de clase III en PPD promedio, exhibiendo diferencia estadísticamente significativa.
(Tabla 3) Parámetros de la superficie de los dientes afectados por la furcación y la superficie de los dientes del grupo control en BL y reevaluación(Tabla 4) Parámetros de la superficie de los dientes de clase I afectados por la furcación y la superficie de los dientes del grupo controlado en BL y reevaluación(Tabla 5) Parámetros de la superficie de los dientes de clase II involucrados en la furcación y la superficie de los dientes del grupo controlado en BL y reevaluación(Tabla 6) Parámetros de la superficie de los dientes de clase III involucrados en la furcación y la superficie de los dientes del grupo controlado en BL y reevaluación(Tabla 7) Parámetros de superficie de los dientes con PPD de 4-5mm en BL, en el momento de BL y reevaluación(Tabla 8) Parámetros de superficie de los dientes con PPD de 6 mm o más en BL, en el momento de BL y reevaluación
IV. Observación
En los resultados retrospectivos de la investigación, se logró el cierre completo por tratamiento no quirúrgico en el 20% de los casos de la clase I, el 3.5% en la clase II y el 0% en la clase III. El 15.8% de los casos de clase II y el 9.4% de los casos de clase III mejoraron a clase I o inferior. Tales resultados indican que el cierre completo de las áreas afectadas por la furcación mediante tratamiento no quirúrgico es difícil de lograr en casos de clase II o superiores. Además, la mejora del cierre al nivel de clase I se produjo solo en un número limitado de casos. La investigación realizada por Salvi et.al12 en un período promedio de seguimiento de 11.5 años indicó que el riesgo de perder un diente durante el período de mantenimiento periodontal para los casos de afectación de furcación de clase I era equivalente a 1.17 veces con poca diferencia estadísticamente significativa y, por lo tanto, los casos de furca clase I no representan el riesgo de pérdida de dientes. Tales resultados muestran que el "cierre parcial" del nivel de clase I puede servir como un objetivo de tratamiento. Tomasi y Wennström14 reafirmaron que como resultado de la implementación del tratamiento periodontal no quirúrgico en el 38% de los casos de afectación de furcación de clase I, se logró el cierre completo, y en los casos de clase II, el 25% tuvo cierre parcial o cierre completo. Si bien la razón de esta mayor tasa de cierre en comparación con la de nuestro estudio no está clara, las diferencias en el control de placa, la forma anatómica y las restricciones de tiempo pueden ser los factores que afectan los resultados. Sin embargo, en nuestro estudio, si bien la tasa de cierre fue menor, ningún caso se ha deteriorado y, por lo tanto, se pensó que valía la pena implementar terapias no quirúrgicas en la etapa inicial del tratamiento. Además, el estudio realizado por Tomasi y Wennström14 indica que la afectación de la furcación mejora aún más al repetir los tratamientos no quirúrgicos y, por lo tanto, es probable que dicho enfoque sea efectivo.
En este estudio, se utilizaron como grupo de control datos sobre dientes de raíz única o superficie lisa de molares con PPD restante equivalente a PPD o superficie de dientes afectados por furcación. Los resultados del tratamiento periodontal no quirúrgico de la superficie de los dientes de una sola raíz y la superficie lisa de los molares no son diferentes, la unión de estos dientes en un grupo de control probablemente esté justificada.6,7 Tener un sujeto cuya superficie de furca restante no coincidía exactamente con el número de dientes y de superficie corta de raíces que mostraban un parámetro clínico similar planteó un límite en este estudio que fue diseñado para ser un estudio retrospectivo.
