Immediate implant placement in the aesthetic area, surgical and restorative considerations
Fernando COLINDRES1)Rodrigo RIVERA1)Rodrigo CAYARGA1)
1) Department of Advanced Implantology, Faculty of Dentistry, Francisco Marroquín University, Guatemala.
I. Introduction
The aesthetic sector represents a challenge for prosthetic treatment on dental implants, due to the high incidence of soft and bone tissue defects that make multidisciplinary treatment approach mandatory with a team of clinicians whose course of work is governed by an accurate diagnosis, and treatment plan in stages, surgical and restorative.1-3 It is well described in the literature that the starting point for predictable and successful results is the initial diagnosis of the problem to be restored, therefore, knowing the etiology of the defect to be rehabilitated is imperative to achieve the planned objectives in each case. The current documentation offers various classifications of defects according to the presence of teeth whose periodontal, endodontic and/or prosthetic prognosis is hopeless,4-7 such as described by Elian et al.8, and Kan et al,9 and there are classifications of residual bone ridges, those depends in the degree of loss of bone or soft tissue.10-12 Generally, the teeth that must be replaced in this sector present a high level of complexity at different levels, which can be categorized as risk factors, Levine,et al.13 they determined that the first key to success for the placement of immediate implants in the aesthetic area is the aesthetic risk assessment of each patient, and it is this analysis that will determine the surgical technique, selection of regeneration materials, design, type and nature of the final restoration. This case report presents the protocol used for prosthetic rehabilitation on an implant placed immediately after extraction of a tooth with a non-treatable prognosis in the anterior sector using the “dual zone therapeutic concept” surgical technique described by Chu et al.14
II. Case Report
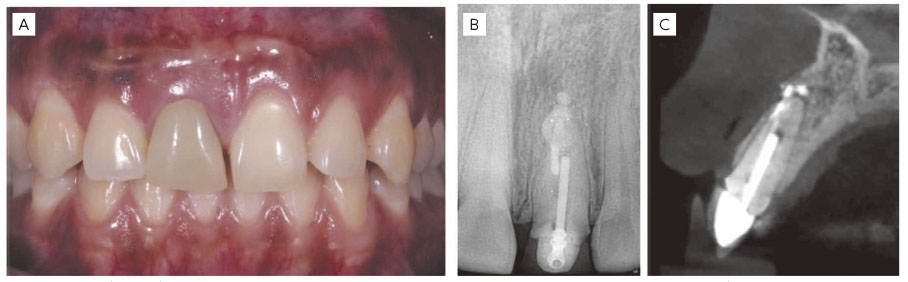
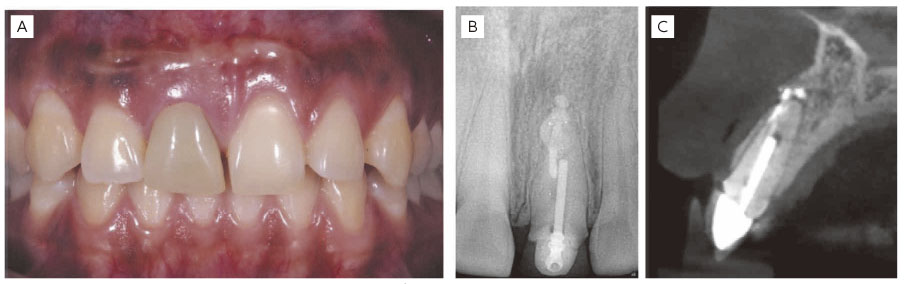
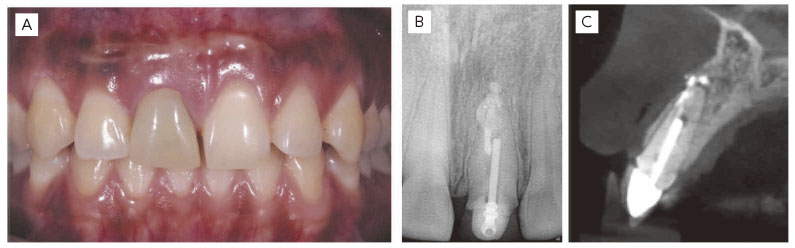
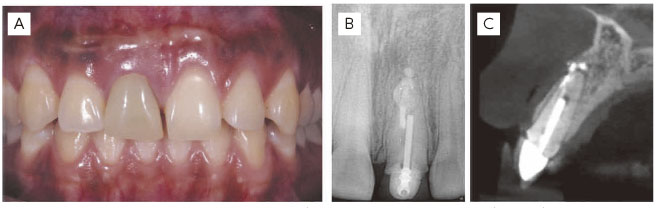
A 22-year-old female patient, systemically healthy, with no history of periodontal disease, presented to the Advanced Implantology Clinic of the Francisco Marroquín University School of Dentistry, for consultation of pain in tooth 8. The clinical evaluation revealed a change in the coloration of the provisional crown, tenderness on palpation, without hemorrhagic exudate, upon removal of the provisional crown caries were observed at the cervical level with the presence of a composite reconstruction supported by a prefabricated post. Radiographic evaluation revealed poor root canal treatment with a history of apicoectomy. Consultation was made with the department of Endodontics to evaluate the possibility of performing a new periapical surgery, with the Department of Periodontology and Restoration to evaluate the possibility of performing a functional coronary lengthening surgery, however, due to the unfavorable crown-root ratio, presence of cervical caries and presence of previous failed endodontic treatments, it was concluded that the best option for this case was extraction and performing and immediate implant placement.
(Fig. 1) A. Teeth 8 with poor provisional crown. B. Poor root canal treatment. C. Type 1 socket according to Elian et al,8 type 1 Kan et al.9
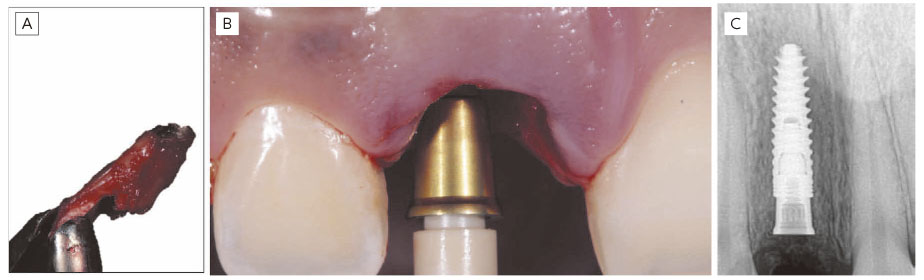
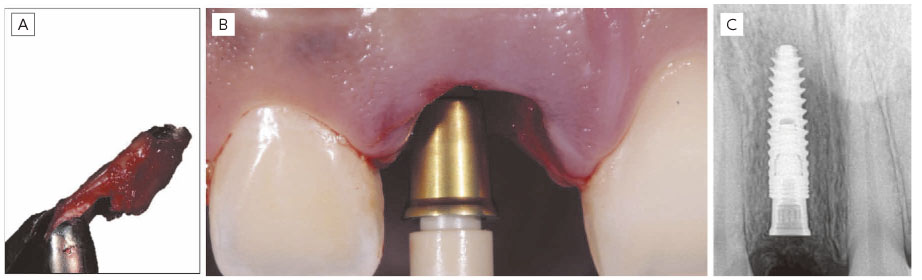
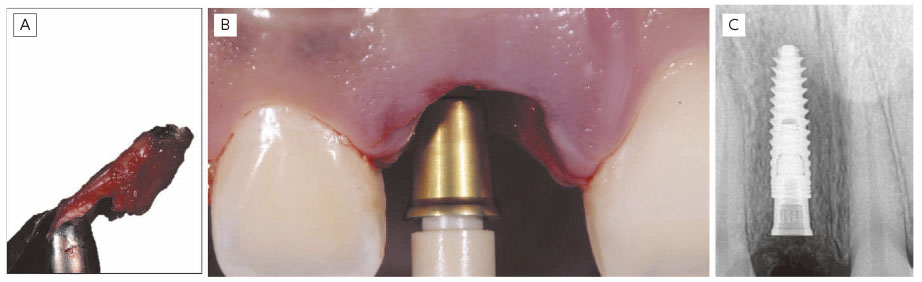
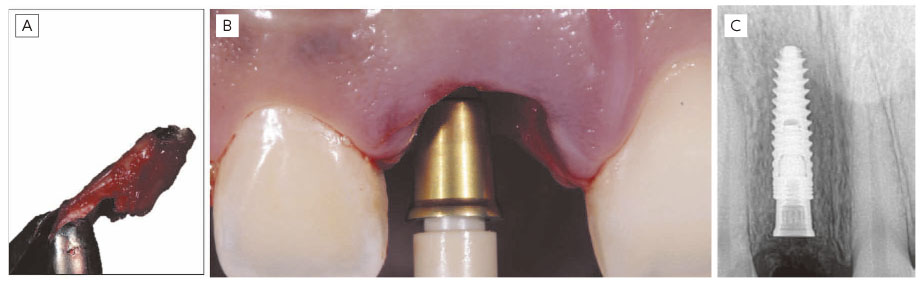
The minimally traumatic extraction of tooth 8 was performed with periotomes, curettage and disinfection of the socket, subsequently the integrity of the buccal bone table and distance between free gingival margin and buccal plate of 3mm was confirmed with a periodontal prob e to proceed with the immediate placement of the implant. A 3.75 × 11.5mm MIS C1 conical connection implant was placed with 45Ncm insertion torque. In addition, a 4mm MIS CONNECT transmucosal abutment with 30Ncm insertion torqu e was used to move the implant-prosthetic abutment interface away from the marginal bone crest(Fig.2).
(Fig. 2) A. Minimally traumatic extraction B. Placement of immediate implant and MIS CONNECT transmucosal abutment. C. Final implant position.
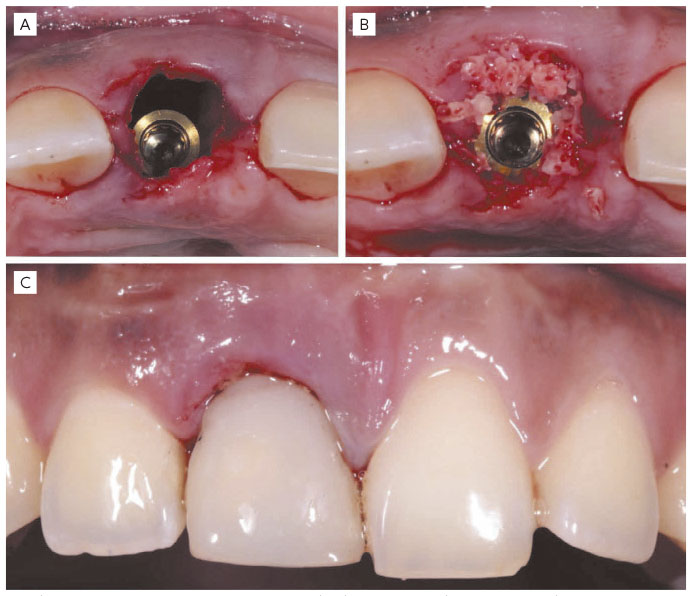
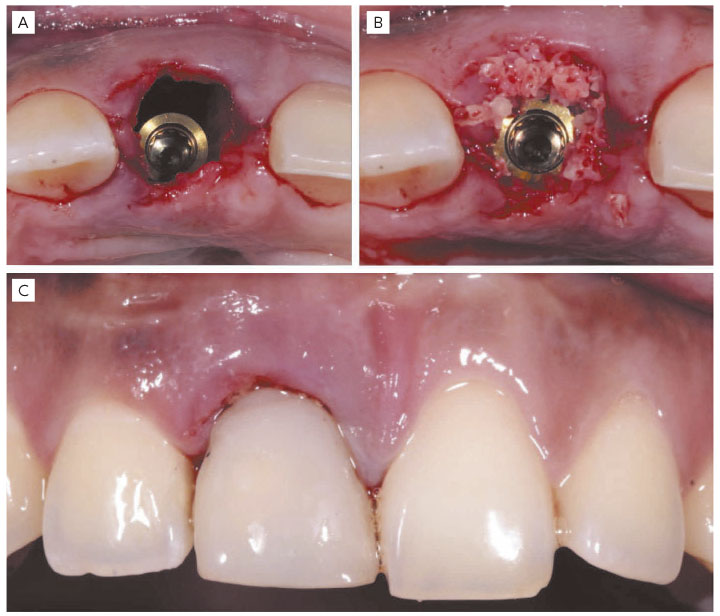
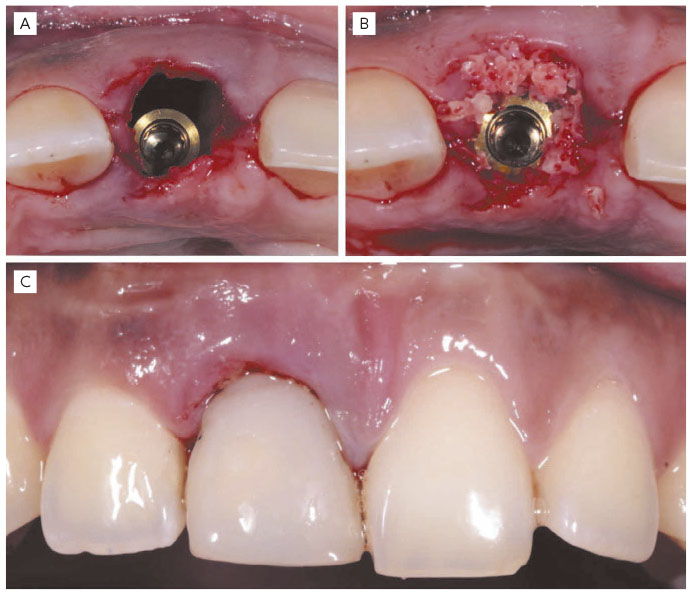
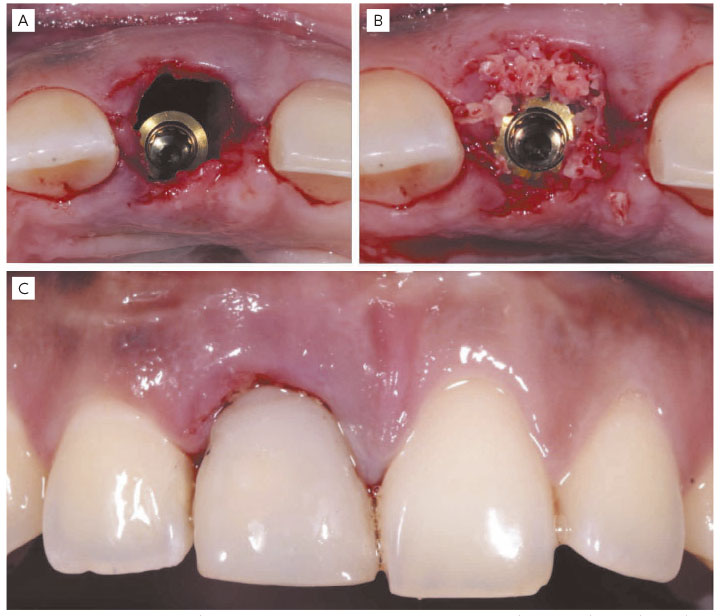
The implant was placed in a palatal position with respect to the clinical crowns of the adjacent teeth, following the “dual zone” concept, a bone graft was performed in the buccal gap between implant and buccal bone wall with a medium particle xenograft hydrated in saline solution (Bonefill ® Dense [0.10 - 0.60mm] (Fine) 0.50 g • 0.50 DC. Bionnovation Biomedical, Bauru, Brazil.). The fixed provisional was immediately performed on a PEEK temporary abutment without occlusal contact(Fig.3).
(Fig. 3) A. Implant placed in palatal position. B. Xenograft placed in buccal gap of bone tissue and soft tissue. C. Provisional screw-retained crown without occlusal contact.
Postoperative care included antibiotic therapy with Amoxicillin 500 mg. every 8 hours for 7 days. Oral anti-inflammatories Dexketoprofen 25 mg. Every 8 hours for 5 days. Mouthwashes with 0.12% Chlorhexidine Gluconate 3 times a day for 15 days. Recommendations on oral hygiene in the surgical area and soft foods. A postoperative control was carried out in the first week, 15 days, and after 4 months, the rehabilitation stage was carried out(Fig.4).