Se realizó una mejora promedio de 1.2mm en la PPD de la superficie de los dientes del grupo control mediante tratamiento no quirúrgico. El metanálisis en la revisión sistemática de Suvan et.al.,15 mostró la mejora de PPD por SRP fue de 1.38mm en promedio. Dado que la diferencia con los resultados de nuestro estudio es mínima, es probable que los resultados de SRP del grupo de control en nuestro estudio estén cerca del promedio generalmente aceptado. La reducción de PPD en la superficie de los dientes con afectación de furcación midió 0.7mm en promedio, mostrando una diferencia estadísticamente significativa con respecto a la del grupo de control. Nordland et.al., indicó que si la PPD antes del tratamiento era de 4.5mm o más, en comparación con los no molares con afectación de la furcación y superficie lisa de los molares, la reducción de la PPD por tratamiento no quirúrgico sería menor.6 Los resultados se explican en parte por una mayor formación de placa en el área de furcación. Sin embargo, en este estudio, no se observaron diferencias en la tasa de formación de placa entre el grupo de afectación de furcación y el grupo de control. En un estudio realizado por Knöfler et.al., compararon los resultados de SRP en arco completo y SRP en cada cuadrante,16 mientras que PPD de la superficie de los dientes involucrados con la furcación fue de 4-6mm antes del tratamiento, la reducción de PPD después del tratamiento no quirúrgico en la superficie de los dientes involucrados con la furcación fue de 0.9-1.0mm, y en superficie lisa 1.0-1.3mm. La BOP en la superficie de los dientes que exhiben furcación mejoró en aproximadamente un 30%, produciendo resultados similares a los de nuestro estudio. Por lo tanto, para evaluar los resultados del tratamiento de la afectación de la furcación, se debe considerar el valor de PPD antes del tratamiento.
En este estudio, la implicación de la furcación en el momento de la presentación inicial se analizó por grado. Los resultados del tratamiento de sólo los casos de afectación de furcación de clase III fueron menos efectivos en comparación con los del grupo de control, lo que probablemente afectó a todos los resultados de los casos de afectación de furcación. Se desconoce el grado de afectación de la furcación en el estudio de Nordland et.al.6 con una alta probabilidad de que el grado de afectación de la furcación antes del tratamiento difiera de la de los sujetos de nuestro estudio. En el estudio realizado por Tomasi y Wennström14, el tratamiento periodontal no quirúrgico único sobre la afectación de la furcación de clase I y II dio como resultado una reducción de la PPD con un promedio de 1.1-1.3mm, que fue similar a los resultados del tratamiento de Nordland et.,al.6 En nuestro estudio, la reducción de la PPD promedió 0.8mm en los casos de clase I y 1.1mm en los casos de clase II. Los números ligeramente más bajos en comparación con los resultados del tratamiento en el estudio anterior pueden explicarse parcialmente de la siguiente manera: en los datos de Tomasi y Wennström14 por ejemplo, PPD antes del tratamiento en la clase I fue un promedio de 5.8mm y en la clase II, 7.1mm, mientras que, en nuestro estudio, la clase I promedió 5.5mm y la clase II 6.4mm.
En nuestro estudio, cuando la PPD fue de 6mm o más en la superficie de los dientes de los casos de furcación de clase III, no se mostró una mejoría significativa en comparación con otros grupos. Una razón es probable que sea que la mejora en el control de la placa en tales áreas fue del 15%, que fue limitada en comparación con otros grupos. Dannewitz et.al.,17 rafirmó que como resultado del tratamiento de 4 dientes de 67 dientes de clase III relacionados con la furcación solo con SRP, se perdieron 3 dientes en un período de 5 años, mientras que 9 de los 62 dientes se perdieron por el tratamiento quirúrgico, incluida la resección radicular, terapia regenerativa, cirugía de colgajo. En los casos de afectación por furcación de clase III con PPD profunda, el tratamiento periodontal no quirúrgico tuvo un efecto limitado como tratamiento y, por lo tanto, se deben considerar otras modalidades de tratamiento, incluida la extracción de dientes, en los planes de tratamiento.
Este estudio es de carácter retrospectivo realizado por múltiples instalaciones y, por lo tanto, el proceso que incluye la repetibilidad de las pruebas, los protocolos de tratamiento estandarizados y las diversas limitaciones de tiempo, puede no haber sido lo suficientemente estandarizado. Por ejemplo, cuando la PPD no mejoró en los casos de afectación de furcación de clase III, se observó una mejoría a otra clase, que puede deberse a la regresión a la media. La participación de furcación en sí misma puede haber sido infravalorada debido a sesgos de detección. Es necesario confirmar los resultados de nuestro estudio en estudios prospectivos a mayor escala en un futuro próximo.
V. Conclusión
Los tratamientos periodontales no quirúrgicos tienen una efectividad limitada en el cierre de áreas de furcación, mientras que se obtuvieron parámetros clínicos mejorados en otras áreas, excepto en los casos de clase III. Por lo tanto, los tratamientos no quirúrgicos serían un enfoque válido como tratamiento inicial. Se necesita investigación adicional a mayor escala para confirmar los resultados de dicha investigación en un futuro próximo.