(Fig. 4) A. Postoperative situation at 1 week. B. Postoperative tomographic section of 1 week
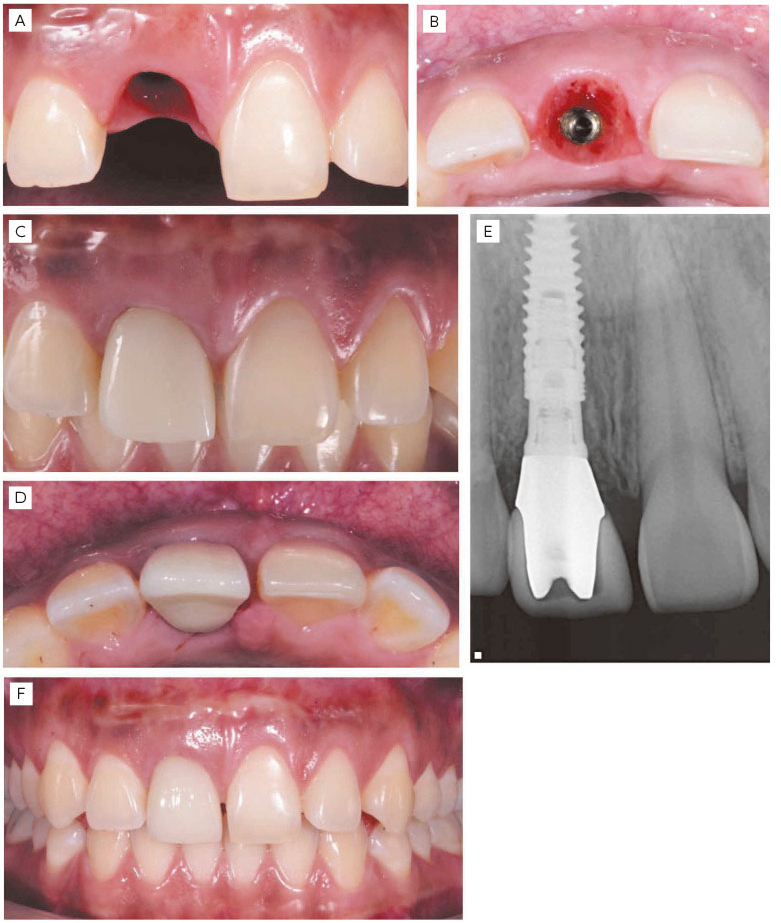
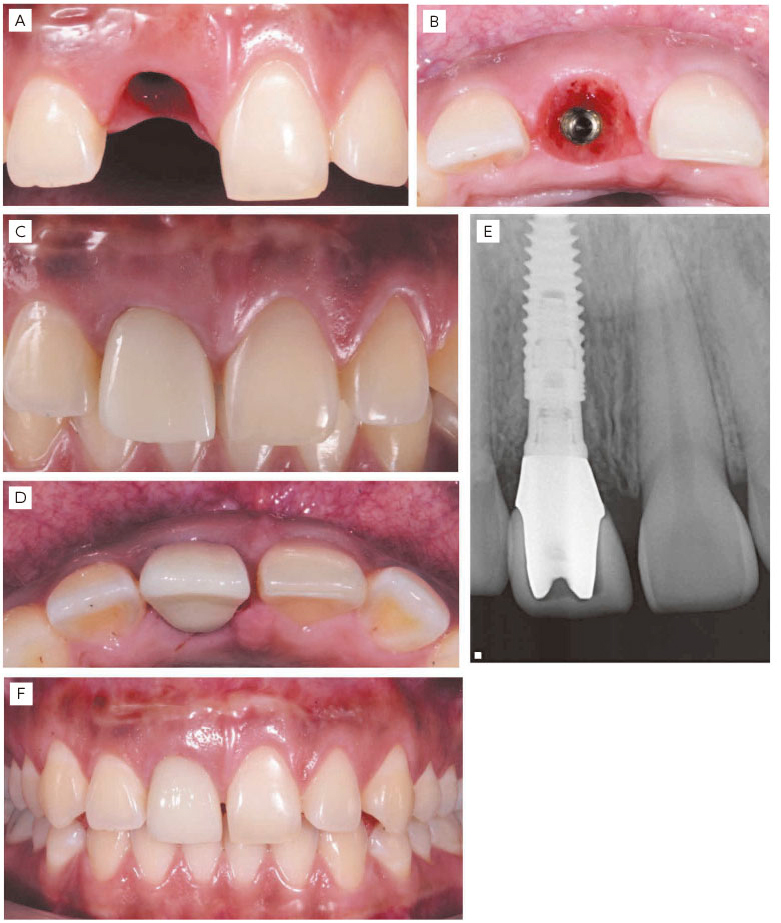
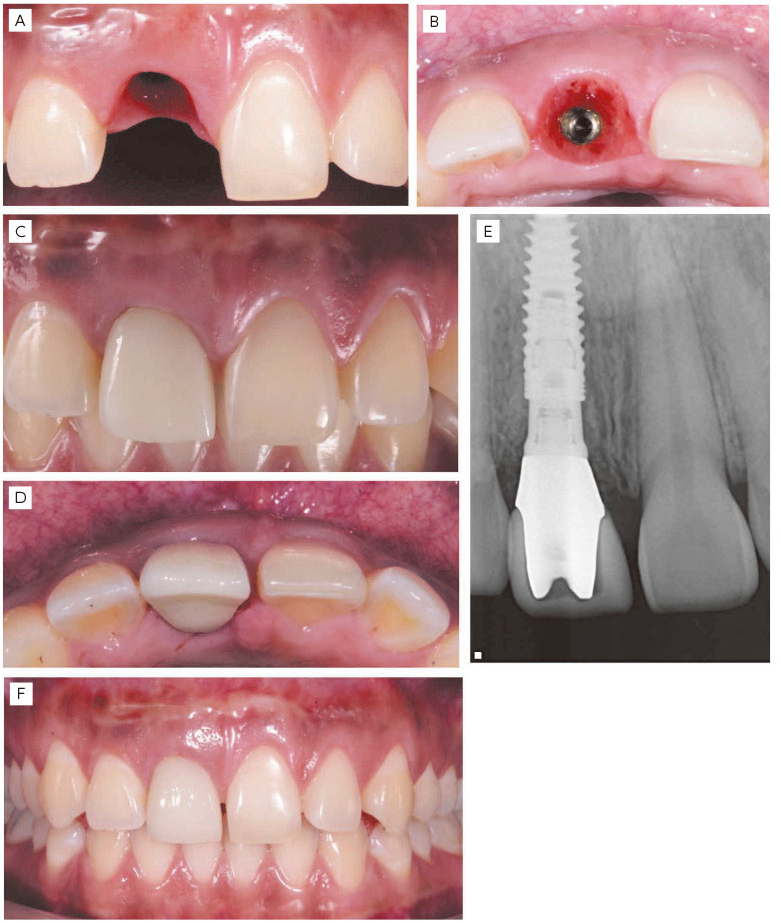
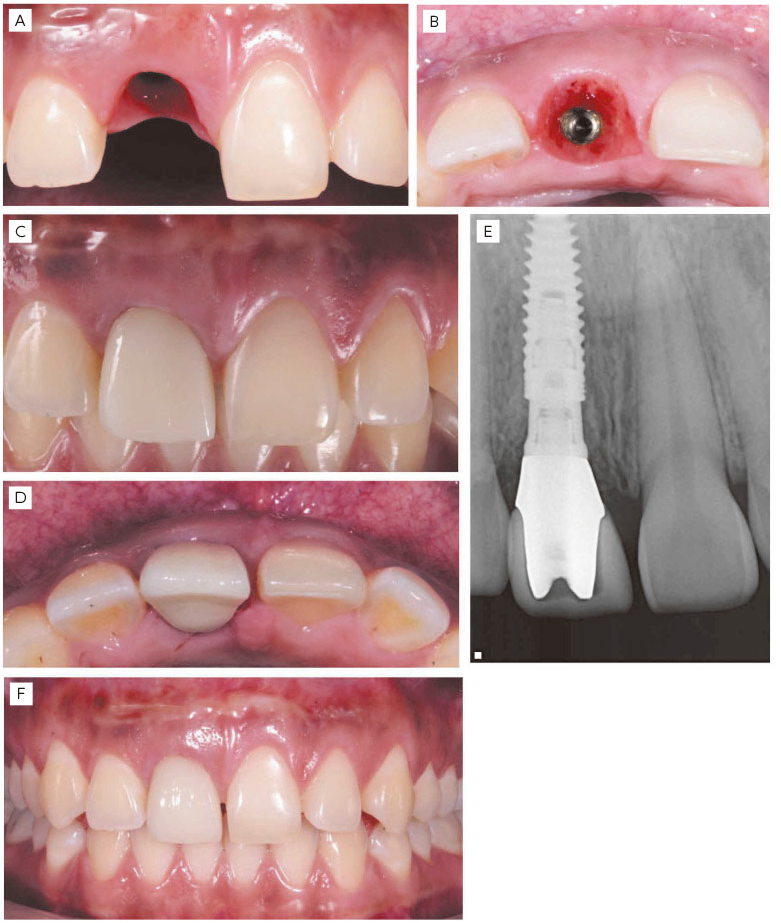
Due to the buccal inclination of the implant, it was decided to perform a cemented crown using a custom zirconia prosthetic abutment. The final crown was made of EMAX lithium disilicate (Ivoclar Vivadent AG, Liechtenstein), which was cemented under the cementation protocol described by Seo & Seo.15 A 6-month follow-up was performed to confirm the integrity of the peri-implant tissues and patient satisfaction(Fig.5).
(Fig. 5) A-B. 4 months postoperative.
C-D Final cemented restoration.
E. Immediate radiographic control of final crown cementation.
F. Control 6 months after prosthetic rehabilitation.
III. Discussion
The extraction of teeth triggers a process of catabolic changes within the periodontal tissues, resulting in a decrease in the height and thickness of the bone tissue available for the placement of dental implants,16,18-20 as well as functional and aesthetic problems for the patient.17 The degree of tissue reabsorption directly depends on the periodontal phenotype, thin bone phenotypes, less than 1 mm thick in the buccal table, the most affected in terms of progressive loss of tissue in both height and thickness.18-20 When carrying out an extraction and immediate implant placement, these catabolic changes are not nullified, but can be modified by biomaterials that act as a scaffold for bone formation at the residual ridge implant interface.4, 21-23 The success rate of immediate implants compared to conventionally placed implants is similar, however in immediate implant cases, the anatomical factors present (phenotype, presence of periapical pathology, available tissue), surgical factors (surgical technique, use of bone grafts, connective tissue) and prosthetic factors (immediate provisionalization, type of restorative material) play a key role in achieving the treatment goals in the short term, and more importantly, in the long term.14, 23 The “dual zone” concept addresses three fundamental principles to manage type I sockets according to Elian et al., with the main objective of minimizing and preserving the greatest amount of periodontal architecture existing in the dental implant treatment site.14, 23-25 These principles are defined as minimally traumatic extraction of the tooth, placement of the implant without elevation of the mucoperiosteal flap, in a suitable three-dimensional location with the use of biomaterials in both areas, soft tissue and bone tissue,26 and use of a fixed provisional as a sealing device to hold the bone graft in place. This case report was carried out under the guidelines of this concept of two important areas of dimensional changes, thus important concepts that have been previously described in the literature for the success of dental implant therapy and maintenance of peri-implant tissues were also considered long-term, such as the use of xenograft as a biomaterial with a low resorption rate and inflammatory response,22.26 use of conical connection and the MIS CONNECT transmucosal abutment to translate the platform-prosthetic abutment interface of the marginal bone crest,27-29 and selection of highly aesthetic inert restorative materials.30 It is important to emphasize that the decision to use a surgical technique depends on several factors, of which the initial diagnosis is key for the predictability of the treatment. Diagnosis should be based on the detailed clinical and radiographic evaluation, etiology of the defect, systemic state, collaboration, and aesthetic requirements of the patient.
IV. Conclusion
Rehabilitation on implants in the aesthetic area is a very complex challenge that requires adequate analysis to select the ideal treatment plan for each specific case. The “dual zone” surgical concept integrates the concepts of minimizing and maintaining the original architecture of the peri-implant tissue in implants placed immediately, however, the use of this technique should be reserved for specific cases where the periodontal tissues of the tooth to extract are present in position, proportion, and quality, as in Elian´s type 1 sockets. In cases where the absence of structures such as the buccal table, absence of keratinized tissue in height or thickness, and in cases of combined defects, it is necessary to consider another type of surgical approach that allows the restoration of the absent tissues prior to implant placement.
Referencies
Chen ST, Buser D. (2014) Esthetic outcomes following immediate and early implant placement in the anterior maxilla—a systematic review. Int J Oral Maxillofac Implants. 29:186-215.
Morton D, Chen ST, Martin Wc, et al. (2014). Consensus statements and recommended clinical procedures regarding optimizing esthetic outcomes in implant dentistry. Int J Oral Maxillofac Implants. 29: 216-220.
Chen ST, Beagle J, Jensen SS, et al. (2009) consensus statements and recommended clinical procedures regarding surgical techniques. Int J Oral Maxillofac Implants. 24: 272-278.
Avila, G., Galindo-Moreno, P., Soehren, S., Misch, C. E., Morelli, T., & Wang, H. L. (2009). A novel decision-making process for tooth retention or extraction. Journal of periodontology, 80(3), 476–491.
McGuire M. K. (1991). Prognosis versus actual outcome: a long-term survey of 100 treated periodontal patients under maintenance care. Journal of periodontology, 62(1), 51–58.
Nunn, M. E., Fan, J., Su, X., Levine, R. A., Lee, H. J., & McGuire, M. K. (2012). Development of prognostic indicators using classification and regression trees for survival. Periodontology 2000, 58(1), 134–142
Zitzmann, N. U., Krastl, G., Hecker, H., Walter, C., Waltimo, T., & Weiger, R. (2010). Strategic considerations in treatment planning: deciding when to treat, extract, or replace a questionable tooth. The Journal of prosthetic dentistry, 104(2), 80–91
Elian, N., Cho, S. C., Froum, S., Smith, R. B., & Tarnow, D. P. (2007). A simplified socket classification and repair technique. Practical procedures & aesthetic dentistry: PPAD, 19(2), 99–106
Kan, J. Y., Roe, P., Rungcharassaeng, K., Patel, R. D., Waki, T., Lozada, J. L., & Zimmerman, G. (2011). Classification of sagittal root position in relation to the anterior maxillary osseous housing for immediate implant placement: a cone beam computed tomography study. The International journal of oral & maxillofacial implants, 26(4), 873–876
Seibert JS. (1983). Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. Part I. Technique and wound healing. Compend Contin Educ Dent. 4:437–453.
Misch CE, Judy KW. (1987). Classification of partially edentulous arches for implant dentistry. Int J Oral Implantol. 4:7–13.
Wang, H. L., & Al-Shammari, K. (2002). HVC ridge deficiency classification: a therapeutically oriented classification. The International journal of periodontics & restorative dentistry, 22(4), 335–343.
Levine RA, Ganeles J, Gonzaga L, et al. (2017). 10 Keys for Successful Esthetic-Zone Single Immediate Implants. Compend Contin Educ Dent. 38: 248-260.
Chu, S. J., Salama, M. A., Salama, H., Garber, D. A., Saito, H., Sarnachiaro, G. O., & Tarnow, D. P. (2012). The dual-zone therapeutic concept of managing immediate implant placement and provisional restoration in anterior extraction sockets. Compendium of continuing education in dentistry (Jamesburg, N.J.: 1995), 33(7), 524–534.
Seo, C. W., & Seo, J. M. (2017). A technique for minimizing subgingival residual cement by using rubber dam for cement-retained implant crowns. The Journal of prosthetic dentistry, 117(2), 327–328.
Araújo MG, Lindhe J. (2005) Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 32:212-218.
Kan JY, Morimoto T, Rungcharassaeng K, et al. Gingival biotype assessment in the esthetic zone: visual versus direct measurement. Int J Periodontics Restorative Dent. 2010;30(3):237-243.
Chappuis, V., Engel, O., Reyes, M., Shahim, K., Nolte, L. P., & Buser, D. (2013). Ridge alterations post-extraction in the esthetic zone: a 3D analysis with CBCT. Journal of dental research, 92(12 Suppl), 195S–201S.
Chappuis, V., Engel, O., Shahim, K., Reyes, M., Katsaros, C., & Buser, D. (2015). Soft Tissue Alterations in Esthetic Postextraction Sites: A 3-Dimensional Analysis. Journal of dental research, 94(9 Suppl), 187S–93S
Chappuis, V., Araújo, M. G., & Buser, D. (2017). Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000, 73(1), 73–83.