Referencias
Badersten A, Nilvéus R, Egelberg J. Effect of nonsurgical periodontal therapy. I. Moderately advanced periodontitis. J Clin Periodontol. 1981 Feb;8(1):57-72. doi: 10.1111/j.1600-051x.1981.tb02024.x.
Badersten A, Nilveus R, Egelberg. Effect of nonsurgical periodontal therapy. II. Severely advanced periodontitis. J Clin Periodontol. 1984 Jan;11(1):63-76. doi: 10.1111/j.1600-051x.1984.tb01309.x.
Tomasi C, Leyland AH, Wennström JL. Factors influencing the outcome of non-surgical periodontal treatment: a multilevel approach. J Clin Periodontol. 2007 Aug;34(8):682-90. doi: 10.1111/j.1600-051X.2007.01111.x
Svärdström G, Wennström JL. Furcation topography of the maxillary and mandibular first molars. J Clin Periodontol. 1988 May;15(5):271-5. doi: 10.1111/j.1600-051x.1988.tb01583.x.PMID: 3164728
Matia JI, Bissada NF, Maybury JE, Ricchetti P. Efficiency of scaling of the molar furcation area with and without surgical access. Int J Periodontics Restorative Dent. 1986;6(6):24-35.
Nordland P, Garrett S, Kiger R, Vanooteghem R, Hutchens LH, Egelberg The effect of plaque control and root debridement in molar teeth. J Clin Periodontol. 1987 Apr;14(4):231-6. doi: 10.1111/j.1600-051x.1987.tb00972.x.PMID: 3294917
Loos B, Nylund K, Claffey N, Egelberg Clinical effects of root debridement in molar and non-molar teeth. A 2-year follow-up. J Clin Periodontol. 1989 Sep;16(8):498-504. doi: 10.1111/j.1600-051x.1989.tb02326.x.PMID: 2778083
Dommisch H, Walter C, Dannewitz B, Eickholz P. Resective surgery for the treatment of furcation involvement: A systematic review. J Clin Periodontol. 2020 Jul;47 Suppl 22:375-391. doi: 10.1111/jcpe.13241.
Langer B, Stein SD, Wagenberg B. An evaluation of root resections. A ten-year study. J Periodontol. 1981 Dec;52(12):719-22. doi: 10.1902/jop.1981.52.12.719.
Bühler H. Evaluation of root-resected teeth. Results after 10 years. J Periodontol. 1988 Dec;59(12):805-10. doi: 10.1902/jop.1988.59.12.805.
Johansson KJ, Johansson CS, Ravald N. The prevalence and alterations of furcation involvements 13 to 16 years after periodontal treatment. Swed Dent J. 2013;37(2):87-95.
Salvi GE, Mischler DC, Schmidlin K, Matuliene G, Pjetursson BE, Brägger U, Lang NP. Risk factors associated with the longevity of multi-rooted teeth. Long-term outcomes after active and supportive periodontal therapy. J Clin Periodontol. 2014 Jul;41(7):701-7. doi: 10.1111/jcpe.12266. Epub 2014 May 26.
Graziani F, Gennai S, Karapetsa D, Rosini S, Filice N, Gabriele M, Tonetti M. Clinical performance of access flap in the treatment of class II furcation defects. A systematic review and meta-analysis of randomized clinical trials. J Clin Periodontol. 2015 Feb;42(2):169-81. doi: 10.1111/jcpe.12327.
Tomasi C, Wennström JL.J Periodontol Locally delivered doxycycline as an adjunct to mechanical debridement at retreatment of periodontal pockets: outcome at furcation sites. J Periodontol. 2011 Feb;82(2):210-8. doi: 10.1902/jop.2010.100308.
Suvan J, Leira Y, Moreno Sancho FM, Graziani F, Derks J, Tomasi C. Subgingival instrumentation for treatment of periodontitis. A systematic review. J Clin Periodontol. 2020 Jul;47 Suppl 22:155-175. doi: 10.1111/jcpe.13245.
Knöfler GU, Purschwitz RE, Jentsch HF. Clinical evaluation of partial- and full-mouth scaling in the treatment of chronic periodontitis. J Periodontol. 2007 Nov;78(11):2135-42. doi: 10.1902/jop.2007.070010.
Dannewitz B, Zeidler A, Hüsing J, Saure D, Pfefferle T, Eickholz P, Pretzl B. Loss of molars in periodontally treated patients: results 10 years and more after active periodontal therapy. J Clin Periodontol. 2016 Jan;43(1):53-62. doi: 10.1111/jcpe.1