Araújo MG, Sukekava F, Wennström JL, Lindhe J. (2005). Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. J Clin Periodontol. 32:645-652.
Araújo MG, Linder E, Lindhe J. (2011). Bio-Oss collagen in the buccal gap at immediate implants: a 6-month study in the dog. Clin Oral Implants Res.22:1-8.
Blanco, J., Carral, C., Argibay, O., & Liñares, A. (2019). Implant placement in fresh extraction sockets. Periodontology 2000, 79(1), 151–167.
Qabbani, A. A., Razak, N., Kawas, S. A., Sheikh Abdul Hamid, S., Wahbi, S., & Samsudin, A. R. (2017). The Efficacy of Immediate Implant Placement in Extraction Sockets for Alveolar Bone Preservation: A Clinical Evaluation Using Three-Dimensional Cone Beam Computerized Tomography and Resonance Frequency Analysis Value. The Journal of craniofacial surgery, 28(4), e318–e325.
Tarnow, D., & Chu, S. (2019). The Single-Tooth Implant: Management of type 1 extraction sockets. Quintessence Publishing.
Al Qabbani, A., Al Kawas, S., A Razak, N. H., Al Bayatti, S. W., Enezei, H. H., Samsudin, A. R., & Sheikh Ab Hamid, S. (2018). Three-Dimensional Radiological Assessment of Alveolar Bone Volume Preservation Using Bovine Bone Xenograft. The Journal of craniofacial surgery, 29(2), e203–e209.
Zipprich, H., Miatke, S., Hmaidouch, R., & Lauer, H. C. (2016). A New Experimental Design for Bacterial Microleakage Investigation at the Implant-Abutment Interface: An In Vitro Study. The International journal of oral & maxillofacial implants, 31(1), 37–44.
Linkevicius, T., Apse, P., Grybauskas, S., & Puisys, A. (2009). The influence of soft tissue thickness on crestal bone changes around implants: a 1-year prospective controlled clinical trial. The International journal of oral & maxillofacial implants, 24(4), 712–719.
Vatėnas, I., & Linkevičius, T. (2021). One abutment one time vs. repeatable abutment disconnections in implants, restored with cemented / screw retained fixed partial dentures: Marginal bone level changes. A systematic review and meta-analysis. Stomatologija, 23(2), 35–40.
Linkevicius, T., & Vaitelis, J. (2015). The effect of zirconia or titanium as abutment material on soft peri-implant tissues: a systematic review and meta-analysis. Clinical oral implants research, 26 Suppl 11, 139–147
Chen ST, Buser D. (2014) Esthetic outcomes following immediate and early implant placement in the anterior maxilla—a systematic review. Int J Oral Maxillofac Implants. 29:186-215.
Morton D, Chen ST, Martin Wc, et al. (2014). Consensus statements and recommended clinical procedures regarding optimizing esthetic outcomes in implant dentistry. Int J Oral Maxillofac Implants. 29: 216-220.
Chen ST, Beagle J, Jensen SS, et al. (2009) consensus statements and recommended clinical procedures regarding surgical techniques. Int J Oral Maxillofac Implants. 24: 272-278.
Avila, G., Galindo-Moreno, P., Soehren, S., Misch, C. E., Morelli, T., & Wang, H. L. (2009). A novel decision-making process for tooth retention or extraction. Journal of periodontology, 80(3), 476–491.
McGuire M. K. (1991). Prognosis versus actual outcome: a long-term survey of 100 treated periodontal patients under maintenance care. Journal of periodontology, 62(1), 51–58.
Nunn, M. E., Fan, J., Su, X., Levine, R. A., Lee, H. J., & McGuire, M. K. (2012). Development of prognostic indicators using classification and regression trees for survival. Periodontology 2000, 58(1), 134–142
Zitzmann, N. U., Krastl, G., Hecker, H., Walter, C., Waltimo, T., & Weiger, R. (2010). Strategic considerations in treatment planning: deciding when to treat, extract, or replace a questionable tooth. The Journal of prosthetic dentistry, 104(2), 80–91
Elian, N., Cho, S. C., Froum, S., Smith, R. B., & Tarnow, D. P. (2007). A simplified socket classification and repair technique. Practical procedures & aesthetic dentistry: PPAD, 19(2), 99–106
Kan, J. Y., Roe, P., Rungcharassaeng, K., Patel, R. D., Waki, T., Lozada, J. L., & Zimmerman, G. (2011). Classification of sagittal root position in relation to the anterior maxillary osseous housing for immediate implant placement: a cone beam computed tomography study. The International journal of oral & maxillofacial implants, 26(4), 873–876
Seibert JS. (1983). Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. Part I. Technique and wound healing. Compend Contin Educ Dent. 4:437–453.
Misch CE, Judy KW. (1987). Classification of partially edentulous arches for implant dentistry. Int J Oral Implantol. 4:7–13.
Wang, H. L., & Al-Shammari, K. (2002). HVC ridge deficiency classification: a therapeutically oriented classification. The International journal of periodontics & restorative dentistry, 22(4), 335–343.
Levine RA, Ganeles J, Gonzaga L, et al. (2017). 10 Keys for Successful Esthetic-Zone Single Immediate Implants. Compend Contin Educ Dent. 38: 248-260.
Chu, S. J., Salama, M. A., Salama, H., Garber, D. A., Saito, H., Sarnachiaro, G. O., & Tarnow, D. P. (2012). The dual-zone therapeutic concept of managing immediate implant placement and provisional restoration in anterior extraction sockets. Compendium of continuing education in dentistry (Jamesburg, N.J.: 1995), 33(7), 524–534.
Seo, C. W., & Seo, J. M. (2017). A technique for minimizing subgingival residual cement by using rubber dam for cement-retained implant crowns. The Journal of prosthetic dentistry, 117(2), 327–328.
Araújo MG, Lindhe J. (2005) Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 32:212-218.
Kan JY, Morimoto T, Rungcharassaeng K, et al. Gingival biotype assessment in the esthetic zone: visual versus direct measurement. Int J Periodontics Restorative Dent. 2010;30(3):237-243.
Chappuis, V., Engel, O., Reyes, M., Shahim, K., Nolte, L. P., & Buser, D. (2013). Ridge alterations post-extraction in the esthetic zone: a 3D analysis with CBCT. Journal of dental research, 92(12 Suppl), 195S–201S.
Chappuis, V., Engel, O., Shahim, K., Reyes, M., Katsaros, C., & Buser, D. (2015). Soft Tissue Alterations in Esthetic Postextraction Sites: A 3-Dimensional Analysis. Journal of dental research, 94(9 Suppl), 187S–93S
Chappuis, V., Araújo, M. G., & Buser, D. (2017). Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000, 73(1), 73–83.
Araújo MG, Sukekava F, Wennström JL, Lindhe J. (2005). Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. J Clin Periodontol. 32:645-652.
Araújo MG, Linder E, Lindhe J. (2011). Bio-Oss collagen in the buccal gap at immediate implants: a 6-month study in the dog. Clin Oral Implants Res.22:1-8.
Blanco, J., Carral, C., Argibay, O., & Liñares, A. (2019). Implant placement in fresh extraction sockets. Periodontology 2000, 79(1), 151–167.
Qabbani, A. A., Razak, N., Kawas, S. A., Sheikh Abdul Hamid, S., Wahbi, S., & Samsudin, A. R. (2017). The Efficacy of Immediate Implant Placement in Extraction Sockets for Alveolar Bone Preservation: A Clinical Evaluation Using Three-Dimensional Cone Beam Computerized Tomography and Resonance Frequency Analysis Value. The Journal of craniofacial surgery, 28(4), e318–e325.
Tarnow, D., & Chu, S. (2019). The Single-Tooth Implant: Management of type 1 extraction sockets. Quintessence Publishing.
Al Qabbani, A., Al Kawas, S., A Razak, N. H., Al Bayatti, S. W., Enezei, H. H., Samsudin, A. R., & Sheikh Ab Hamid, S. (2018). Three-Dimensional Radiological Assessment of Alveolar Bone Volume Preservation Using Bovine Bone Xenograft. The Journal of craniofacial surgery, 29(2), e203–e209.
Zipprich, H., Miatke, S., Hmaidouch, R., & Lauer, H. C. (2016). A New Experimental Design for Bacterial Microleakage Investigation at the Implant-Abutment Interface: An In Vitro Study. The International journal of oral & maxillofacial implants, 31(1), 37–44.
Linkevicius, T., Apse, P., Grybauskas, S., & Puisys, A. (2009). The influence of soft tissue thickness on crestal bone changes around implants: a 1-year prospective controlled clinical trial. The International journal of oral & maxillofacial implants, 24(4), 712–719.
Vatėnas, I., & Linkevičius, T. (2021). One abutment one time vs. repeatable abutment disconnections in implants, restored with cemented / screw retained fixed partial dentures: Marginal bone level changes. A systematic review and meta-analysis. Stomatologija, 23(2), 35–40.
Linkevicius, T., & Vaitelis, J. (2015). The effect of zirconia or titanium as abutment material on soft peri-implant tissues: a systematic review and meta-analysis. Clinical oral implants research, 26 Suppl 11, 139–147
審美領域におけるインプラント治療は非常に複雑であり,個々の症例に対して適切な治療計画を選択するためには十分な診査が必要である.「デュアルゾーン」の概念は,インプラント即時埋入において,インプラント周囲組織の本来の形を維持することを目的とした考えから成り立っているが,それは,Elian’s type 1 socketのように,抜歯する歯の歯周組織が軟組織,硬組織ともに存在する限られた症例に限定されるべきである.インプラント体と唇側骨との空隙であるジャンピングディスタンスや付着歯肉が得られないとき,また複合的に組織の欠損を伴う症例では,インプラント埋入前に組織の欠損を補う別のタイプの外科的アプローチが必要である.
文献
Chen ST, Buser D. (2014) Esthetic outcomes following immediate and early implant placement in the anterior maxilla—a systematic review. Int J Oral Maxillofac Implants. 29:186-215.
Morton D, Chen ST, Martin Wc, et al. (2014). Consensus statements and recommended clinical procedures regarding optimizing esthetic outcomes in implant dentistry. Int J Oral Maxillofac Implants. 29: 216-220.
Chen ST, Beagle J, Jensen SS, et al. (2009) consensus statements and recommended clinical procedures regarding surgical techniques. Int J Oral Maxillofac Implants. 24: 272-278.
Avila, G., Galindo-Moreno, P., Soehren, S., Misch, C. E., Morelli, T., & Wang, H. L. (2009). A novel decision-making process for tooth retention or extraction. Journal of periodontology, 80(3), 476–491.
McGuire M. K. (1991). Prognosis versus actual outcome: a long-term survey of 100 treated periodontal patients under maintenance care. Journal of periodontology, 62(1), 51–58.
Nunn, M. E., Fan, J., Su, X., Levine, R. A., Lee, H. J., & McGuire, M. K. (2012). Development of prognostic indicators using classification and regression trees for survival. Periodontology 2000, 58(1), 134–142
Zitzmann, N. U., Krastl, G., Hecker, H., Walter, C., Waltimo, T., & Weiger, R. (2010). Strategic considerations in treatment planning: deciding when to treat, extract, or replace a questionable tooth. The Journal of prosthetic dentistry, 104(2), 80–91
Elian, N., Cho, S. C., Froum, S., Smith, R. B., & Tarnow, D. P. (2007). A simplified socket classification and repair technique. Practical procedures & aesthetic dentistry: PPAD, 19(2), 99–106
Kan, J. Y., Roe, P., Rungcharassaeng, K., Patel, R. D., Waki, T., Lozada, J. L., & Zimmerman, G. (2011). Classification of sagittal root position in relation to the anterior maxillary osseous housing for immediate implant placement: a cone beam computed tomography study. The International journal of oral & maxillofacial implants, 26(4), 873–876
Seibert JS. (1983). Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. Part I. Technique and wound healing. Compend Contin Educ Dent. 4:437–453.
Misch CE, Judy KW. (1987). Classification of partially edentulous arches for implant dentistry. Int J Oral Implantol. 4:7–13.
Wang, H. L., & Al-Shammari, K. (2002). HVC ridge deficiency classification: a therapeutically oriented classification. The International journal of periodontics & restorative dentistry, 22(4), 335–343.
Levine RA, Ganeles J, Gonzaga L, et al. (2017). 10 Keys for Successful Esthetic-Zone Single Immediate Implants. Compend Contin Educ Dent. 38: 248-260.
Chu, S. J., Salama, M. A., Salama, H., Garber, D. A., Saito, H., Sarnachiaro, G. O., & Tarnow, D. P. (2012). The dual-zone therapeutic concept of managing immediate implant placement and provisional restoration in anterior extraction sockets. Compendium of continuing education in dentistry (Jamesburg, N.J.: 1995), 33(7), 524–534.
Seo, C. W., & Seo, J. M. (2017). A technique for minimizing subgingival residual cement by using rubber dam for cement-retained implant crowns. The Journal of prosthetic dentistry, 117(2), 327–328.
Araújo MG, Lindhe J. (2005) Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 32:212-218.
Kan JY, Morimoto T, Rungcharassaeng K, et al. Gingival biotype assessment in the esthetic zone: visual versus direct measurement. Int J Periodontics Restorative Dent. 2010;30(3):237-243.
Chappuis, V., Engel, O., Reyes, M., Shahim, K., Nolte, L. P., & Buser, D. (2013). Ridge alterations post-extraction in the esthetic zone: a 3D analysis with CBCT. Journal of dental research, 92(12 Suppl), 195S–201S.
Chappuis, V., Engel, O., Shahim, K., Reyes, M., Katsaros, C., & Buser, D. (2015). Soft Tissue Alterations in Esthetic Postextraction Sites: A 3-Dimensional Analysis. Journal of dental research, 94(9 Suppl), 187S–93S
Chappuis, V., Araújo, M. G., & Buser, D. (2017). Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000, 73(1), 73–83.
Araújo MG, Sukekava F, Wennström JL, Lindhe J. (2005). Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. J Clin Periodontol. 32:645-652.
Araújo MG, Linder E, Lindhe J. (2011). Bio-Oss collagen in the buccal gap at immediate implants: a 6-month study in the dog. Clin Oral Implants Res.22:1-8.
Blanco, J., Carral, C., Argibay, O., & Liñares, A. (2019). Implant placement in fresh extraction sockets. Periodontology 2000, 79(1), 151–167.
Qabbani, A. A., Razak, N., Kawas, S. A., Sheikh Abdul Hamid, S., Wahbi, S., & Samsudin, A. R. (2017). The Efficacy of Immediate Implant Placement in Extraction Sockets for Alveolar Bone Preservation: A Clinical Evaluation Using Three-Dimensional Cone Beam Computerized Tomography and Resonance Frequency Analysis Value. The Journal of craniofacial surgery, 28(4), e318–e325.
Tarnow, D., & Chu, S. (2019). The Single-Tooth Implant: Management of type 1 extraction sockets. Quintessence Publishing.
Al Qabbani, A., Al Kawas, S., A Razak, N. H., Al Bayatti, S. W., Enezei, H. H., Samsudin, A. R., & Sheikh Ab Hamid, S. (2018). Three-Dimensional Radiological Assessment of Alveolar Bone Volume Preservation Using Bovine Bone Xenograft. The Journal of craniofacial surgery, 29(2), e203–e209.
Zipprich, H., Miatke, S., Hmaidouch, R., & Lauer, H. C. (2016). A New Experimental Design for Bacterial Microleakage Investigation at the Implant-Abutment Interface: An In Vitro Study. The International journal of oral & maxillofacial implants, 31(1), 37–44.
Linkevicius, T., Apse, P., Grybauskas, S., & Puisys, A. (2009). The influence of soft tissue thickness on crestal bone changes around implants: a 1-year prospective controlled clinical trial. The International journal of oral & maxillofacial implants, 24(4), 712–719.
Vatėnas, I., & Linkevičius, T. (2021). One abutment one time vs. repeatable abutment disconnections in implants, restored with cemented / screw retained fixed partial dentures: Marginal bone level changes. A systematic review and meta-analysis. Stomatologija, 23(2), 35–40.
Linkevicius, T., & Vaitelis, J. (2015). The effect of zirconia or titanium as abutment material on soft peri-implant tissues: a systematic review and meta-analysis. Clinical oral implants research, 26 Suppl 11, 139–147
Colocación inmediata de implantes en el área estética, consideraciones quirúrgicas y restaurativas
Fernando COLINDRES 1)Rodrigo RIVERA 1)Rodrigo CAYARGA 1)
1) Departamento de Implantología Avanzada, Facultad de Odontología, Universidad Francisco Marroquín, Guatemala.
I. Introducción
El sector estético representa un reto para el tratamiento rehabilitador sobre implantes dentales, debido a la alta incidencia de defectos de tejido blando y tejido óseo que hacen mandatorio el abordaje del tratamiento multidisciplinario con un equipo de clínicos cuyo curso de trabajo esté regido por un diagnóstico preciso y plan de tratamiento en etapas, quirúrgicas y restauradoras.1-3 Está bien descrito en la literatura que el punto de partida para resultados predecibles y exitosos es el diagnóstico inicial del problema que se quiere restaurar, por tanto, conocer la etiología del defecto a rehabilitar es imperativo para alcanzar los objetivos planificados en cada caso en particular. La documentación actual ofrece varias clasificaciones de defectos de acuerdo con la presencia de piezas dentales cuyo estado periodontal, endodóntico y/o protésico es no tratable,4-7 como la descrita por Elian et al,8 y Kan et al,9 y también se detallan clasificaciones de crestas óseas residuales cuya complejidad de tratamiento recae en el grado de pérdida de tejido óseo o blando presente.10-12 Generalmente las piezas dentales que deben ser reemplazadas en este sector presentan un nivel de complejidad alto en diferentes niveles, que pueden ser categorizados como factores de riesgo, Levine, et al.13 Determinaron que la primera clave del éxito para la colocación de implantes inmediatos en el área estética es la evaluación de riesgo estética de cada paciente, y es este análisis el que determinará la técnica quirúrgica, selección de materiales de regeneración, diseño, tipo y naturaleza de la restauración final. En este reporte de caso se presenta el protocolo utilizado para la rehabilitación protésica sobre un implante colocado de forma inmediata luego de extracción de una pieza con pronóstico no tratable en el sector anterior utilizando la técnica quirúrgica “dual zone therapeutic concept” descrita por Chu et al.14
II. Reporte de Caso
Paciente femenina de 22 años, sistémicamente sana sin historia de enfermedad periodontal, se presentó a la clínica de Implantología Avanzada de la facultad de odontología, Universidad Francisco Marroquín, con motivo de consulta de dolor en la pieza 8. A la evaluación clínica se evidenció cambio en la coloración de la corona provisional presente en dicha pieza, dolor a la palpación, sin exudado hemorrágico, a la remoción de la corona provisional se observó caries a nivel cervical con la presencia de una reconstrucción de muñón sostenida por un poste prefabricado. A la evaluación radiográfica se apreció un tratamiento de conductos radiculares deficiente con historia de apicectomía. Se hizo la interconsulta con el departamento de Endodoncia para evaluar la posibilidad de realizar una nueva cirugía periapical, con el departamento de Periodoncia y Restaurativa para evaluar la posibilidad de hacer una cirugía de alargamiento coronario funcional, sin embargo, debido a la proporción corono-radicular desfavorable, presencia de caries cervical y presencia de tratamientos endodónticos previos fallidos se concluyó que la mejor opción protésica era la extracción y colocación inmediata de implante en dicha área(Fig. 1).
(Fig. 1) A. Pieza 8 con corona provisional deficiente. B. Tratamiento de conductos radiculares deficiente. C. Alveolo tipo 1 según Elian et al,8 tipo 1 Kan et al.9
Se realizó exodoncia mínimamente traumática del diente 8 con periotomos, curetaje y desinfección del alvéolo, posteriormente se comprobó la integridad de la tabla ósea bucal y distancia entre margen gingival libre y placa bucal de 3 mm con sonda periodontal para proceder a la inmediata colocación del implante. Se colocó un implante de conexión cónica MIS C1 de 3,75 × 11,5mm con un torque de inserción de 45 Ncm. Además, se utilizó un pilar transmucoso MIS CONNECT de 4 mm con un torque de inserción de 30 Ncm para alejar la interfaz implante-pilar protésico de la cresta ósea marginal(Fig. 2).
(Fig. 2) A. Extracción mínimamente traumática B. Colocación de implante inmediato y aditamento transmucoso MIS CONNECT. C. Posición del implante final.
El implante se colocó en posición palatal respecto a las coronas clínicas de las piezas adyacentes, siguiendo el concepto de “dual zone” se realizó injerto óseo en el gap bucal entre implante y pared ósea bucal con xenoinjerto de partícula media hidratado en solución salina (Bonefill ® Dense [0,10 - 0,60mm] (Fine) 0,50 g • 0,50 cc. Bionnovation Biomedical, Bauru, Brasil.). Inmediatamente se realizó el provisional fijo sobre un pilar temporal PEEK sin contacto oclusal(Fig. 3).
(Fig. 3) A. Implante colocado en posición palatal. B. Xenoinjerto colocado en gap bucal de tejido óseo y tejido blando C. Corona provisional atornillada sin contacto oclusal.
Los cuidados postoperatorios incluyeron terapia antibiótica con Amoxicilina de 500mg. cada 8 horas por 7 días. Antiinflamatorios orales Dexketoprofeno de 25mg. Cada 8 horas por 5 días. Enjuagues con Gluconato de Clorhexidina al 0.12% 3 veces al día por 15 días. Recomendaciones sobre higiene oral en el área quirúrgica y comidas blandas. Se realizó un control postoperatorio a la primera semana, 15 días y al cabo de 4 meses se procedió a la etapa rehabilitadora(Fig. 4).
(Fig. 4) A. Situación postoperatoria a 1 semana. B. Corte tomográfico postoperatorio de 1 semana
Debido a la inclinación bucal del implante se decidió realizar una corona cementada utilizando un pilar protésico personalizado de zirconia. La corona definitiva se realizó de disilicato de litio EMAX (Ivoclar Vivadent AG, Liechtenstein), la cual fue cementada bajo el protocolo de cementación descrito por Seo & Seo.15 Se realizó un seguimiento a los 6 meses para corroborar la integridad de los tejidos periimplantarios y satisfacción de la paciente(Fig. 5).
(Fig. 5) A-B. Postoperatorio de 4 meses.
C-D Restauración final cementada.
E. Control radiográfico inmediato de cementación de corona final.
F. Control a los 6 meses posteriores a la rehabilitación protésica.
III. Discusión
La extracción de piezas dentales desencadena un proceso de cambios catabólicos dentro de los tejidos periodontales, dando como resultado disminución en la altura y grosor del tejido óseo disponible para la colocación de implantes dentales,16 así como problemas funcionales y estéticos para el paciente.17 El grado de reabsorción de los tejidos depende directamente del fenotipo periodontal, siendo fenotipos óseos finos, menores a 1 mm de grosor en tabla bucal, los más afectados en cuanto a pérdida progresiva de tejido tanto en altura como en grosor.18-20 Al realizar una extracción y colocación inmediata del implante, estos cambios catabólicos no son anulados, pero pueden ser modificados mediante biomateriales que actúen como andamio para la formación ósea en la interfase implante cresta residual.4, 21-23 La tasa de éxito de los implantes inmediates en comparación con los implantes colocados de manera convencional es similar, sin embargo en los primeros, los factores anatómicos presentes (tipo de fenotipo, presencia de patología periapical, tejido disponible), factores quirúrgicos (técnica quirúrgica, uso de injertos óseos, tejido conectivo) y factores protésicos (Provisionalización inmediata, tipo de material restaurador) juegan un papel clave para conseguir los objetivos del tratamiento a corto plazo, y más importante, a largo plazo.14, 23 El concepto “dual zone” aborda tres principios fundamentales para manejar alveolos tipo I según Elian et al., con el objetivo principal de minimizar y preservar la mayor cantidad de arquitectura periodontal existente en el sitio de tratamiento sobre implantes dentales.14, 23-25 Estos principios se definen como extracción mínimamente traumática de la pieza dental, colocación del implante sin elevación de colgajo mucoperióstico, en una ubicación tridimensional adecuada con uso de biomateriales en ambas zonas, de tejido blando y tejido óseo,26 y utilización de provisional fijo como dispositivo de sellado para contener el injerto óseo en su lugar. Este reporte caso fue realizado bajo los lineamientos de este concepto de dos zonas importantes de cambios dimensionales, así también se tomaron en cuenta conceptos importantes que se han descrito en la literatura con anterioridad para el éxito de la terapia sobre implantes dentales y mantenimiento de tejidos periimplantarios a largo plazo, como el uso de xenoinjerto como biomaterial de baja tasa de reabsorción y respuesta inflamatoria,22, 26 el empleo de conexión cónica y aditamento transmucoso MIS CONNECT para trasladar la interfase plataforma-pilar protésico de la cresta ósea marginal,27-29 y la selección de materiales restauradores inertes altamente estéticos.30 Es importante recalcar que la decisión de emplear una técnica quirúrgica depende de varios factores, de los cuales el diagnóstico inicial es clave para la predictibilidad del tratamiento. Dicho diagnóstico debe ser basado en la evaluación clínica y radiográfica detallada, etiología del defecto, estado sistémico, colaboración y requerimientos estéticos del paciente.
IV. Conclusión
La rehabilitación sobre implantes en el área estética es un reto muy complejo que requiere el análisis adecuado para seleccionar el plan de tratamiento ideal en cada caso específico. El concepto quirúrgico “dual zone” integra muy bien los conceptos de minimizar y mantener la arquitectura original del tejido periimplantario en implantes colocados de forma inmediata, sin embargo, la utilización de esta técnica debe reservarse para casos específicos en donde los tejidos periodontales del diente a extraer se encuentran presentes en posición, proporción y calidad, como en alveolos tipo 1 de Elian et al. En casos donde la ausencia de estructuras como la tabla bucal, ausencia de tejido queratinizado en altura o grosor, y en casos de defectos combinados es necesario considerar otro tipo de abordaje quirúrgico que permita el restablecimiento de los tejidos ausentes previo a la colocación del implante.
Bibliografía
Chen ST, Buser D. (2014) Esthetic outcomes following immediate and early implant placement in the anterior maxilla—a systematic review. Int J Oral Maxillofac Implants. 29:186-215.
Morton D, Chen ST, Martin Wc, et al. (2014). Consensus statements and recommended clinical procedures regarding optimizing esthetic outcomes in implant dentistry. Int J Oral Maxillofac Implants. 29: 216-220.
Chen ST, Beagle J, Jensen SS, et al. (2009) consensus statements and recommended clinical procedures regarding surgical techniques. Int J Oral Maxillofac Implants. 24: 272-278.
Avila, G., Galindo-Moreno, P., Soehren, S., Misch, C. E., Morelli, T., & Wang, H. L. (2009). A novel decision-making process for tooth retention or extraction. Journal of periodontology, 80(3), 476–491.
McGuire M. K. (1991). Prognosis versus actual outcome: a long-term survey of 100 treated periodontal patients under maintenance care. Journal of periodontology, 62(1), 51–58.
Nunn, M. E., Fan, J., Su, X., Levine, R. A., Lee, H. J., & McGuire, M. K. (2012). Development of prognostic indicators using classification and regression trees for survival. Periodontology 2000, 58(1), 134–142
Zitzmann, N. U., Krastl, G., Hecker, H., Walter, C., Waltimo, T., & Weiger, R. (2010). Strategic considerations in treatment planning: deciding when to treat, extract, or replace a questionable tooth. The Journal of prosthetic dentistry, 104(2), 80–91
Elian, N., Cho, S. C., Froum, S., Smith, R. B., & Tarnow, D. P. (2007). A simplified socket classification and repair technique. Practical procedures & aesthetic dentistry: PPAD, 19(2), 99–106
Kan, J. Y., Roe, P., Rungcharassaeng, K., Patel, R. D., Waki, T., Lozada, J. L., & Zimmerman, G. (2011). Classification of sagittal root position in relation to the anterior maxillary osseous housing for immediate implant placement: a cone beam computed tomography study. The International journal of oral & maxillofacial implants, 26(4), 873–876
Seibert JS. (1983). Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. Part I. Technique and wound healing. Compend Contin Educ Dent. 4:437–453.
Misch CE, Judy KW. (1987). Classification of partially edentulous arches for implant dentistry. Int J Oral Implantol. 4:7–13.
Wang, H. L., & Al-Shammari, K. (2002). HVC ridge deficiency classification: a therapeutically oriented classification. The International journal of periodontics & restorative dentistry, 22(4), 335–343.
Levine RA, Ganeles J, Gonzaga L, et al. (2017). 10 Keys for Successful Esthetic-Zone Single Immediate Implants. Compend Contin Educ Dent. 38: 248-260.
Chu, S. J., Salama, M. A., Salama, H., Garber, D. A., Saito, H., Sarnachiaro, G. O., & Tarnow, D. P. (2012). The dual-zone therapeutic concept of managing immediate implant placement and provisional restoration in anterior extraction sockets. Compendium of continuing education in dentistry (Jamesburg, N.J.: 1995), 33(7), 524–534.
Seo, C. W., & Seo, J. M. (2017). A technique for minimizing subgingival residual cement by using rubber dam for cement-retained implant crowns. The Journal of prosthetic dentistry, 117(2), 327–328.
Araújo MG, Lindhe J. (2005) Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 32:212-218.
Kan JY, Morimoto T, Rungcharassaeng K, et al. Gingival biotype assessment in the esthetic zone: visual versus direct measurement. Int J Periodontics Restorative Dent. 2010;30(3):237-243.
Chappuis, V., Engel, O., Reyes, M., Shahim, K., Nolte, L. P., & Buser, D. (2013). Ridge alterations post-extraction in the esthetic zone: a 3D analysis with CBCT. Journal of dental research, 92(12 Suppl), 195S–201S.
Chappuis, V., Engel, O., Shahim, K., Reyes, M., Katsaros, C., & Buser, D. (2015). Soft Tissue Alterations in Esthetic Postextraction Sites: A 3-Dimensional Analysis. Journal of dental research, 94(9 Suppl), 187S–93S
Chappuis, V., Araújo, M. G., & Buser, D. (2017). Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000, 73(1), 73–83.
Araújo MG, Sukekava F, Wennström JL, Lindhe J. (2005). Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. J Clin Periodontol. 32:645-652.
Araújo MG, Linder E, Lindhe J. (2011). Bio-Oss collagen in the buccal gap at immediate implants: a 6-month study in the dog. Clin Oral Implants Res.22:1-8.
Blanco, J., Carral, C., Argibay, O., & Liñares, A. (2019). Implant placement in fresh extraction sockets. Periodontology 2000, 79(1), 151–167.
Qabbani, A. A., Razak, N., Kawas, S. A., Sheikh Abdul Hamid, S., Wahbi, S., & Samsudin, A. R. (2017). The Efficacy of Immediate Implant Placement in Extraction Sockets for Alveolar Bone Preservation: A Clinical Evaluation Using Three-Dimensional Cone Beam Computerized Tomography and Resonance Frequency Analysis Value. The Journal of craniofacial surgery, 28(4), e318–e325.
Tarnow, D., & Chu, S. (2019). The Single-Tooth Implant: Management of type 1 extraction sockets. Quintessence Publishing.
Al Qabbani, A., Al Kawas, S., A Razak, N. H., Al Bayatti, S. W., Enezei, H. H., Samsudin, A. R., & Sheikh Ab Hamid, S. (2018). Three-Dimensional Radiological Assessment of Alveolar Bone Volume Preservation Using Bovine Bone Xenograft. The Journal of craniofacial surgery, 29(2), e203–e209.
Zipprich, H., Miatke, S., Hmaidouch, R., & Lauer, H. C. (2016). A New Experimental Design for Bacterial Microleakage Investigation at the Implant-Abutment Interface: An In Vitro Study. The International journal of oral & maxillofacial implants, 31(1), 37–44.
Linkevicius, T., Apse, P., Grybauskas, S., & Puisys, A. (2009). The influence of soft tissue thickness on crestal bone changes around implants: a 1-year prospective controlled clinical trial. The International journal of oral & maxillofacial implants, 24(4), 712–719.
Vatėnas, I., & Linkevičius, T. (2021). One abutment one time vs. repeatable abutment disconnections in implants, restored with cemented / screw retained fixed partial dentures: Marginal bone level changes. A systematic review and meta-analysis. Stomatologija, 23(2), 35–40.
Linkevicius, T., & Vaitelis, J. (2015). The effect of zirconia or titanium as abutment material on soft peri-implant tissues: a systematic review and meta-analysis. Clinical oral implants research, 26 Suppl 11, 139–147